Penile Carcinoma in Young Age Masquerading as Mondor’s Disease
Pritesh Jain1, Debansu Sarkar2, Dilip Kumar Pal3
1 MCh Resident, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
2 Associate Professor, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
3 Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dilip Kumar Pal, Professor and Head, Department of Urology, Institute of Post Graduate Medical Education and Research, Kolkata-700020, West Bengal, India.
E-mail: urologyipgmer@gmail.com
A 26-year-old unmarried male presented with voiding difficulty and penile oedema, was initially diagnosed and treated for Mondor’s disease, which is a rare, benign, usually self-limiting pathology of anonymous origin. When he failed to respond to conservative management, a biopsy from glans penis was taken which revealed it to be moderately differentiated Squamous Cell Carcinoma (SCC). Apart from being an old man’s affliction, usual presentations of penile cancer range from ulcerative lesion to exophytic growth. Thus, its presentation as thrombosis of dorsal vein of penis is astounding as depicted in this case.
Penile cancer, Phimosis, Phlebothrombosis, Young adult
Case Report
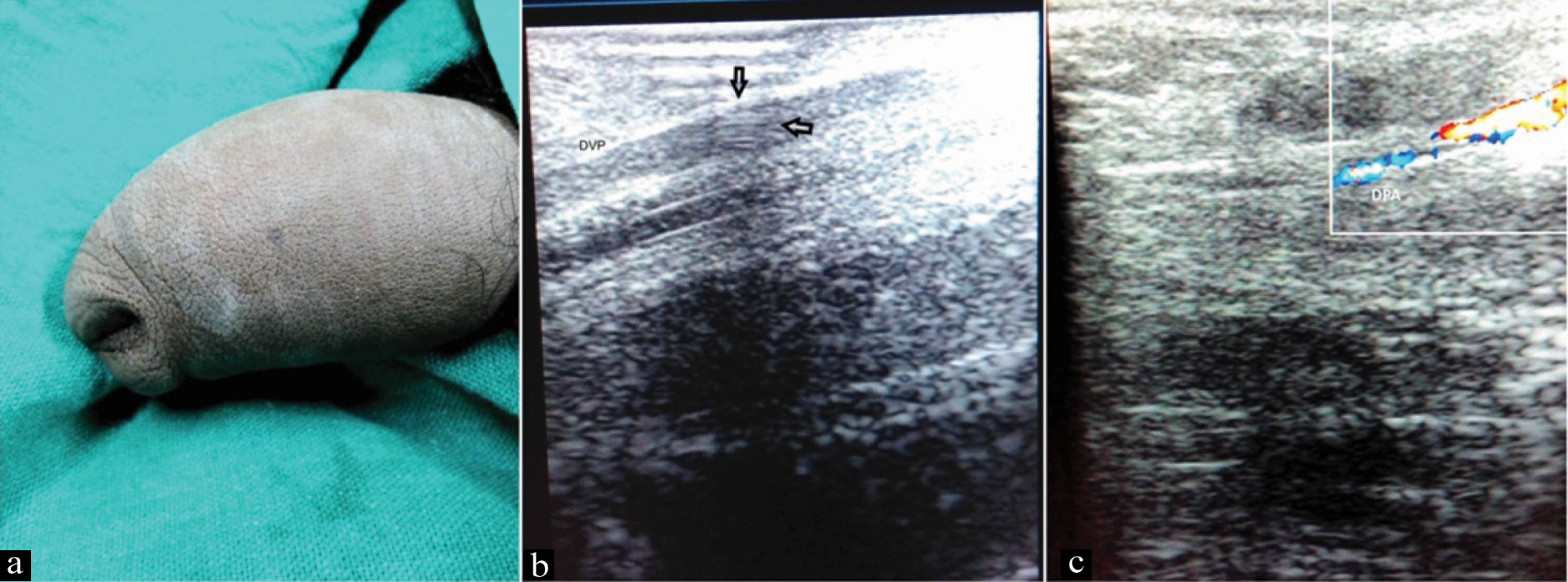
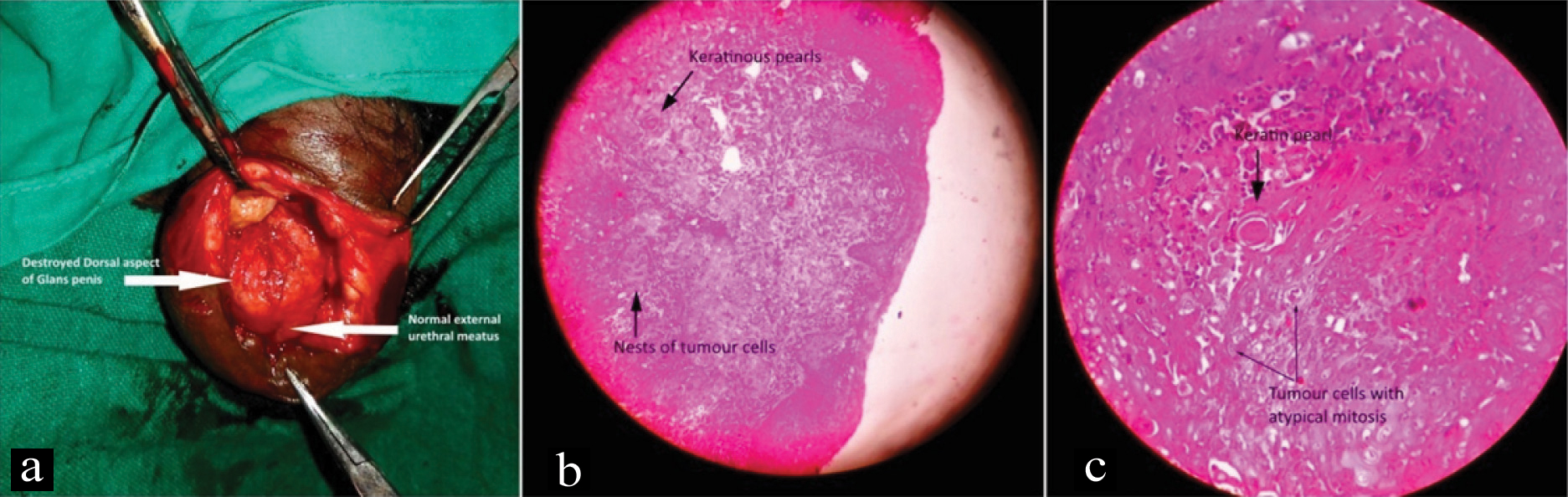
A 26-year-old unmarried male presented at our outpatient department with complaint of difficulty in voiding from childhood related to phimosis. From last 15 days he noticed penile oedema, pain and some hardness over dorsum of penis. He self-prescribed analgesics however when symptoms not relieved he consulted us. Local examination revealed penile oedema involving whole shaft of the penis along with phimosis [Table/Fig-1a]. On palpation of penis hard cord like structure was palpated at dorsum of the penis, without any lymphadenopathy. He denied history of trauma, aggressive sexual intercourse, masturbation or drug intake. Based on the clinical examination provisional diagnosis of penile vein thrombosis was made. Doppler ultrasound study of the penis confirmed the diagnosis with thrombus in dorsal vein of the penis, without any detectable flow in vein and normal flow in dorsal penile artery [Table/Fig-1b,c]. Ultrasonography of lower abdomen was normal. Laboratory tests including kidney function, liver function tests and coagulation profile all were within normal limits except total leucocyte count which were marginally raised. He was started on oral antibiotics and symptomatic treatment given however when symptoms didn’t respond to treatment, he was admitted and to relieve urinary obstruction under local anaesthesia dorsal slit was done. Approximately 25% of the dorsal aspect of the glans was found destroyed whereas external urethral meatus was found normal [Table/Fig-2a]. Based on suspicious findings imprint cytology and biopsy were taken from the suspected area over glans. Imprint cytology reported it as inflammatory, however biopsy revealed malignancy in form of moderately differentiated squamous cell carcinoma [Table/Fig-2b,c]. From the time patient presented to us there was a delay of approximately one month between provisional and final diagnosis. After diagnosis of penile carcinoma was made, with proper counselling penis preserving surgery (Partial penectomy) was done. Resected specimen margins were free of tumour and patient was doing well at four month of follow up.
a) Image of penis depicting oedema and phimosis; b) Penile ultrasound grey scale showing dilated dorsal vein of the penis with thrombus inside (arrow); c) Penile Doppler ultrasonography showing normal flow in dorsal penile artery.
a) Intraoperative image of penis depicting destroyed dorsal aspect of glans penis with normal external urethral meatus; b,c) Histopathology photomicrographs at (100x) and (400x) showing few keratinous pearls along with nests of cancer cells with atypical mitosis suggestive of moderately differentiated SCC.
Discussion
Mondor’s disease of the penis is a very rare and underreported disease, which was first described by Helm JD Jr and Hodge IG in 1958 [1]. It is a benign condition of the penis which might affect sexually active men of any age group [2]. Usual presentation of the disease is a palpable cord like structure over the penile shaft. Patient is usually asymptomatic but it may present with mild pain [3]. Most commonly involved vein is superficial dorsal vein of the penis; however involvement of circumflex veins has also been described in literature [4]. Multiple speculative aetiologies has been described like vigorous sexual intercourse, trauma, sexually transmitted infections, surgery of the pelvic region, certain haematological conditions like sickle cell disease, coagulation disorders etc., [3]. Most common implicating factor described was trauma associated with vigorous sexual intercourse. Diagnosis is made by proper history, physical examination revealing palpable cord like structure over dorsum and Doppler ultrasonography of penis revealing thrombus in the vein with decreased to absent blood flow [5]. In our case also there was palpable cord like structure which was confirmed to be thrombus in dorsal vein of the penis. Mondor’s disease of penis is a self-resolving condition however symptomatic treatment or use of anticoagulant may be required in certain cases. In rare cases lack of response to medical treatment may require surgery in form of thrombectomy and penile vein resection [2,6]. Penile cancer is an uncommon cancer with significant geographical variations such as in western countries it has an incidence of less than 1.00 per 100000 males [7,8]. Its incidence is strongly related to age and is highest in older age groups. An abrupt increase is encountered at 60 years which peaks at 80 years. However, the tumour is not unusual in younger men [8,9]. Phimosis due to chronic infection is described as one of the important risk factors for penile cancer [10]. Usual presentation of the disease is lesion over the penis however it can be hidden under the phimosis. In neglected cases it may present with ulcer or proliferative growth with distant metastasis with worse prognosis. Presentation of penile cancer with dorsal vein thrombosis of penis is bizarre. In our case because of phimosis from birth and typical finding of penile vein thrombosis the diagnosis was delayed. Early diagnosis of penile cancer is crucial especially in young patients to preserve sexual function and for favourable prognosis. We didn’t found this unusual presentation of penile carcinoma as Mondor’s disease of penis after a thorough search in various indexing agencies.
The importance of our case is that it highlights the atypical presentation of penile cancer in form of penile vein phlebitis and also associated phimosis which can delay the diagnosis and treatment of penile cancer apart from being a risk factor.
Conclusion
Phlebitis of dorsal penile veins may present with pelvic tumours but association with penile cancer has not been reported so far. Thus, one should be conscious of underlying malignancy even if presentation is of benign nature as in this case.
[1]. Helm JD Jr, Hodge IG, Thrombophlebitis of a dorsal vein of the penis: report of a case treated by phenylbutazone (Butazolidin)J Urol 1958 79(2):306-07.10.1016/S0022-5347(17)66273-6 [Google Scholar] [CrossRef]
[2]. Hamilton J, Mossanen M, Strote J, Mondor’s Disease of the penisWest J Emerg Med 2013 14(2):18010.5811/westjem.2012.8.1327623599866 [Google Scholar] [CrossRef] [PubMed]
[3]. Kumar B, Narang T, Radotra BD, Gupta S, Mondor’s disease of penis a forgotten diseaseSex Transm Infect 2005 81(6):480-82.10.1136/sti.2004.01415916326851 [Google Scholar] [CrossRef] [PubMed]
[4]. Arora R, Sonthalia S, Gera T, Sarkar R, Atypical penile Mondor’s disease – involvement of the circumflex veinInt. J STD AIDS 2015 26(5):360-63.10.1177/095646241453748224867818 [Google Scholar] [CrossRef] [PubMed]
[5]. Fitzgerald SW, Erickson SJ, Foley DW, Lipchik EO, Lawson TL, Color Doppler sonography in the evaluation of erectile dysfunctionRadiographics 1992 12(1):3-17.10.1148/radiographics.12.1.17344781734478 [Google Scholar] [CrossRef] [PubMed]
[6]. Al-Mwalad M, Loertzer H, Wicht A, Fornara P, Subcutaneous penile vein thrombosis (Penile Mondor’s Disease): pathogenesis, diagnosis, and therapyUrology 2006 67(3):586-88.10.1016/j.urology.2005.09.05416527584 [Google Scholar] [CrossRef] [PubMed]
[7]. Backes DM, Kurman RJ, Pimenta JM, Smith JS, Systematic review of human papillomavirus prevalence in invasive penile cancerCancer Causes Control 2009 20(4):449-57.10.1007/s10552-008-9276-919082746 [Google Scholar] [CrossRef] [PubMed]
[8]. Chaux A, Netto GJ, Rodríguez IM, Barreto JE, Oertell J, Ocampos S, Epidemiologic profile, sexual history, pathologic features, and human papillomavirus status of 103 patients with penile carcinomaWorld J Urol 2013 31(4):861-67.10.1007/s00345-011-0802-022116602 [Google Scholar] [CrossRef] [PubMed]
[9]. Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, Giuliano AR, Incidence trends in primary malignant penile cancerUrol Oncol 2007 25(5):361-67.10.1016/j.urolonc.2006.08.02917826651 [Google Scholar] [CrossRef] [PubMed]
[10]. Daling JR, Madeleine MM, Johnson LG, Schwartz SM, Shera KA, Wurscher MA, Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive diseaseInt J Cancer 2005 116(4):606-16.10.1002/ijc.2100915825185 [Google Scholar] [CrossRef] [PubMed]