Left coronary artery (LCA) originates from left posterior aortic sinus. Patency of left coronary artery is vital for sufficient perfusion of the heart. The left coronary artery supplies most of the left ventricle and considerable portion of right ventricle [1].
LCA bifurcates into left anterior descending and circumflex artery and passes between pulmonary trunk and left auricle. The left anterior descending artery (LAD) runs in the left anterior interventricular groove and ends at the apex or may run up to crux of the heart [2]. Circumflex artery (CX) then runs in the posterior atrioventricular groove and ends at the crux of heart by anastomosing with right coronary artery (RCA) or may end before the crux. Sometimes posterior interventricular artery may arise from circumflex artery and may run in the posterior interventricular groove as left coronary dominance [2].
The frequency of various anomalies of left coronary artery and the arterial dominance of the heart were observed in current study.
Materials and Methods
The Cross sectional observational study was conducted from September 2016 to November 2016. The study was carried out after obtaining ethical clearance from Institutional ethical committee. Fifty formalin fixed heart specimens of both sexes with intact coronary arterial pattern were studied. Specimens with damaged arterial pattern were excluded. The left coronary artery and their branches were carefully dissected out till their termination and were analysed for variable patterns.
Length of the arteries were measured with the help of thread and Vernier caliper from the point of origin of the arteries to the point of termination. The course of artery was delineated and thread was passed around the vessel. Then thread with mark was measured using the Vernier caliper. Percentage incidence of various patterns was recorded and tabulated.
Results
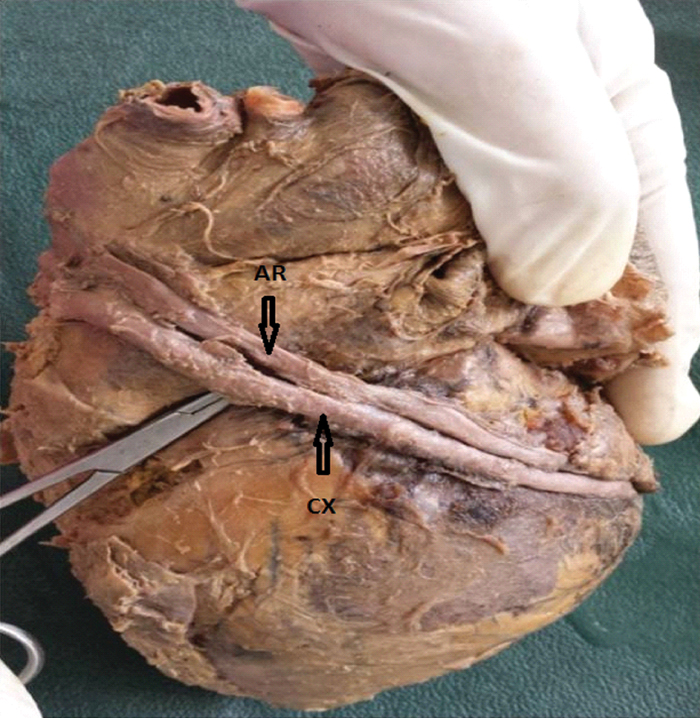
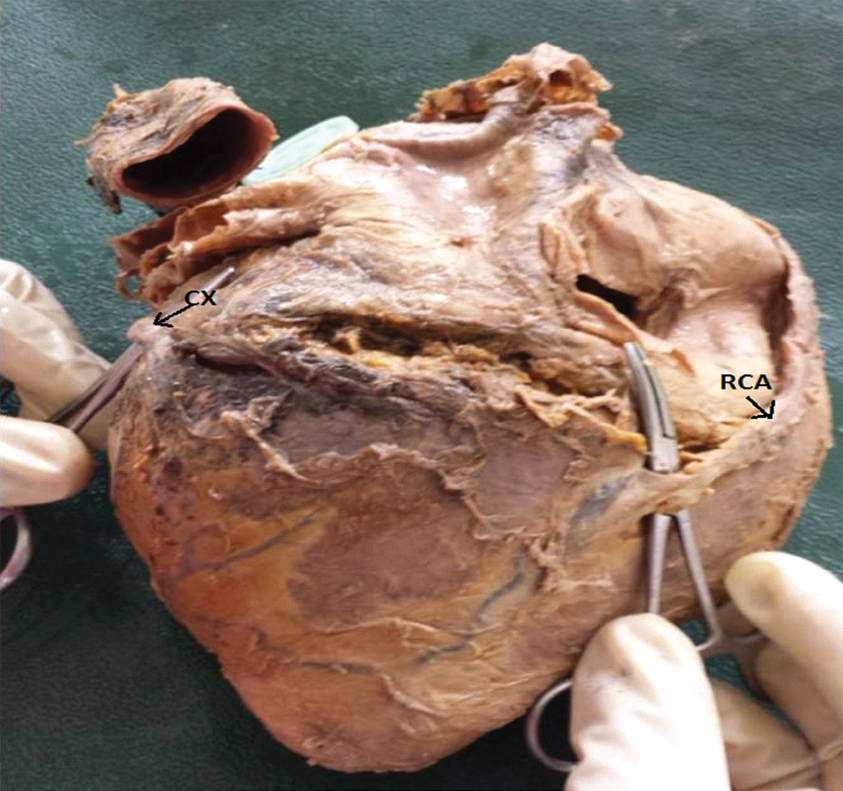
Left coronary artery was observed to originate from left posterior aortic sinus in forty nine heart specimens. In one specimen where there was absence of Left coronary arterial trunk. The Left Anterior Descending (LAD) artery and Circumflex artery (CX) were found to originate from left anterior aortic sinus [Table/Fig-1a]. It was coursing in front of pulmonary trunk and was found in the posterior atrioventricular groove. Parallel to this circumflex artery, another artery was found to originate from left anterior aortic sinus and had its course above the circumflex artery and ended in the left atrium in the same specimen [Table/Fig-1b and 1c]. Two ostias were found in the left anterior aortic sinus, one for the opening of CX and other for an artery which was found parallel to CX. [Table/Fig-1a,b and c].
Circumflex artery (CX) originating from left anterior aortic sinus. RCA-Right coronary artery.

Circumflex artery (CX) and an artery (AR) parallel to it.
Termination of Right Coronary artery (RCA) and Circumflex artery (CX).
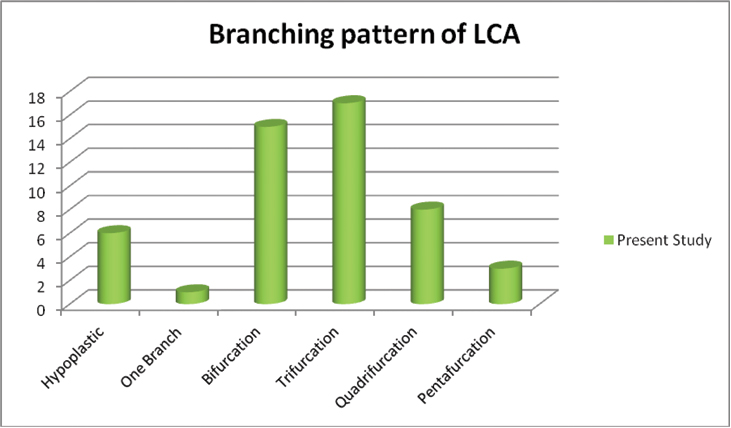
The main trunk of LCA showed variable branching pattern [Table/Fig-2]. Quadrifurcation of LCA was found in 8 (16%) specimens [Table/Fig-3] and pentafurcation was found in 3 (6%) of specimens [Table/Fig-4], however trifurcation was found in 17 (34%) cases. Hypoplastic (0.1–0.2 cm) left coronary arterial trunk was observed in six heart specimens (12%) [Table/Fig-5].
Branching pattern of Left coronary artery.
x-axis: Pattern observed, y-axis: number of specimens
Quadrifurcation of LCA (LCA–left coronary artery).

Pentafurcation of LCA (LCA–Left coronary artery).

Hypoplastic Left Coronary arterial (LCA) trunk.

In one specimen with hypoplastic LCA, LAD artery was crossed by a vein and had a fistulous communication between the artery and vein underneath the vein [Table/Fig-6]. Thin LAD with thick CX was found in one specimen [Table/Fig-7].
Fistula between Left anterior descending artery (LAD) and a vein.

Thin Left anterior descending artery (LAD) and thick Circumflex artery (CX).
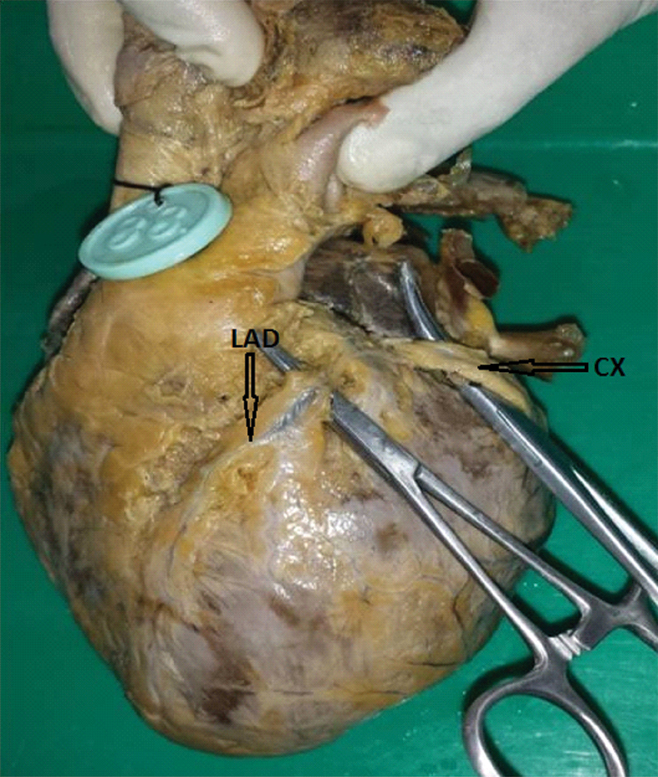
Circumflex artery was absent in one specimen where left coronary artery bifurcated into left anterior descending artery and diagonal artery and the branches of diagonal artery were found to supply circumflex territory [Table/Fig-8]. This was included as one of the bifurcation of LCA. The length of CX (1 cm in length) was very short in one specimen [Table/Fig-9].
Absence of Circumflex artery (CX), LCA–Left coronary artery and LAD–Left anterior descending artery.

Short length of Circumflex artery (CX).

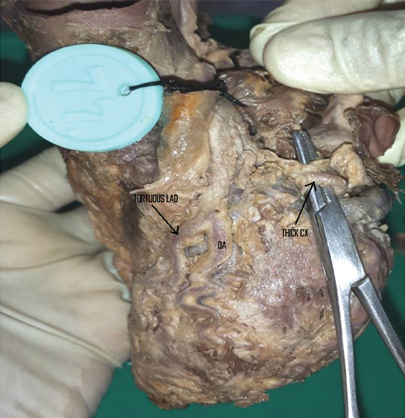
The variable pattern of termination of LAD in anterior and posterior interventricular groove is represented in [Table/Fig-10] and number of diagonal branches originating from it is shown in [Table/Fig-11]. Large circumflex artery (CX) with tortuous LAD and diagonal artery was observed in one specimen [Table/Fig-12]. The tortuous artery may reduce the blood flow through the artery.
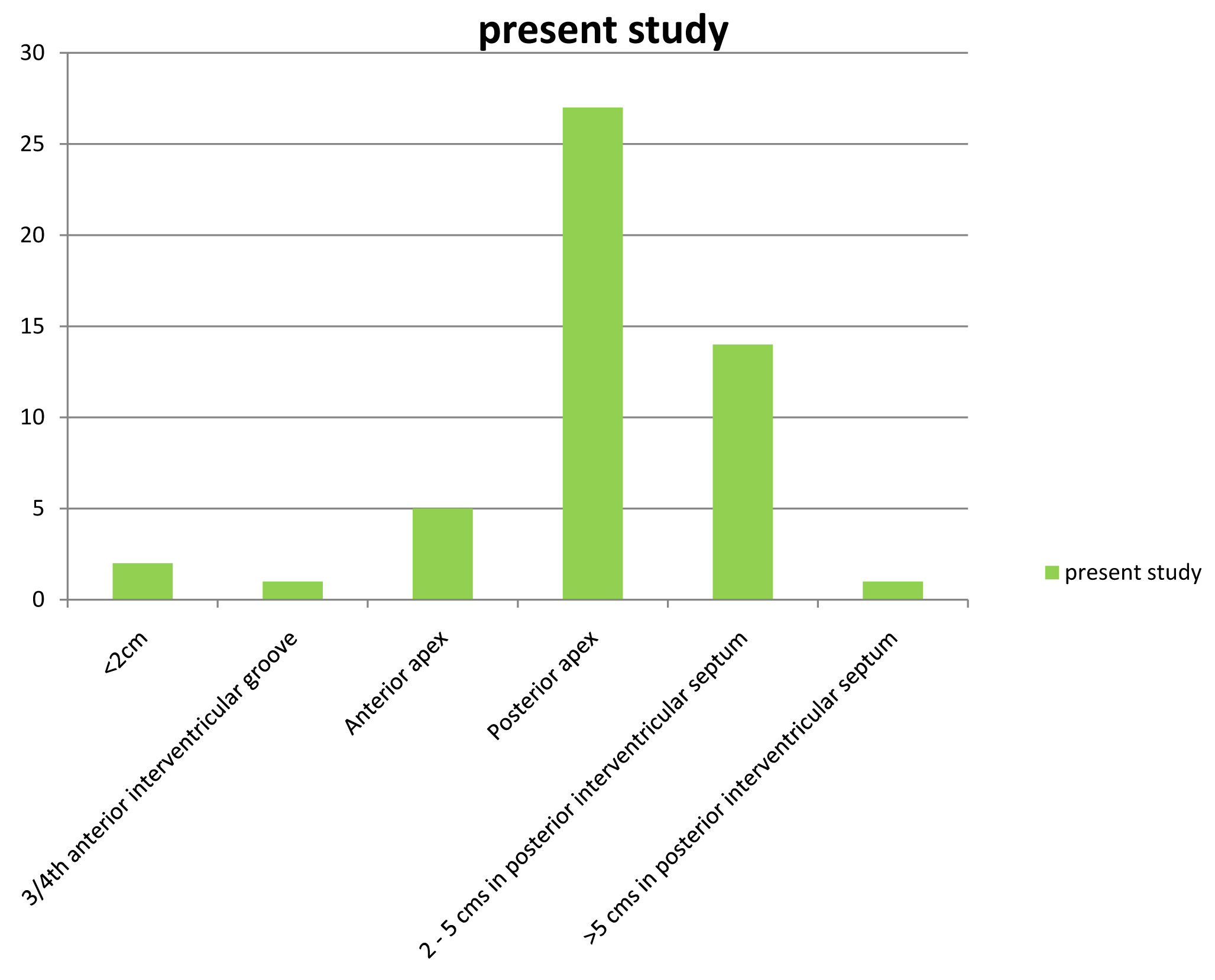
Termination of Left anterior descending artery.
x-axis: Level of termination of LAD, y-axis: Numer of specimens
Number of diagonal branches originating from left anterior descending artery.
| Number of diagonal branches orginating from LAD | Number (%) |
|---|
| 1 | 18 (36) |
| 2 | 29 (58) |
| 3 | 3 (6) |
| Total | 50 |
Thick circumflex artery (CX) and tortuous left anterior descending artery (LAD) and diagonal artery (DA).
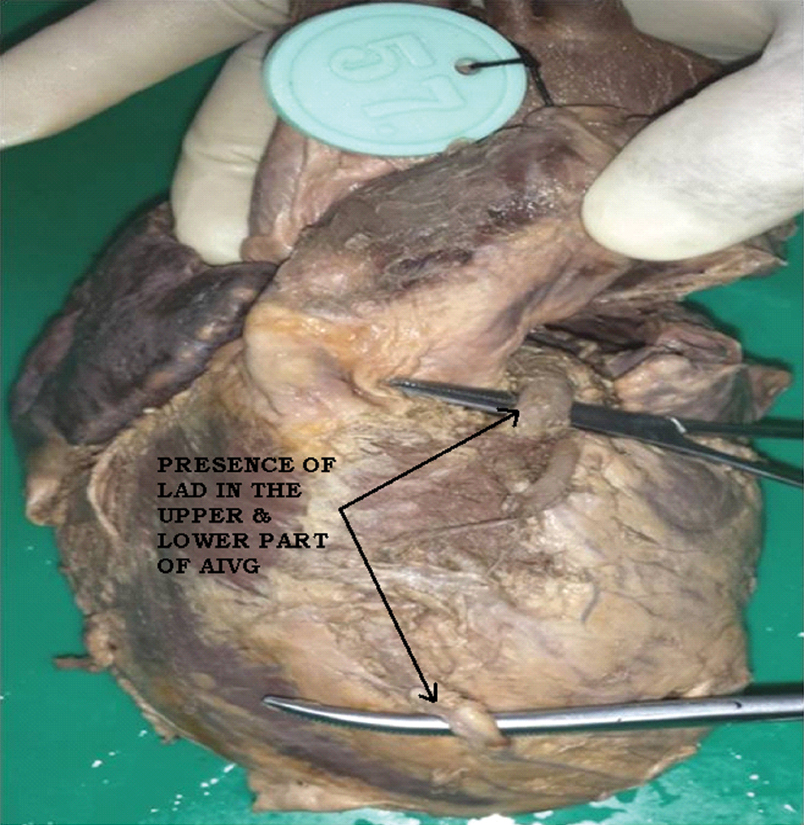
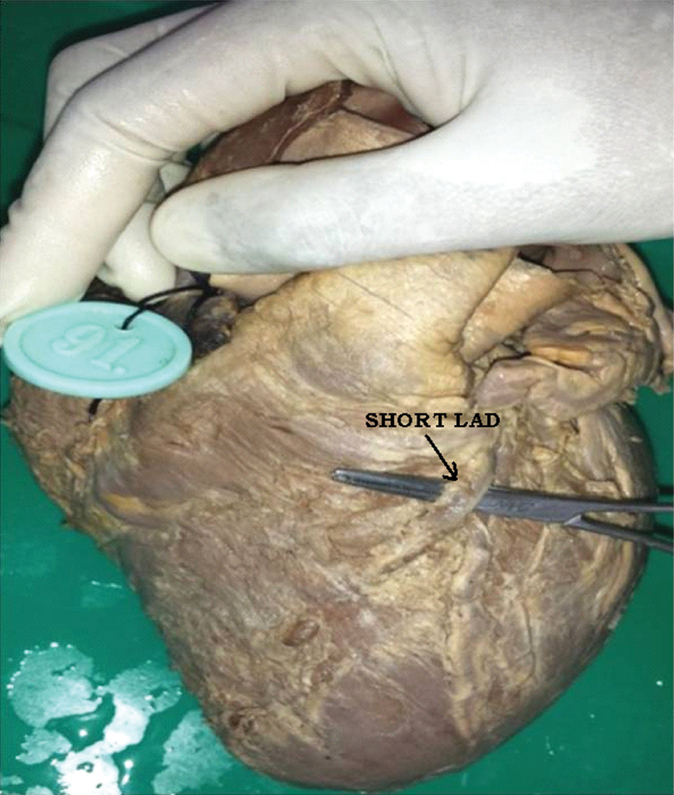
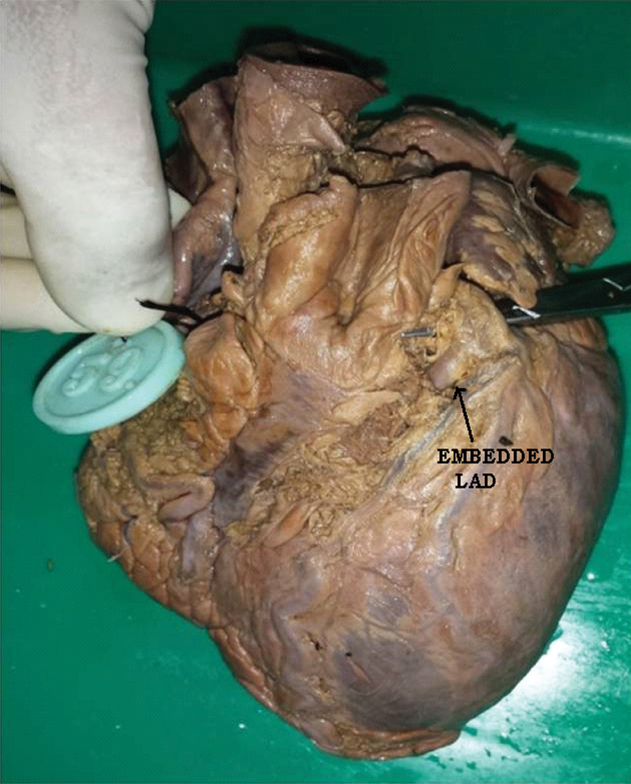
LAD was found to be discontinuous in two specimens due to presence of myocardial bridges [Table/Fig-13]. LAD was observed to have a short course (2 cm) in the anterior interventricular groove in one specimen [Table/Fig-14]. LAD was found to be embedded in the anterior atrioventricular groove in one specimen [Table/Fig-15].
Discontinuous left anterior descending artery (LAD), AIV–Anterior interventricular groove.
Short length of left anterior descending artery (LAD).
Embedded left anterior descending artery (LAD).
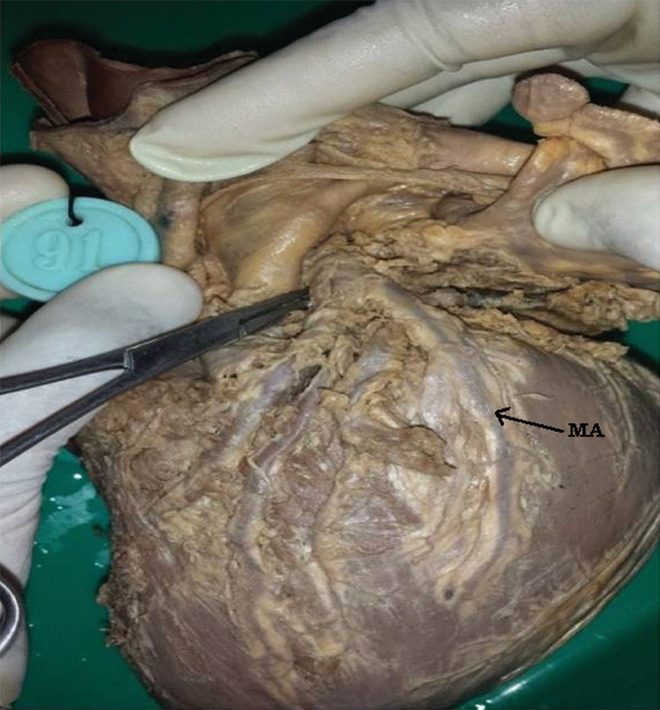
Kugel’s artery was found in three specimens which had its origin from Circumflex artery and coursed posterior to the atrial wall and was found to anastomose with an atrial branch of right coronary artery [Table/Fig-16]. A median artery which was found in seven specimens, was originating from left coronary artery and had a substantial calibre. It was found to extend half way down the free wall of the left ventricle [Table/Fig-17].

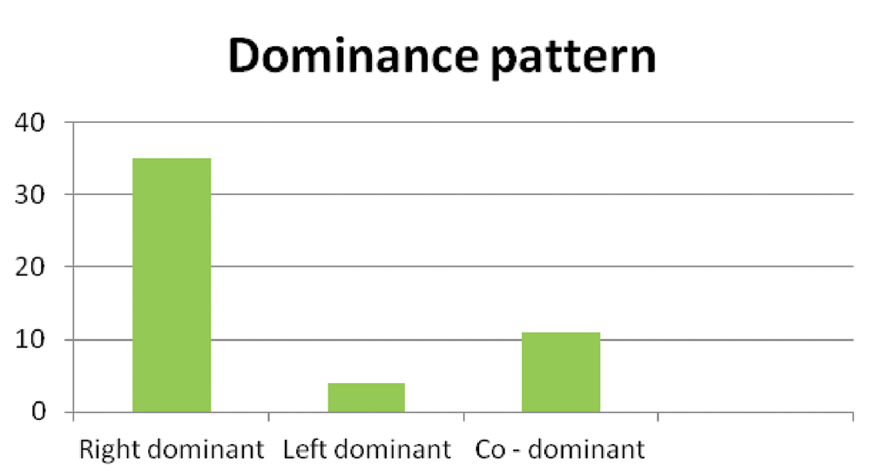
The dominance patter of heart was also studied whereby Left dominance was observed in 4 (8%) specimens. [Table/Fig-18,19].
Left dominance, PIA-Posterior interventricular artery, CX–Circumflex artery.

Dominance pattern of the heart specimens.
x-axis: Pattern oberved, y-axis: Number of Specimens
Discussion
Splanchnopleuric mesoderm contributes to all components of heart. The mesoderm contributes to the cardiogenic area that appears during 3rd week of embryogenesis. The cardiogenic area subsequently forms a pair of endocardial tubes which fuses to form primitive heart tube. Coronary arteries arise from appropriate differentiation of pluripotent cells into their respective anatomic and functional components. Anomalies of the coronary circulation result from processes that disrupt the normal differentiation and specialization of heart tube [5]. In particular, abnormal involution, position of endothelial buds or septation of truncus arteriosus may give rise to anomalous origin of coronary artery [6].
Coronary endothelial sprouts occur at around 5th week of Intrauterine life from the bulbous cordis which has not yet differentiated into the aorta and pulmonary trunk. The first evidence of coronary vessel development is the appearance of the blood islands at the beginning of the 5th week just under the epicardium in the sulci of the developing heart [6].
The incidence of Left main coronary artery anomaly ranges from 0.3 to 5.6%, the absence of left main artery is between 0.41 to 0.43% of cases [7]. But in our study, left coronary artery and left anterior descending artery were absent in one specimen in which circumflex artery was found to arise from left anterior aortic sinus.
The size, number and origin of coronary arteries and its branches may vary. Hypoplastic left coronary artery was found in six specimens (12%) which was slightly higher as compared to the study reported by Nordon DG et al., [8] where the incidence was 8%. Trifurcation of left coronary artery was comparable to similar study done by Kalpana R [3], Baptista CA [9] and Cavalcanti JS [10] [Table/Fig-20].
Comparative Division of main trunk of left coronary artery.
| Branch | Kalpana R [3] 2003 | Baptista CA [9] 1991 | Cavalcanti JS [10] 1995 | Present study 2017 |
|---|
| Hypoplastic | - | - | - | 12% |
| One branch | 1 | - | 1 | 2% |
| Bifurcation | 47 | 54.7 | 60 | 30% |
| Trifurcation | 40 | 38.7 | 38.18 | 34% |
| Quadrifurcation | 11 | 6.7 | - | 16% |
| Pentafurcation | 1 | - | - | 6% |
(In Percentage)
On comparison of termination of left anterior descending branch with the study by Kalpana R [3] and James TN [11], the left anterior descending artery with less than 2 cm size was found in two specimens of our study. The LAD had its course only in 3/4th of anterior interventricular groove in one specimen. The incidence of left anterior descending artery running up to posterior apex was found to be higher in our study (54%) when compared to Kalpana R (12%) [3] and James TN (23%) [11]. Earlier studies have reported highest incidence of left anterior descending artery coursing up to 2-5 cms in the posterior interventricular groove viz. 80% [3] and 42% [11] [Table/Fig-21].
| Termination of left anterior descending artery | Kalpana R [3] 2003 Number (%) | James TN [11] 1961 Number (%) | Present study Number (%) |
|---|
| <2 cm | - | - | 2(4) |
| 3/4th anterior interventricular groove (5-8 cm) | - | - | 1(2) |
| Anterior apex (9-11 cm) | 8(8) | 18(17) | 5(10) |
| Posterior apex (12-13 cm) | 12(12) | 24(23) | 27(54) |
| 2–5 cms in posterior interventricular septum (14-18 cm) | 80(80) | 44(42) | 14(28) |
| >5 cms in posterior interventricular septum (>19 cm) | - | 20(18) | 1(2) |
| Total | 100(100) | 106(100) | 50(100) |
The prevalence of absence of circumflex artery is about 0.6–1.3% [12] and in current study it was 2%. Absence of circumflex artery is usually associated with systolic click syndrome, dilated cardiomyopathy and acute myocardial infarction [13]. Termination of circumflex artery in our study when compared with Kalpana R [3] and James TN [11] was not similar where circumflex artery terminated at crux in 38% of specimen [Table/Fig-22].
Comparison of termination of circumflex artery.
| Point of termination | Kalpana R [3] 2003 Number (%) | James TN [11] 1961 Number (%) | Present study 2017 |
|---|
| Before obtuse margin (5-7 cm) | 3(3) | 1(1) | 4(8) |
| At obtuse margin (8-9 cm) | 13(13) | 22(20) | 8(16) |
| Between obtuse margin & crux (7-9 cm) | 67(67) | 64(67) | 9(18) |
| At crux (10-11 cm) | 6(6) | 9(9) | 19(38) |
| Beyond crux (>12 cm) | 11(11) | 9(9) | 9(18) |
| Not present | - | 1(1) | 1(2) |
Kugel’s artery was found in three specimens which had its origin from circumflex artery and coursed posterior to the left atrium and was found to have a communication with an atrial branch of right coronary artery. This artery is considered as an important collateral path for AV node [14].
Myocardial bridge is explained for the discontinuous left anterior interventricular artery. This bridge is the portion of myocardium that covers the artery. Contraction of these bridges may reduce the caliber of the artery by >75%. Hence myocardial bridges cause myocardial ischemia. They are risk factor for certain surgical interventions, in particular aorto–coronary bypasses that affect anterior interventricular artery. This is because the submerged portion of the artery is only a few millimeter from the right ventricle and there is a risk of perforation during surgical maneuvers to identify the artery [15].
Fistula between left anterior descending artery and a vein was observed in one specimen in our study. A coronary fistula is a direct communication between the coronary artery and the coronary sinus or one of its tributaries, the superior vena cava, the pulmonary artery or veins close to the heart or lumen of any cardiac chambers of the heart. New communications are said to be indicative of hypoxia, occlusive disease, valvular disease of the heart and anaemia [16].
Comparative observations of termination of posterior interventricular artery, originating from LCA is shown in [Table/Fig-23].
Point of Termination of Posterior interventricular artery was compared with other studies.
| Point of termination of posterior interventricular artery provided by LCA | Kalpana R [3] 2003 Number (%) | James TN [11] 1961 Number (%) | Present study 2017 |
|---|
| Hypoplastic LCA | - | - | 6(12) |
| ¼ way down PIVG (12-14 cm) | - | - | 1(2) |
| ½ way down PIVG (15-17 cm) | 7(7) | 5(5) | 1(2) |
| ¾ way down PIVG (18-20) | 4(4) | 3(3) | 3(6) |
| At apex (>20 cm) | - | 2(2) | 4(8) |
| Total | 11(11) | 10(10) | 15(30) |
PIVG-Posterior Interventricular Groove
Right dominance was found to be higher than other dominances in current study similar to earlier studies [Table/Fig-24]. The origin of posterior interventricular artery is one of the parameters on which Schlesinger’s system of arterial dominance was based. Coronary dominance is based on the origin of posterior interventricular artery. If it had its origin from right coronary artery, then it is termed as right dominance, if it had its origin from circumflex artery, it is termed as left dominance. If posterior interventricular artery had its origin from both the arteries, then it is termed as co–dominance [2].
Comparison of dominance of heart with the other studies.
| Dominance pattern (Posterior interventricular artery) | Kalpana R [3] (2003) | Cavalcanti JS [10] (1995) | Present study 2017 |
|---|
| Right | 89 | 88.18 | 35(70%) |
| Left | 11 | 11.82 | 4(8%) |
| Co–dominant | - | - | 11(22%) |
| Total | 100 | 100 | 50(100) |
(Values in percentage)
Knowledge of coronary artery anatomy and its variations are necessary for cardiothoracic surgeons and cardiologists for performing cardiac catheterization and coronary artery bypass surgery.
Limitation
As only fifty wet heart specimens were included, limited number of variations of left coronary artery were found. A histomorphometrical analysis could have been done in future to find out the exact luminal diameter of main trunk and its various branches.
Conclusion
Even though numerous variations in the branching pattern of the left coronary artery were reported earlier, some of the variations like fistula between left anterior descending artery and a vein, absence of left coronary arterial trunk and anterior descending artery with circumflex artery and a parallel vessel, absence of circumflex artery and Kugel’s artery are rare. These variations should be known to the cardiologists and cardiothoracic surgeons. These are of great importance in performing coronary angiography and bypass surgeries.
(In Percentage)
PIVG-Posterior Interventricular Groove
(Values in percentage)