Bilateral Lateral Rotation of Kidneys with Unilateral Cryptorchidism
Abhijit Jagdale1, Vinitkumar Deshmukh2, Bikash Parida3, Sumit Patil4, Sanjiv Thakur5
1 Assistant Professor, Department of Surgery, Byramjee Jeejeebhoy Medical College and Sassoon General Hospital, Pune, Maharashtra, India.
2 Senior Registrar, Department of Surgery, Byramjee Jeejeebhoy Medical College and Sassoon General Hospital, Pune, Maharashtra, India.
3 Assistant Professor, Department of Surgery, Byramjee Jeejeebhoy Medical College and Sassoon General Hospital, Pune, Maharashtra, India.
4 Associate Professor, Department of Anatomy, Andaman and Nicobar Islands Institute of Medical Sciences and GB Pant Hospital, Port Blair, Andaman and Nicobar, India.
5 Professor, Department of Surgery, Byramjee Jeejeebhoy Medical College and Sassoon General Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Abhijit Jagdale, S.N. 19, Gondhale Nagar Hadapsar, Pune-411028, Maharashtra, India.
E-mail: abhijitjagdale111285@gmail.com
Different types of renal anomalies like renal agenesis, ectopic kidney, horseshoe kidney, aberrant renal arteries are common. However, renal rotational anomalies are relatively rare. The present case is unique and may be the first reported case of bilateral renal lateral rotation with unilateral cryptorchidism. During embryological development, kidneys ascend from the sacral region to the lumbar region while the testis descend downwards laterally from lumbar region to iliac part of pelvis and then medially downwards to scrotal sac through inguinal canal. The path of descent of testis and ascent of kidneys are fixed. We assume that in this patient due to lateral rotation of the kidneys, the lateralised ureter might had obstructed the descent of the testis. Developmental anomaly of the kidneys like lateral rotation can arrest descent of testis and cause cryptorchidism.
Pelvis, Renal development, Testicular descent
Case Report
A 16-year-old male came with complaint of single testicle to General Surgery Outpatient Department (OPD) with no other significant complaints. He was born by full term normal delivery from non-consanguineous marriage. His other male sibling was normal. The consent was taken from the patient. On clinical examination, right hemiscrotum was poorly developed, left hemiscrotum and left testicle was normal. Examination of the inguinal region was normal. On ultrasonography, bilateral kidneys were malrotated with small echogenic soft tissue mass present below right kidney. In view of absent right testicle this infra renal echogenic soft tissue mass was mostly suggestive of undescended testis. Hence, Magnetic Resonance Imaging (MRI) was done for further clarification. On MRI in addition to undescended right testicle, there was bilateral malrotation of kidneys with hilum directed laterally [Table/Fig-1]. Left sided testicle was visualised in scrotal sac and was normal in size [Table/Fig-2]. Right sided testicle was adjacent to inferior pole of kidney and was small in size. Patient’s growth and development was normal with well developed secondary sexual characteristics. Haematological investigations and hormonal assays were normal. On laparoscopy, right testicle was found below inferior pole of right kidney and orchidectomy was done. Histopathological report was suggestive of atrophic testis with no evidence of malignancy [Table/Fig-3]. Patient recovered well from surgery and discharged on postoperative day three. Patient was advised follow up one month after the discharge and was normal during follow up visit.
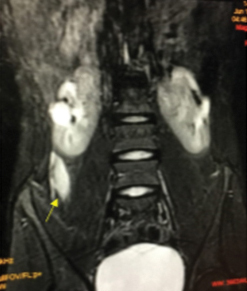
MRI image showing bilateral laterally rotated kidneys with right undescended testis below right kidney (yellow arrow).
MRI image showing normal left testicle (red arrow) and undescended right testicle (yellow arrow).

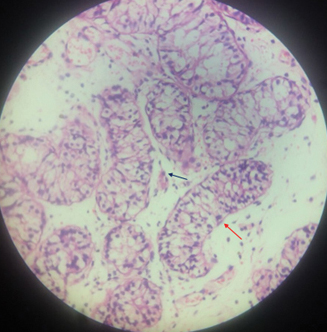
Histopathology image of undescended testis stained with Haematoxylin and Eosin showing atrophy of seminiferous tubules (red arrow) and prominent leydig cells (black arrow). Magnification 10X.
Discussion
Renal rotational anomalies can be of three types; 1) Nonrotation type; where renal pelvis is ventral; 2) Incomplete rotation; where renal pelvis is located ventromedially and 3) Reverse or excessive rotation; where renal pelvis is directed laterally. Reverse rotation is less commonly seen [1,2].
There are two case reports where there is lateral rotation of the bilateral kidneys. Both studies were on cadaveric females and were associated with abnormal renal vasculature [2,3].
In study done by Pappis CH et al., cryptorchidism and associated renal anomalies were studied in 144 patients, in which 36 patients were associated with renal abnormalities. Out of these 36 patients, 3 patients had renal malrotation, but type of malrotation was not specified [4]. Study done by Felton LM, in 61 cryptorchid boys, 12 patients had renal anomalies and of these 12, only two patients were found to have nonrotated kidney i.e., with ventral renal pelvis [5]. Grossman H and Ririe DG, studied urinary tract anomalies in 100 cryptorchid boys of which 78 patients had renal anomalies. Out of those 78 patients, only two patients had unilateral nonrotated kidney (with ventral pelvis) [6].
Considering above studies, it seems that though renal anomalies in cryptorchid boys are common but malrotation is rare and in malrotation, lateral malrotation is very rare. The present case is rare because not only one kidney but both kidneys were laterally rotated along with unilateral cryptorchidism.
During embryological development, kidneys ascend from the sacral region to the lumbar region while the testis descend downwards laterally from lumbar region to iliac part of pelvis and then medially downwards to scrotal sac through inguinal canal. Kidney also shows the medial 90° rotation, so that ventrally placed hilum comes on medial side. Ascent of the kidneys is associated with acquisition of the blood supply from the nearby vessel. When they are in pelvis blood supply is derived from iliac vessels. As they ascents, blood supply is derived from aorta with regression of former vessels. These different sources of blood supply during embryological development and non involution of vessels gives rise to multiple renal arteries which can be present in around 24% patients. Renal rotation precedes definitive vascularisation. Supplementary renal vessels are usual cause of rotational variations [7-9]. During the same period when there is ascent of the kidneys gonads descent from cranial location to caudal location with blood supply derived from abdominal aorta [3,10]. The cephalic end of primitive gonad (testis) is attached to the diaphragm through suspensory ligament. This ligament disappears in males while it persists in females as suspensory ligament of ovary. From caudal end of testis, fibro muscular band extends to scrotum called as gubernaculum testis, which guide the descend of testis [11]. Hormonal and mechanical factors act together for the normal descent of the testis in this hormonal factors include gonadotropins, testosterone, dihydrotestosterone and mullerian inhibiting factor. Mechanical factors include gubernaculum, epididymis, intra-abdominal pressure [12].
In this case, both kidneys failed to get medial rotation, instead they were laterally rotated. Due to this the hilum of kidney along with pelvis and ureter came on lateral side. Right testis might had failed to descent due to overlapping of upper part of right ureter on the superolateral part of right testis [Table/Fig-1,2]. Another possibility is that, due to malrotation of kidney, the ureter might had come on lateral side, which might had crossed the gubernaculum of testis resulting in undescended right testis. The left kidney ascends slightly higher than right kidney, so after malrotation left testis might not be trapped by upper part of ureter.
Impaired fertility is well recognised complication of undescended testis. There are 5-10 times more chances of malignancy in undescended testis than normal testis. There is no supportive data about reduction in chances of malignancy after orchiopexy, but obviously it is easier to identify malignancy of testis which is in scrotum [13]. There are high chances of patent processus vaginalis with undescended testis, but chances of hernia are much lower. Undescended testis is more prone to torsion. Laparoscopic Orchiopexy is standard treatment for the undescended testis. Histological changes are seen from age of one year and atrophy usually seen in puberty [13]. Diagnosis of the malrotated kidneys is done by Intravenous pylogram. Malrotated kidneys cause stasis of urine leading to stones, also they are difficult for manipulation during percutaneous nephrolithotomy and there is increased risk of visceral injury especially colonic injury [7].
Conclusion
During embryological development path of descent of testis and ascent of kidneys are fixed. Lateral rotation of the kidneys may affect descent of testis leading to undescended testis which is usually asymptomatic.
[1]. Ingole IV, Ghosh SK, Laterally rotated kidney-a rare congenital anomalyJ Anat Soc India 2005 54:19-21. [Google Scholar]
[2]. Gopinath V, Mookambika RV, Nair V, Nair RV, Rao M, Bilateral lateral rotation of the kidneys with their hilum facing laterally (outwards)-rare anatomical variationsAsian J Med Sci 2015 6(5):82-84.10.3126/ajms.v6i5.12414 [Google Scholar] [CrossRef]
[3]. Patil ST, Meshram MM, Kasote AP, Bilateral malrotation and lobulation of kidney with altered hilar anatomy: a rare congenital variationSurg Radiol Anat 2011 33(10):941-44.10.1007/s00276-011-0826-621626276 [Google Scholar] [CrossRef] [PubMed]
[4]. Pappis CH, Argianas SA, Bousgas D, Athanasiades E, Unsuspected urological anomalies in asymptomatic cryptorchild boysPediatric Radiology 1988 18(1):51-53.10.1007/BF023957602893330 [Google Scholar] [CrossRef] [PubMed]
[5]. Felton LM, Should intravenous pyelography be a routine procedure for children with cryptorchism or hypospadias?J Urol 1959 81(2):335-38.10.1016/S0022-5347(17)66021-X [Google Scholar] [CrossRef]
[6]. Grossman H, Ririe DG, The incidence of urinary tract anomalies in cryptorchid boysAm J Roentgenol 1968 103(1):210-13.10.2214/ajr.103.1.2104384938 [Google Scholar] [CrossRef] [PubMed]
[7]. Nathan H, Glezer I, Right and left accessory renal arteries arising from a common trunk associated with unrotated kidneysJ Urol 1984 132(1):07-09.10.1016/S0022-5347(17)49439-0 [Google Scholar] [CrossRef]
[8]. Braasch WF, Anomalous renal rotation and associated anomaliesJ Urol 1931 25(1):09-21.10.1016/S0022-5347(17)72818-2 [Google Scholar] [CrossRef]
[9]. Olsson O, Wholey M, Vascular abnormalities in gross anomalies of kidneysActa Radiologica Diagnosis 1964 2(5):420-32.10.1177/02841851640020050614210276 [Google Scholar] [CrossRef] [PubMed]
[10]. Gupta NP, Mishra S, Seth A, Anand A, Percutaneous nephrolithotomy in abnormal kidneys: single-center experienceUrology 2009 73(4):710-14.10.1016/j.urology.2008.10.07019193423 [Google Scholar] [CrossRef] [PubMed]
[11]. Datta AK, Essentials of Human Embryology 2010 6th edKolkataCurrent Books International:201-38. [Google Scholar]
[12]. Elder JS, Cryptorchidism: isolated and associated with other genitourinary defectsPediatric Clin North Am 1987 34(4):1033-53.10.1016/S0031-3955(16)36301-5 [Google Scholar] [CrossRef]
[13]. Williams NS, Bulstrode CJ, O’Connell PR, Bailey and Love’s Short Practice of Surgery 2013 26th edNew YorkCRC Press:1377-92. [Google Scholar]