The intracanal intricacies often restrict the comprehensive biomechanical preparation which is indispensible for long term endodontic success [1]. Certain infected root canals may depict internal resorptive defects, often arising due to pathologic course. The cells within the pulp differentiate into clastic type cells that resorb the dentin resulting in internal resorptive defect. These resorptive spaces are filled with granulation tissue alone or in combination with bone or cementum like mineralised tissues [2]. The internal resorption predominantly occurs in teeth with traumatic injuries, pulpitis, pulpotomy, tooth transplantation, restorative procedures, invagination and orthodontic treatment [3]. An early diagnosis and careful management of internal resorptive defects hold excellent prognosis [4]. Therefore, it is essential to completely eliminate the granulation tissue that is vested in the resorptive spaces [5]. The conventional endodontic instruments do not allow thorough cleaning of resorptive defects, therefore, the chemical dissolution of vital and necrotic pulp using NaOCl is clearly of great importance [6].
Other than CSNI, other several relatively newer techniques such as canal brush, sonic, passive ultrasonic agitation and Endo Vac devices are suggested that debride the internal resorptive defects more effectively. Such procedures augment the flow and distribution of irrigating solutions in this region, thus, resulting in fairly efficient disinfection [7].
A unique system, SAF (ReDent Nova, Ra’anana, Israel), in contrast to other rotary instruments, three dimensionally adapts to the dentinal walls of the root canal. The surface of its framework is slightly abrasive, which assists in canal preparation by vibrating and back and forth grinding motion [8]. Furthermore, the exclusive continuous irrigation system augments irrigant flow through the file [9]. The existing literature also endorses the better canal cleaning potential of SAF system when used in combination with NaOCl and Ethylenediaminetetraacetic Acid (EDTA) in long oval as well as C shaped canals [10,11].
Another innovative finishing instrument, the XP-endo finisher (XP) (FKG Dentaire, La Chaux de Fonds, Switzerland) based on the shape-memory principle of NiTi alloy, with a small core size 25 and no taper comprises of a C-shape arc in the apical half of the file [12]. It reportedly cleans the canal walls while preserving dentin. While activated, XP can diametrically expand up to 6 mm or 100 times more than its tip size [13]. Also, the shape of XP is temperature sensitive being straighter (Austenite phase) at room temperature and C shape arc form (Maretensite phase) at body temperature which on rotation mode allows better cleaning of difficult to reach canal details [14]. The file can be returned to its original straight shape manually once it is cooled. It is documented that their irregular designs will put these instruments in contact with more dentin than ordinary NiTi instruments [15,16].
The limited literature availability about the effectiveness of XP in removing the smear layer or intracanal medicament in simulated internal resorptive defects demands further researches that can justify their usage [12-14]. Therefore, the present study was aimed to evaluate the cleaning efficacy of XP from mechanically unreachable region like simulated IRR in the middle third of relatively straight root canals in comparison to the clinically recognised SAF or the conventional CSNI protocol. According to the null hypothesis, there should be no difference in the outcome of XP, SAF and CSNI in debriding the dentinal walls of internal resorptive defects.
Materials and Methods
This in vitro study was conducted in the Department of Conservative Dentistry and Endodontics, K. M. Shah Dental College and Hospital, Piparia, Vadodara, Gujarat, India, after obtaining the prior permission from the Institutional Ethics Committee. (Ethical Approval number-SVIEC/ON/Dent/SRP/16184). Total duration of the study was six months (October 2016 to March 2017).
A sample size of 30 achieved 80% power to detect an effect size (W) of 0.50 using a degree of freedom Chi-Square Test with a significance level (alpha) of 0.05000. Thirty freshly extracted human single rooted maxillary anterior teeth, extracted for periodontal reasons were collected from the Department of Oral and Maxillofacial Surgery. Teeth with caries, coronal restorations and root fillings, dilacerations, resorptions, any non-carious defect or fracture were excluded. All the teeth were disinfected by immersing the specimens in 0.1% thymol solution for one week followed by cleaning with ultrasonic scaler as per previously established protocol [17]. All the specimens were decoronated to obtain standardised root length of 12 mm. The apices were sealed with sticky wax to prevent the irrigant solutions from escaping through the apex to simulate in vivo situations. The canals were prepared using NiTi rotary files up till size 40 (0.06 taper) (K3 XFTM, Sybron Endo, USA). A 3% NaOCl solution was used as irrigant during instrumentation as well as during final rinse [18]. Each root canal was irrigated with 10 mL of distilled water to prevent the extended effects of the NaOCl solution. After biomechanical preparation of the root canals, internal resorption defects were simulated in each tooth.
Simulation of Internal Resorption
The simulation of internal resorptive defects was done as per the protocol suggested by da Silveira PF et al., [19]. All the prepared teeth were split mesiodistally using a diamond disk, generating two equal halves equidistant to the section line. Digital caliper was used to measure the root extensions. After determination of the root length, the middle third area were delimited and it was ensured that both the halves of the root were simulated at the same level. This measure was adopted to facilitate superimposition of the root sections. Composite resin (Filtek Z250; 3M ESPE, St Paul, MN) was used to prepare the cylindrical chamber (2 mm in diameter and 2 mm in height) which limited the application of nitric acid in each section. After the preparation of cylindrical chamber, distilled water was dispensed in the chamber to ensure the absence of fluid leakage [Table/Fig-1]. Nitric acid and NaOCl solutions were alternatively used to produce internal resorption by the demineralisation procedure. The cylindrical chamber was filled to its top with each respective substance. The plastic and disposable micropipettes were used to deliver solutions in the chamber. During the alternate use of two solutions distilled water was used to wash the chambers. Each demineralisation cycle comprised of 5% nitric acid solution for 12 hours, 8% NaOCl for 10 minutes followed by 5% nitric acid solution for 12 hours. Throughout, the internal resorption formation process, all the samples were placed at 1°C (+3°C). The protocol was performed for four days. At the end of the cycles, the resin cylindrical chamber was detached from the middle third of the root with orthodontic pliers [Table/Fig-2]. The root halves were then re-assembled using sticky wax along the junction of both sections over the entire root length. Thereafter, they were mounted in light body silicone filled in plexiglass tube.
Preparation of conduit designed cylindrical chamber to deliver fluids to the dentin surface in a controlled and restricted way using a micropipette.
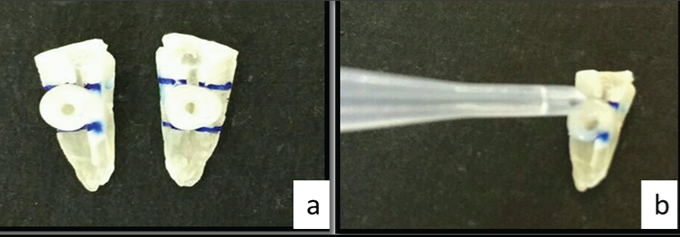
Arrow depicting simulated internal resorptive defect in a representative sample.

After storage for one week, the specimens were randomly allocated to three equal groups (n=10) according to the technique used for removal of smear layer. The randomisation of prepared specimen was done by Research Randomiser program [20].
CSNI Group
The canals were irrigated with 2 mL of distilled water followed by flushing the canals with 10 mL of 17% of EDTA solution with an in-and-out motion using the 27 gauge conventional needle and syringe and left in place for one minute per canal. All canals were then flushed with 10 mL of 3% NaOCl, which was again left in place for one minute per canal.
Self Adjusting File Group
For the SAF system, an in-and-out vibrating handpiece in combination with an RDT3 head (ReDent-Nova, Ra’nana, Israel), at a frequency of 5,000 movements per minute and amplitude of 0.4 mm were used. Throughout, the four minute of operation, canals were irrigated with 3% NaOCl through the hollow file. A VATEA peristaltic pump (ReDent-Nova, Ra’nana, Israel) provided continuous irrigation, at a rate of 4 mL per minute. This was followed by irrigation of canal with 2 mL of distilled water followed by flushing the canals with 10 mL of 17% of EDTA solution with passive and an in-and-out motion using the 27 gauge conventional needle and syringe and left in place for one minute per canal. This was followed by flushing of all canals with 10 mL of 3% NaOCl, which was again left in place for one minute per canal.
XP-Endo Finisher Group
A 5 mL of 3% NaOCl solution was used to rinse the specimens using a syringe and 27 gauge needle placed 1 mm from the working length with a flow rate of approximately 5 mL/minute. The XP-Endo finisher file with a torque controlled motor (X-Smart, Dentsply Sirona Ballaigues, Switzerland) operated at 800 rpm and the torque set to 1 Ncm, was used according to the manufacturer’s instructions. The rubber stopper was adjusted in a plastic tube to fix the working length, and according to manufacturer’s recommendations, the cold spray (Endo-Ice, Whaledent, Mahwah, NJ, USA) was used to cool the file inside the tube. The canal were filled with irrigant and then the XP file was inserted till the working length and operated for 60 seconds using slow and gentle 7–8 mm lengthwise in and out movements. New XP files were used after every three samples to maintain their efficiency. This was followed by flushing the canals with 10 mL of 17% of EDTA solution with an in-and-out motion using the 27 gauge conventional needle and syringe and left in place for one minute per canal. All canals were then flushed with 10 mL of 3% NaOCl, which were again left in place for one minute per canal.
Cleaning Efficacy Assessment
Scanning electron microscope (JEOL JSM-5610LV, JEOL INDIA Pvt. Ltd., New Delhi, India) was used for evaluation of cleaning efficacy. The SEM evaluation was carried out at Metallurgical and Materials Engineering Department, Faculty of Technology and Engineering, M.S. University, Vadodara, India. All the samples were demounted and both the halves were separated by removing the sticky wax. Thereafter, one of the halves was selected from each tooth using flip coin technique and coded. The coded specimens were mounted on metallic stubs and examined independently by single independent observers using SEM [7]. After general evaluation of the canal wall, SEM photomicrograph of the internal resorptive defect were captured at magnification of 500X and 1000X for evaluation of smear layer in accordance with the previous studies [8,21]. SEM images were inspected using inbuilt software in SEM assembly. The scoring system suggested by Parente JM et al., were modified and used to record the cleaning efficacy score [Table/Fig-3] [22]. An experienced independent blinded examiner evaluated and scored each image. Thereafter, the collected scores were tabulated [Table/Fig-4].
Description of debris/ smear layer score.
| Score | Description [23] |
|---|
| 1 | No debris/smear layer |
| 2 | 25% or more but less than 50% of tooth surface covered with debris / smear layer |
| 3 | 50% or more but less than 75% of tooth surface covered with debris/smear layer |
| 4 | 75% or more but less than 100% of tooth surface covered with debris/smear layer |
| 5 | 100% debris/smear layer covering the complete root canal wall |
CSNI-Conventional Syringe Needle Irrigation, SAF-Self-Adjusting File
Debris/smear layer score.
| S No. | Group A | Group B | Group C |
|---|
| CSNI | SAF | XP ENDO Finisher |
|---|
| 1 | 4 | 3 | 3 |
| 2 | 4 | 2 | 3 |
| 3 | 3 | 2 | 2 |
| 4 | 4 | 3 | 3 |
| 5 | 3 | 3 | 2 |
| 6 | 4 | 2 | 3 |
| 7 | 4 | 3 | 3 |
| 8 | 4 | 2 | 2 |
| 9 | 3 | 3 | 3 |
| 10 | 4 | 2 | 3 |
| Average | 3.7 | 2.5 | 2.7 |
Statistical Analysis
The collected data were subjected to one-way ANOVA test to obtain mean scores of the group and inter relationship between different groups was obtained using Post-hoc Tukey’s test.
Results
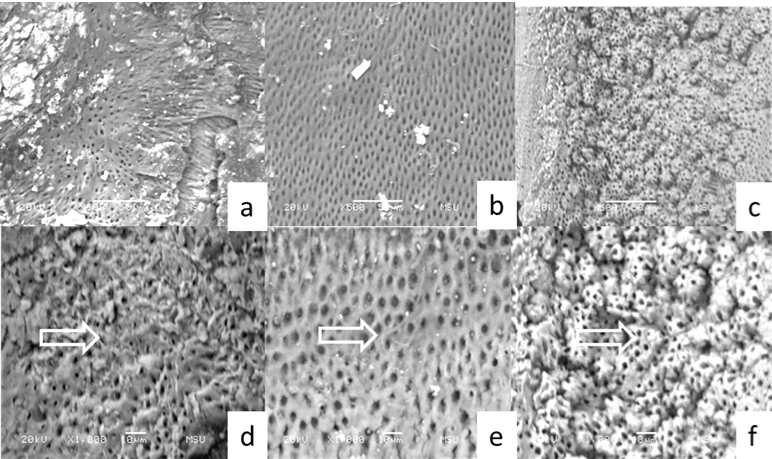
Although, most of the samples amongst the tested groups showed comparatively clean dentinal surfaces of artificially created internal resorptive defects, the mean scores of SAF (2.50; SD=0.527) and XP Endo Finisher group (2.70; SD=0.483) depicted comparatively cleaner canal walls [Table/Fig-5]. However, the scores in SAF and XP group did not differ statistically (p>0.001) simultaneously both the groups showed statistically significant difference with CSNI group (p<0.001) [Table/Fig-6]. Minimal amount of smear layer and debris was seen in the SEM images of tested samples from SAF and XP group as compared to CSNI group. Also, the SEM images of the SAF group showed much smoother surfaces as compared to the other two groups [Table/Fig-7].
Mean debris score of the respective groups and oneway anova analysis.
| Group | N | Mean | (±) Std. Deviation | Std. Error | 95% Confidence Interval for Mean | Minimum | Maximum | ANOVA p-value |
|---|
| Lower Bound | Upper Bound |
|---|
| CSNI | 10 | 3.70 | 0.483 | 0.153 | 3.35 | 4.05 | 3 | 4 | <0.001 |
| SAF | 10 | 2.50 | 0.527 | 0.167 | 2.12 | 2.88 | 2 | 3 |
| XP ENDO FINISHER | 10 | 2.70 | 0.483 | 0.153 | 2.35 | 3.05 | 2 | 3 |
| Total | 30 | 2.97 | 0.718 | 0.131 | 2.70 | 3.23 | 2 | 4 |
CSNI-Conventional Syringe Needle Irrigation, SAF-Self-Adjusting File
Intergroup comparision via Post-Hoc Test.
| (I) Group | (J) Group | Mean Difference (I-J) | Std. Error | p-value | 95% Confidence Interval |
|---|
| Lower Bound | Upper Bound |
|---|
| CSNI | SAF | 1.20 | 0.22 | <0.001 | 0.65 | 1.75 |
| CSNI | XP ENDO FINISHER | 1.00 | 0.22 | <0.001 | 0.45 | 1.55 |
| SAF | | | | | | |
| XP ENDO FINISHER | -0.20 | 0.22 | 0.646 | -0.75 | 0.35 | |
CSNI-Conventional Syringe Needle Irrigation, SAF-Self-Adjusting File
SEM images of specimen of Internal resorptive defect in the middle third of the canal wall. a) CSNI; b) SAF; c) XP, d) CSNI, arrow depicting accumulation of debris, e) SAF arrow depicting smooth and cleaner canal walls, f) XP arrow depicting cleaner canal walls with irregularities (Fig a to c-SEM images taken at 500X and Fig d to f-SEM images taken at 1000X).
Discussion
In the current study the chemo-mechanical abilities of three different root canal instruments, the SAF, XP and CSNI were evaluated in terms of cleaning efficacy in the IRR defects. Both the SAF and the XP rendered clean dentinal surfaces as compared to CSNI. Syringe irrigation is the routinely used mode for root canal sanitisation; however, in areas of internal root resorptive defects this method is not effective owing to extensive unapproachable irregularities [23,24].
The results of our study showed that there was no significant difference in cleaning efficacy from IRR cavities between SAF and XP group. Successful debridement was achieved by SAF and XP, mostly with scores of one or two signifying that the internal resorptive defects were free of the debris. With respect to SAF the results of the present study are in agreement with the previous studies which also showed satisfactory removal of canal debris in simulated IRR by SAF [5,25]. However, on the contrary another research showed the presence of residual calcium hydroxide despite using SAF in simulated IRR [26].
Since, SAF adapts to the narrowest diameter first, it is fairly difficult for the lattice to fully contact the irregular dentinal walls of the IRR. Despite this fact, the grinding motion and the vibrating effect of the SAF significantly removed dentin from the canal walls [8]. Also, the better scores in the SAF group may be principally related to the continuous activated irrigation with larger volumes. As the SAF was operated for four minutes with a flow rate of 4 mL/minute, a total of 16 mL of NaOCl solution was used. The continuous replenishment of the fresh root canal irrigant during SAF instrumentation ensured sufficient free chlorine in the root canal that completely dissolved the organic component of dentin debris. As suggested by Gu LS et al., the vibrating motion of the system also positively affects the debridement [27]. Additionally, De-Deus G et al., recently suggested that the operation of the SAF system at 5,000 vibrations/minute induces sonic activation of the chosen irrigant throughout the procedure which could result in effective debridement through all regions of IRR defect [5,28].
The positive outcome of the XP group in our study is in agreement with previous researches which also claimed the effectiveness of XP in removing the smear layer and debris from the canal walls; however, those were not carried in artificial IRR [5,25]. Few other contrasting studies showed the presence of residual calcium hydroxide in either simulated IRR or artificial grooves within the canals despite using XP endofinisher. Despite this fact they still suggested the supplementary use of XP owing to its cleansing benefit [12,29]. Other researches, although, not carried out in artificial IRR also claimed the effectiveness of XP in removing the smear layer and debris from the canal walls [21,30]. The positive effect of XP is primarily related to its small diameter (ISO 25) and the ability to change its shape from straight to a specific arc design while rotating in the canal allows it to reach inaccessible areas of the canal wall thus, efficiently removing dentin debris and smear layer.
In our study, we noted that the SEM images of the XP group showed comparatively rougher dentinal surfaces as compared to SAF. This possibly may be explained by the fact that the non-cutting tip of the XP endo finisher only touches the canal wall removing only soft debris and smear layer without altering intact dentin. Additionally, the lack of continuous irrigation alike SAF also could have resulted in the comparatively inferior results in XP group than SAF.
Andreasen FM et al., indicated the use of burs with different diameters to produce small to intermediate IRR, with different diameters and depth [31]. These protocols generate uniform, well characterised cavities, whereas the natural root resorption defects are rather much irregular. This dissimilarity has also been noticed in previous study by Topçuoglu HS et al., [26]. Therefore, in the present study IRR lesions were produced through acid demineralisation process. Lesions were simulated on both the halves of middle third of the root of the same tooth because it has been reported that there is a high frequency of IRR in this specific area. One of the drawbacks of this method is that the lesions are influenced by the internal diameter of the conduit, which was standardised at 2 mm. However, 5% nitric acid could flow freely beyond the conduit, inducing resorption of varied sizes and facilitating acid infiltration and the consequent action on dentin [19]. Also, in this method it was difficult for the operator to control the depth of the defect unlike those resorptive defects produced by bur. Despite this fact, the resultant artificial defects were more over of similar depth which could be attributed to the uniform demineralisation protocol in the entire specimens.
Normal saline was used for storage of extracted teeth until use to prevent dehydration which might adversely affect the properties of tooth structure and result in biased outcome [32].
All the specimen were sealed apically by adapting sticky wax at the apex to prevent irrigating solutions from escaping through canal to simulate the clinical situation. All the specimens were mounted in elastomeric impression material to reapproximate, stabilise and provide additional sealing along with sticky wax.
Scanning electron microscope was opted in this study as it is one of the most recommended and commonly available apparatus for evaluation of smear layer at higher magnification [23]. Tooth specimens were dried thoroughly before the SEM evaluation because SEM involves creation of vacuum. The presence of moisture may interfere with the process resulting in the formation of artifacts.
The research incorporated only single rooted teeth having only one canal to avoid bias and homogenise the treatment procedure. Inclusion of multi-rooted teeth, the presence of curvature in the roots and other anatomic complexities makes the standardisation difficult and also increase the possibility of increased frequency of procedural errors [33].
All the specimens were decoronated below cementoenamel junction to obtain uniform root length of 12 mm. For the rotary instrumentation we used K3 XFTM rotary system as various researches have confirmed that it results in the greater production of debris as compared to any other rotary systems [34].
Limitation
Although, the demineralisation protocol resulted in life like resorptive defects, attaining the standardised depth of defects remains a challenge. Also, the SEM at even higher magnification may provide more specific results. Also, the SEM images in our study were assessed by single examiner only; hence, it may be associated with observer related bias. Therefore, further researches are needed in the similar direction with more specific and refined testing methodologies.
Conclusion
Within the limitations of this study, it can be concluded that SAF and XP endofinisher have superior cleaning ability as compared to CSNI from simulated internal resorption cavities. Hence, the use of these instruments should be incorporated during the treatment of IRR to accomplish long term predictable outcome.
CSNI-Conventional Syringe Needle Irrigation, SAF-Self-Adjusting File
CSNI-Conventional Syringe Needle Irrigation, SAF-Self-Adjusting File