Angiomyoma: An Unusual Diagnosis of Preauricular Swelling
Anamika Kashyap1, Smita Singh2, Kiran Agarwal3
1 Senior Resident, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
2 Associate Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
3 Director Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anamika Kashyap, Senior Resident, Department of Pathology, Lady Hardinge Medical College, New Delhi-110001, India.
E-mail: anamikakashyap25@gmail.com
Angiomyoma is a benign tumour arising from smooth muscle of blood vessel walls. These tumours are usually found in the lower extremities presenting as a painful mass. Angiomyoma of the preauricular area is rare, and only a few cases have been reported. Here, we report the case of a 56-year-old male patient with preauricular swelling for 30 years mimicking benign parotid neoplasm. A diagnosis of angiomyoma of the preauricular area was made on the basis of histopathology.
Benign, Smooth muscle, Vascular
Case Report
A 56-year-old male presented to Department of Surgery with complaint of painless swelling in left preauricular region for 30 years. The swelling had gradually increased in size with no history of any trauma or similar lesion on his body. His medical and family history were unremarkable. On clinical examination, lesion was 2×2 cm, soft, cystic, mobile, non-tender with unremarkable overlying skin. Clinical suspicion of benign parotid neoplasm was made. Fine Needle Aspiration Cytology (FNAC) was performed which yielded 0.2 mL clear fluid and showed mainly mature lymphoid cells along with few squamous cells with a suggestive diagnosis of lymphoepithelial lesion. The lesion was completely excised under local anaesthesia and sent for histopathology.
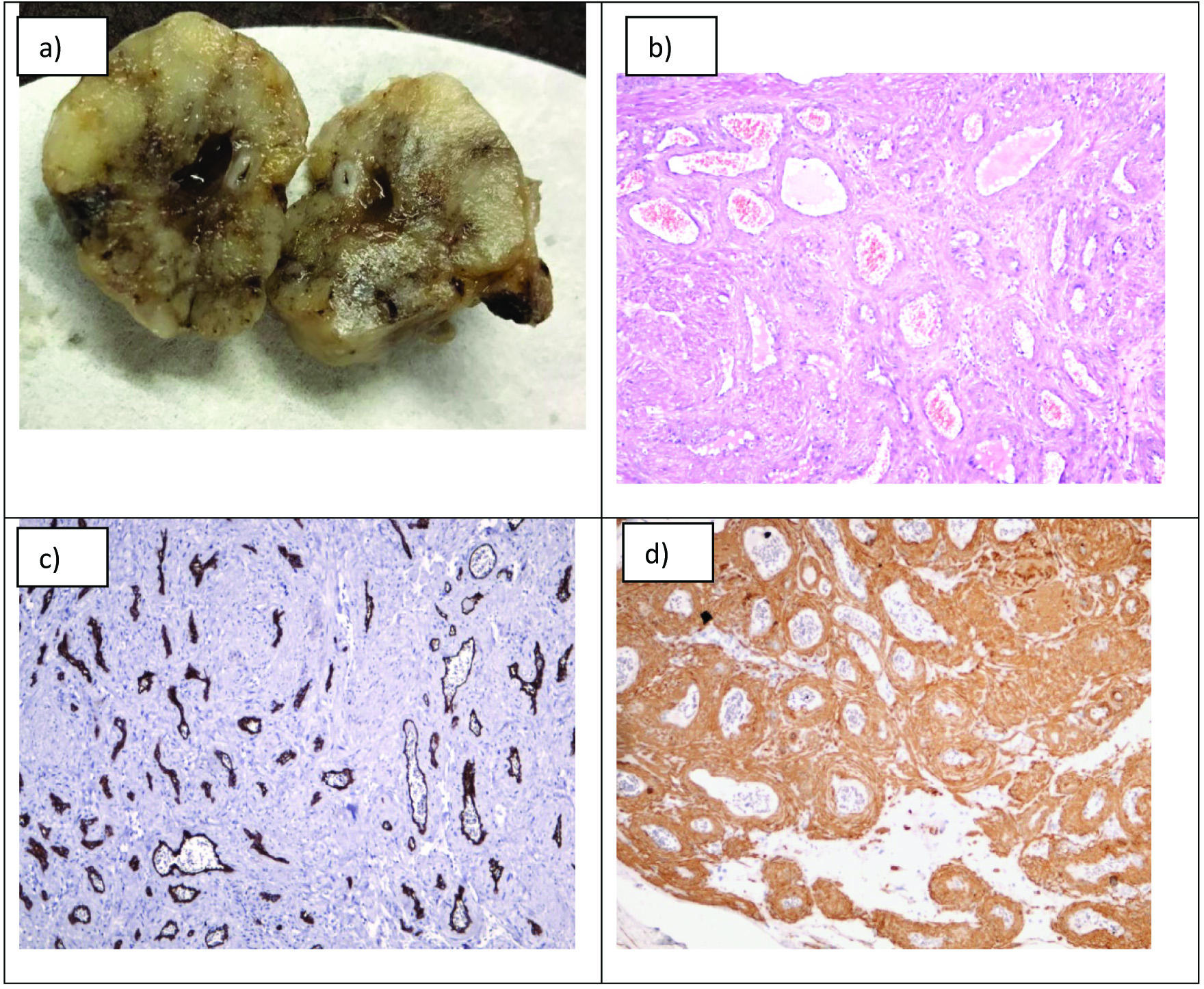
Grossly, the specimen was an 2×2×1.5 cm encapsulated, firm, grey-white to focally grey-brown, solid spherical mass with a single cyst of 0.6 cm diameter in center of lesion [Table/Fig-1a]. Microscopic examination revealed that the tumour was a well-defined nodule containing many thick-walled blood vessels blending with proliferative smooth muscle tissue. These vessels were lined by normal appearing endothelium [Table/Fig-1b]. No significant cellular atypia or mitotic activity was observed. On Immunohistochemistry (IHC) Smooth Muscle Actin (SMA) was found to be positive in smooth muscle around blood vessels (CD34 positive) [Table/Fig-1c,d]. Based on histological findings, the pathologic diagnosis of venous type of angiomyoma was made. Patient came for regular follow up and is presently doing well seven months post-surgery without requirement of any further treatment.
a) Gross finding- grey-white to grey-brown mass with a cyst in center; b) Thick-walled blood vessels surrounded by proliferative smooth muscle (H&E 10X); c) CD34 positive endothelial cells of vessels (IHC 10X); d) IHC- SMA positive proliferative smooth muscle (IHC 10X).
Discussion
Angiomyomas also termed as vascular leiomyoma are rare benign neoplasms of the soft tissue arising from the tunica media layer of blood vessels [1]. It has been hypothesised that pericytes (mesenchymal cells in small blood vessel wall) which have a phenotype between fibroblasts and vascular smooth muscle cells have an important role in the pathogenesis of this tumour. These cells can get differentiated into smooth muscle cells when stimulated by various inducing factors and form the progenitors in angiomyomas [2].
They usually occur in females aged 30-60 years and present as solitary, slow-growing nodule with pain seen in 60% of the cases. Angiomyomas occurs anywhere on the skin/subcutaneous tissue; the most common sites are the lower extremities (67%), upper extremities (22%), head and neck (8.5%), and trunk (2.5%) [3]. An angiomyoma in the auricular region has been reported in less than 3% of the 562 total cases of the head and neck region [4].
These tumours are capsulated, small, solitary, firm masses with no specific clinical presentation. Pain and tenderness is seen in 60% of cases and can be induced by exposure to wind, cold, local pressure, and other stimuli. Tumours occurring in the head and neck regions are usually not associated with pain [5]. Making a clinical diagnosis of angiomyoma in a preauricular mass a challenge and requires histopathological examination. Our case had a rare preauricular site of occurrence of angiomyoma with a long history of painless mass for 30 years in a 56-year-old male.
Several benign or malignant spindle cell tumours like fibroma, haemangioma, lymphangioma, hemangiopericytoma and myofibroma found in the preauricular area form their differential diagnosis. All these tumours are well circumscribed, grey-white nodules on gross examination.
Special stains like Masson’s Trichrome and immunohistochemical stains such as SMA and desmin can be helpful in reaching the final diagnosis. In our case, the immunohistochemical marker SMA and the tumour cells were found to be positive for SMA which led to the diagnosis of angiomyoma.
Angiomyomas are classified into three histological subtypes: 1) solid (closely compacted smooth muscle bundles); 2) venous (vessels have thick muscular walls that merge with smooth muscle bundles); and 3) cavernous (dilated vascular channels with minimal smooth muscle that merges with smooth muscle bundles) [1]. Solid angioleiomyomas occur most frequently in the lower extremities of women. The venous type tumour most frequently appears on the head and neck region and is generally found in men [1].
The treatment for angiomyoma is usually surgical excision to reduce the risk of malignancy and also for cosmetic reasons. Recurrence is extremely rare, regardless of the pathological subtype. However, cases of malignant changes and an association with a leiomyosarcoma have been reported [6].
Conclusion
The present case report describes angiomyoma at an unusual location of preauricular region mimicking parotid neoplasm. This lesion should be considered in the differential diagnosis of mass-like lesions of the preauricular region.
[1]. Ramesh P, Annapureddy SR, Khan F, Sutaria PD, Angioleiomyoma: A clinical, pathological and radiological reviewInt J Clin Pract 2004 58(1):587-91.10.1111/j.1368-5031.2004.00085.x15311559 [Google Scholar] [CrossRef] [PubMed]
[2]. Gerhardt H, Betsholtz C, Endothelial- pericyte interactions in angiogenesisCell Tissue Res 2003 314(1):15-23.10.1007/s00441-003-0745-x12883993 [Google Scholar] [CrossRef] [PubMed]
[3]. Choe KS, Sclafani AP, McCormick SA, Angioleiomyoma of the auricle: A rare tumourOtolaryngol Head Neck Surg 2001 125(1):109-10.10.1067/mhn.2001.11566311458228 [Google Scholar] [CrossRef] [PubMed]
[4]. Hachisuga T, Hashimoto H, Enjoji M, Angioleiomyoma. A clinicopathologic reappraisal of 562 casesCancer 1984 54(1):126-30.10.1002/1097-0142(19840701)54:1<126::AID-CNCR2820540125>3.0.CO;2-F [Google Scholar] [CrossRef]
[5]. Wirth GA, Sundine MJ, Kong AP, Carpenter PM, Auricular angioleiomyoma: A case report and review of the literatureEar Nose Throat J 2007 86(5):281-83.10.1177/01455613070860051217580807 [Google Scholar] [CrossRef] [PubMed]
[6]. Herren DB, Zimmermann A, Büchler U, Vascular leiomyoma in an index finger undergoing malignant transformationJ Hand Surg Br 1995 20(4):484-87.10.1016/S0266-7681(05)80158-5 [Google Scholar] [CrossRef]