Peritonitis due to Galactomyces geotrichum: A Rare Case Report
Anushka V Devnikar1, PM Beena2, A Bhaskaran3, MR Shivaprakash4
1 Assistant Professor, Department of Microbiology, S. Nijalingappa Medical College, Bagalkot, Karnataka, India.
2 Professor and Head, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
3 Professor, Department of Surgery, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
4 Additional Professor, Department of Microbiology, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anushka V Devnikar, Assistant Professor, Department of Microbiology, S. Nijalingappa Medical College, Navanagar, Bagalkot-587102, Karnataka, India.
E-mail: anushkad20@gmail.com
Galactomyces geotrichum is the teleomorphic stage of several unnamed Geotrichum species. They are filamentous yeast like fungi that are ubiquitous in nature. They have been isolated from various sources such as fruits, vegetables, plants and soil and are also found to be a part of the normal flora of the human gastrointestinal tract.
It is an emerging pathogen associated with superficial or disseminated infections in an immunocompromised host or in patients with debilitating diseases. This report describes an unusual case of peritonitis due to Galactomycesgeotrichum secondary to hollow viscus perforation in a young woman without any underlying co-morbidities.
Filamentous yeasts, Fungal peritonitis, Ubiquitous
Case Report
A 22-year-old woman came to the Emergency Department at tertiary care Hospital with abdominal pain since two days and no history of vomiting or loose stools. She was diagnosed with typhoid fever at a local clinic three weeks back and was treated with Cefixime 200 mg orally BD for five days. She had no other co-morbidities.
On examination, she had a pulse rate of 102 beats per minute and blood pressure of 100/70 mmHg. Examination of the abdomen revealed tenderness, guarding and rigidity. Bowel sounds were absent. Other systems were normal and WBC count was 10,100 cells/mm3 with neutrophilia (91%).
Based on these findings, a provisional diagnosis of peritonitis secondary to hollow viscus perforation was made and she underwent emergency exploratory laparotomy. Intra operatively, around 1000 mL of peritoneal fluid and whitish flakes covering the intestine and liver were noted and a pre pyloric perforation (0.5x1 cm) was discovered and repaired. The abdomen was closed with sub hepatic and pelvic drains in situ. The patient was started on empiric therapy of intravenous Piperacillin–Tazobactam 4.5 gm BD and Metronidazole 500 mg TID. In the post-operative period, the patient developed low grade fever and her general condition started deteriorating and the WBC count rose to 18,500 cells/mm3 with neutrophilia (88%). An ultrasound of the abdomen revealed mild to moderate ascites with no other significant findings.
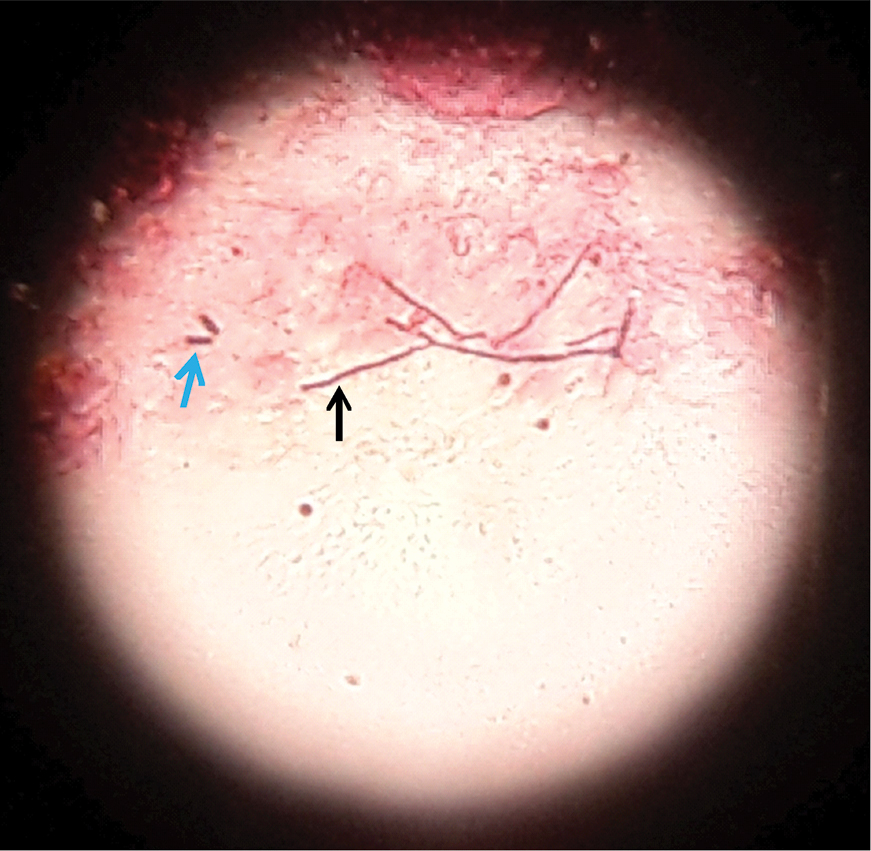
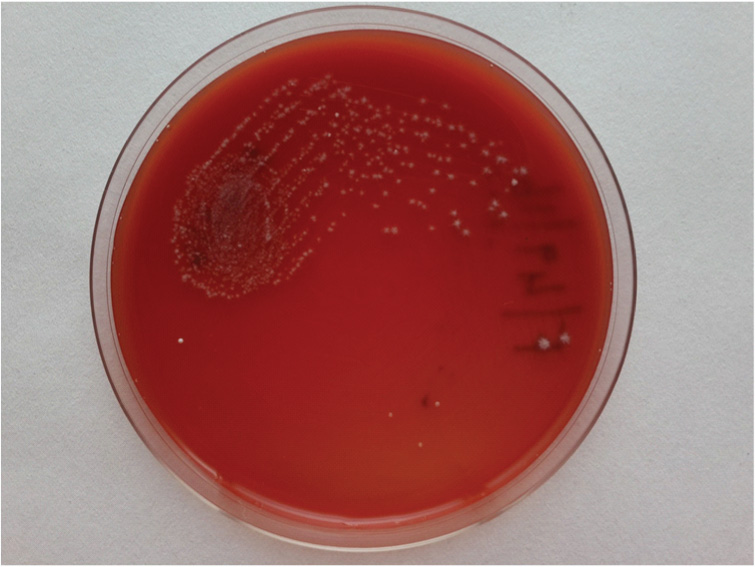
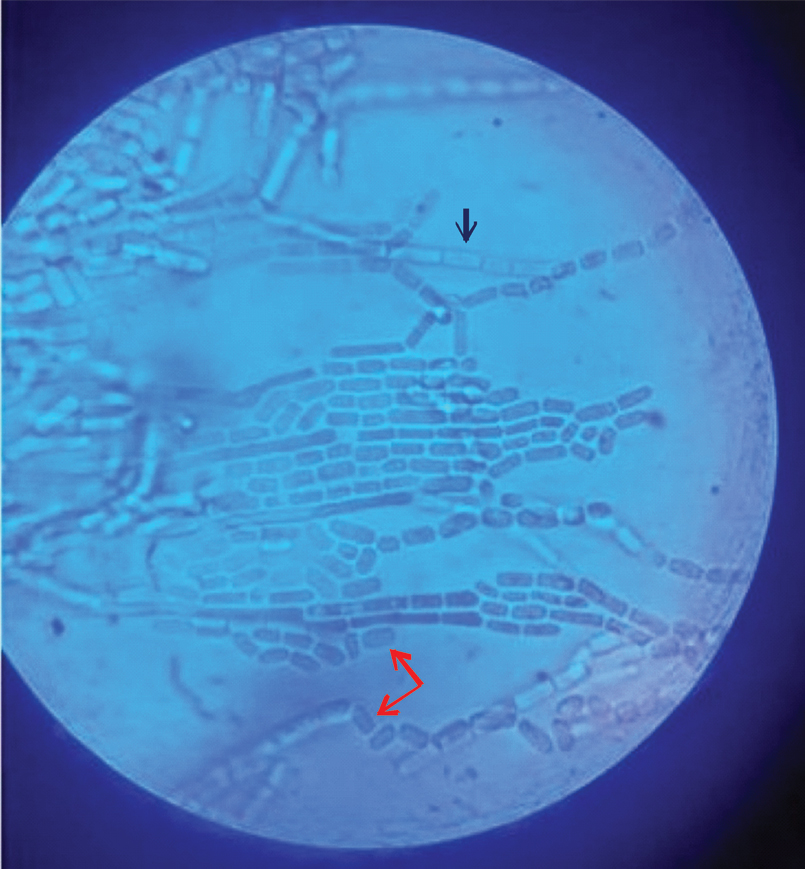
The peritoneal fluid that was collected intra operatively was sent for microbiological investigations. On gross examination, the fluid appeared turbid and brown with whitish flakes. Gram stain showed scanty pus cells and Gram positive fungal hyphae [Table/Fig-1]. Culture was done on Sabouraud’s dextrose agar and blood agar which yielded pure growth of dry, whitish, hairy colonies after 24 hours of incubation [Table/Fig-2]. Lactophenol Cotton Blue (LPCB) preparation of the isolate showed true septate hyphae, arthrospores and no blastospores [Table/Fig-3]. It was presumptively identified as Geotrichum species [1]. The identity of the isolate was confirmed by a negative urease test and assimilation of glucose, xylose and galactose on yeast nitrogen medium [2].
Direct gram stain showing gram positive fungal hyphae (black arrow) arthrospores (blue arrow) (100X).
Blood agar showing dry, white and spidery colonies of Geotrichum spp.
LPCB mount showing septate hyphae (black arrow) and arthroconidia (red arrow) (40X).
A second sample collected post operatively also yielded pure growth of Geotrichum species. Identification was further confirmed by amplification and sequencing of the D1/D2 domain of 26S rDNA at National Culture Collection of Pathogenic Fungi (NCCPF), Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Briefly, Genomic DNA was extracted from pure culture obtained from peritoneal fluid by phenol chloroform method [3]. D1/D2 region of 26S rDNA was amplified using the primers pairs NL-1 (5’-GCATATCAATAAGCGGAGGAAAAG-3’) and NL-4 (5’-GGTCCGTGTTTCAAGACGG-3’) (Sigma, Bengaluru, India). Amplified gene products were purified by a gel extraction kit (QIAquick; Qiagen, Bengaluru, India). Purified PCR products were sequenced using the big dye terminator cycle sequencing kit, version 3.1 (Applied Biosystems, Foster City, CA) and analysed on an ABI 3130 Genetic Analyzer (Applied Biosystems). The sequences were compared in the Gene Bank DNA database (http://www.ncbi.nlm.nih.gov/Genbank/index.html). The 26S rDNA sequence of our isolate had 99% (526/529) homology to type strain of Galactomyces geotrichum (ATCC® 34614™) (GenBank accession number GQ458034.1)
The patient was started on oral Itraconazole 100 mg OD. She became afebrile and started to improve. The remainder of her post operative stay was uneventful. She was discharged after one week with the advice to continue oral itraconazole for five weeks. On follow up visits, the patient had recovered completely.
Discussion
Geotrichum candidum and G. capitatum are reported in literature as rare pathogens of low virulence in humans. They are recognised to cause superficial skin infections, respiratory tract infections, oral infections or disseminated infections in patients with underlying predisposing factors such as diabetes, haematological malignancies or in patients undergoing chemotherapy for cancer [4,5]. Peritonitis due to Geotrichum species has occasionally been reported in patients with continuous ambulatory peritoneal dialysis [6]. However, peritonitis in the absence of underlying co-morbidities is uncommon.
In the present case report, Geotrichum species was considered as the causative agent of peritonitis as repeated culture yielded pure growth of the same organism [1] and the patient’s symptoms resolved only after treatment with itraconazole. It is probable that prior antibacterial therapy could have led to suppression of normal bacterial flora which subsequently led to overgrowth of the fungus, Galactomyces geotrichum which is found in the human gut [7,8]. Following perforation, the fungus could have entered peritoneal cavity and led to the development of peritonitis.
Earlier, the anamorph Geotrichumcandidum was included in Galactomyces geotrichum. In 2004, Hoog GS and Smith MT introduced Galactomyces candidus to accommodate Geotrichum candidum complex and Galactomyces geotrichum became a complex of several unnamed Geotrichum species [9,10]. It is conceivable that the cases of G. candidum in literature are over estimated because of possible misidentification due to the difficulties in speciation and confusion over the recent changes in taxonomy [6,10].
This case puts emphasis on emergence of Geotrichum species as a significant pathogen and the best of our knowledge this is the first case report of peritonitis due to Galactomyces geotrichum in an immunocompetent patient. This case also stresses that fungal aetiology should be considered early in the course of disease, especially in patients with history of taking broad spectrum antibacterial therapy or in those who do not respond to empirical antibacterial therapy. Early identification and appropriate therapy are essential for a successful outcome.
Conclusion
This report on Galactomyces geotrichum aids in increasing awareness of its ubiquity, to highlight the change in its taxonomy and to emphasize that high index of suspicion for fungal peritonitis along with early therapy will lead to successful outcomes.
[1]. Emmons CW, Binford CH, Utz JP, Kwon-Chung KJ, Medical Mycology 1977 3rd EdLondonHenry Kimpton Publishers:202-05. [Google Scholar]
[2]. Chander J, Textbook of Medical Mycology 2015 3rd EdDelhiMehta Offset Pvt Ltd:512 [Google Scholar]
[3]. Chakrabarti A, Rudramurthy S, Kale P, Hariprasath P, Dhaliwal M, Singhi S, Epidemiological study of a large cluster of fungaemia cases due to Kodamaeaohmeri in an Indian tertiary care centreClin Microbiol Infect 2014 20(2):O83-O89.10.1111/1469-0691.1233724004250 [Google Scholar] [CrossRef] [PubMed]
[4]. Girmenia C, Panago L, Martino B, D’Antonio D, Fanci R, Specchia G, Invasive infections caused by Trichosporon species and Geotrichum capitatum in patients with haematological malignancies: a retrospective multicentre study from Italy and review of literatureJ Clin Microbiol 2005 43(4):1818-28.10.1128/JCM.43.4.1818-1828.200515815003 [Google Scholar] [CrossRef] [PubMed]
[5]. Sfakianakis A, Krasagakis K, Stefanidou M, Maraki S, Koutsopoulos A, Kofteridis D, Invasive cutaneous infection with Geotrichum candidum – sequential treatment with amphotericin B and voriconazoleMed Mycol 2007 45(1):81-84.10.1080/1369378060093994817325948 [Google Scholar] [CrossRef] [PubMed]
[6]. Garcia-Agudo R, Garcia-Martos P, Clinical and microbiological aspects of fungal peritonitis in peritoneal dialysisNefrologia 2009 29(6):506-17. [Google Scholar]
[7]. Scanlan PD, Marchesi JR, Micro-eukaryotic diversity of the human distal gut microbiota: qualitative assessment using culture dependent and independent analysis of faecesISME J 2008 2(12):1183-93.10.1038/ismej.2008.7618670396 [Google Scholar] [CrossRef] [PubMed]
[8]. Hamad I, Sokhna C, Raoult D, Bittar F, Molecular Detection of Eukaryotes in a Single Human Stool Sample from SenegalPLoS ONE 2012 7(7):e4088810.1371/journal.pone.004088822808282 [Google Scholar] [CrossRef] [PubMed]
[9]. Hoog GS, Smith MT, Ribosomal gene phylogeny and species delimitation in Geotrichum and its teleomorphsStud Mycol 2004 50:489-515. [Google Scholar]
[10]. Hoog GS, Smith MT, Galactomyces Redhead & Malloch (1977). In: Kurtzman CP, Fell JW, Boekhout T, editorsYeasts, A taxonomic study 2011 Vol 25th edUSAElsevier:413-20.10.1016/B978-0-444-52149-1.00031-8 [Google Scholar] [CrossRef]