Cerebellar Cognitive Affective Syndrome-A Case Report
MS Bhatia1, Nimisha Doval2, Rashmita Saha3, Aparna Goyal4
1 Director Professor and Head, Department of Psychiatry, University College of Medical Science and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
2 Senior Resident, Department of Psychiatry, University College of Medical Science and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
3 Senior Resident, Department of Psychiatry, University College of Medical Science and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
4 Senior Resident, Department of Psychiatry, University College of Medical Science and Guru Teg Bahadur Hospital, Dilshad Garden, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. MS Bhatia, D-1, Naraina Vihar, New Delhi-110028, India.
E-mail: manbhatia1@rediffmail.com
There are an increasing number of reports suggesting that cerebellum, apart from its significance in movement coordination, plays an important role in cognitive and emotional regulation. Cerebellar Cognitive Affective Syndrome (CCAS) also known as Schmahmann syndrome, refers to deficits in the cognitive domains of executive function, spatial cognition, language and affect resulting from damage to the cerebellum. There are only few case reports reflecting the affective features in CCAS. We present a 17-year-old girl brought to psychiatry Outpatient Department (OPD) with depressive features, who was subsequently diagnosed as a case of CCAS and started on fluoxetine 20 mg and propranolol 20 mg daily. There was improvement in the affective symptoms on follow up.
Cerebellum, Cognition, Degeneration, Depression
Case Report
A 17-year-old female, studying in 12th standard, presented to the psychiatry OPD with a history of persistent low mood, anxiety, decreased interest in pleasurable activities and disturbed sleep for the past two months. This was preceded by gradual onset of weakness in body leading to inability to walk steadily and had frequent falls. She had difficulty in writing and holding things steadily in her hands, all amounting to problems in her scholastic performance. There were no problems in speech. Family history of psychiatric disorder, history of chronic medical illness and substance abuse was absent.
A general physical examination revealed a conscious, cooperative well oriented young girl with normal vitals. On neurological examination, there were ataxic gait, tremors, impaired tandem walking and impaired tests for coordination (finger to nose test, heel-shin test, dysdiadochokinesia). Sensory and motor systems and cranial nerves examinations were normal. Mental state examination revealed poor eye contact, reduced psychomotor activity and speech, depressed affect, decreased self-confidence and hopelessness. Higher cognitive functions including digit span, serial subtraction, FAS test, proverb interpretation were impaired.
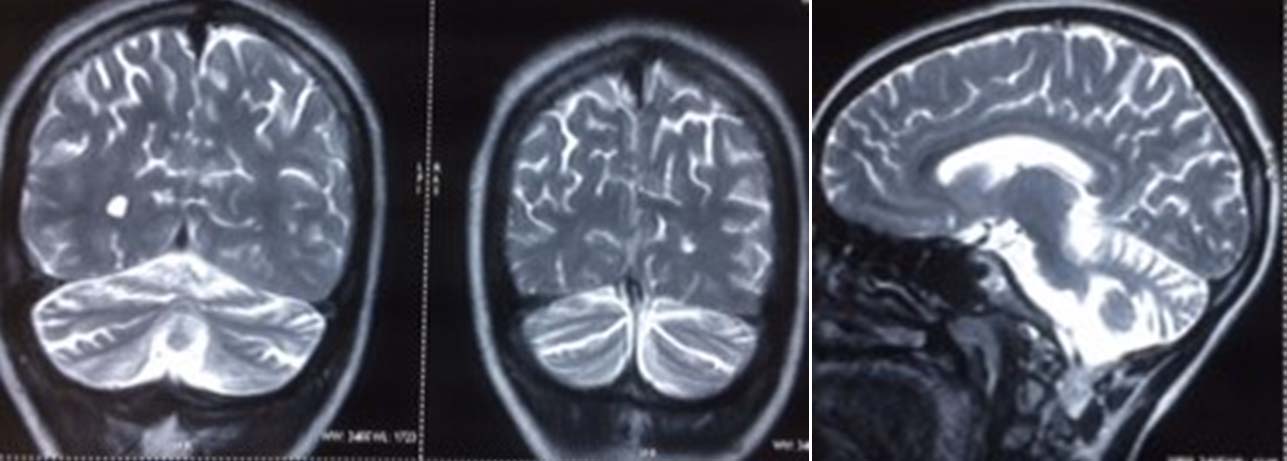
Results of routine blood investigations, liver and kidney function tests, iron and lipid profile, thyroid function tests, vitamin D and B12 levels, X-ray chest, ultrasound abdomen and electroencephalograph were within normal limits. MRI brain showed diffuse cerebellar atrophy with bilateral prominent cerebellar folia [Table/Fig-1-3]. Cerebellar cognitive affective syndrome was diagnosed based on impairment in executive functions, neuropsychiatric manifestations, impaired cerebellar functions and MRI changes [1,2]. Patient was given fluoxetine 20 mg and propranolol 20 mg daily. She reported improvement in anxiety, sleep, appetite and sad mood on fourth week follow-up. On follow-up after eight weeks, her affective symptoms remitted completely. Same medication was continued and regular follow up was advised.
MRI brain showing prominent folia on both sides indicating diffuse cerebellar atrophy.
Discussion
Cerebellar cognitive affective syndrome also known as Schmahmann syndrome was first reported by Schmahmann JD and Sherman JC [1]. It refers to deficits in the cognitive domains of executive function, spatial cognition, language, and affect resulting from damage to the cerebellum. These cognitive impairments result in an overall lowering of intellectual function [2-4]. Although, certain features were prominent in each patient; however, all symptoms were not present in every patient. The behavioural changes were clinically prominent in patients with disease of the posterior lobe of the cerebellum and the vermis [5]. The cerebellum itself has largely been considered for regulation of motor functions. CCAS raises the possibility of cerebellar association with non-motor deficits due to dysfunction in its connections to the cortex and limbic system. Personality changes such as disinhibited and inappropriate behaviour has been reported in CCAS but in our patient it was absent. The severity of CCAS varies depending on the site and extent of the lesion. The behavioural symptoms are severe if the cerebellar lesion is bilateral or it lies in the posterior lobe, especially vermis [1,5]. Behavioural and emotional changes have been linked to dysfunctional circuits between cerebellum, cortex and limbic system [6].
There can be a number of causes for cerebellar damage such as cerebellar agenesis, dysplasia and hypoplasia, cerebellar stroke, tumour, cerebellitis, trauma, neurodegenerative diseases, viral infections and drugs [1,7]. Our patient was more likely to be sporadic as no specific cause could be detected.
Treatment of CCAS include cognitive behaviour therapy, reality orientation therapy, transcranial magnetic stimulation and medications such as bromocriptine (to treat deficit in executive functioning and learning), methylphenidate (to treat deficit in attention and inhibition)but both of these drugs have not been used in CCAS [8-10]. The previous case of CCAS reported by us suggested that Selective Serotonin Reuptake Inhibitor (SSRIs) may be useful in treating mood disturbances [11]. Clomipramine, a tricyclic antidepressant, had also been reported to be effective [12]. Our case responded to SSRI (fluoxetine).
Conclusion
The present case of CCAS presented with depressive features which responded to fluoxetine. So, it is important to screen the patients with CCAS for mood disturbances so that they can be timely treated.
There is need of future studies to find out the treatment modalities and long-term effects of CCAS.
[1]. Schmahmann JD, Sherman JC, The cerebellar cognitive affective syndromeBrain 1998 121(Pt 4):561-79.10.1093/brain/121.4.5619577385 [Google Scholar] [CrossRef] [PubMed]
[2]. Schmahmann JD, Therapeutic and research implicationsInt Rev Neurobiol 1997 41:637-47.10.1016/S0074-7742(08)60374-8 [Google Scholar] [CrossRef]
[3]. Schmahmann JD, The cerebellar cognitive affective syndrome: Clinical correlations of the dysmetria of thought hypothesisInternational Review of Psychiatry 2001 13(4):313-22.10.1080/09540260120082164 [Google Scholar] [CrossRef]
[4]. Wolf U, Rapoport MJ, Schweizer TA, Evaluating the affective component of the cerebellar cognitive affective syndromeJ Neuropsychiatr Clin Neurosci 2009 21(3):245-53.10.1176/jnp.2009.21.3.24519776302 [Google Scholar] [CrossRef] [PubMed]
[5]. Timmann D, Dimitrova A, Hein-Kropp C, Wilhelm H, Dörfler A, Cerebellar agenesis: clinical neuropsychological and MR findingsNeurocase 2003 9(5):402-13.10.1076/neur.9.5.402.1655514972755 [Google Scholar] [CrossRef] [PubMed]
[6]. Konarski JZ, McIntyre RS, Grupp LA, Kennedy SH, Is the cerebellum relevant in the circuitry of neuropsychiatric disorders?J Psychiatr Neurosci 2005 30(3):178-76. [Google Scholar]
[7]. Schmahmann JD, Disorders of the cerebellum: ataxia, dysmetria of thought, and the cerebellar cognitive affective syndromeJ Neuropsychiatry Clin Neurosci 2004 16(3):367-78.10.1176/jnp.16.3.36715377747 [Google Scholar] [CrossRef] [PubMed]
[8]. Ravizza SM, McCormick CA, Schlerf JE, Justus T, Ivry RB, Fiez JA, Cerebellar damage produces selective deficits in verbal working memoryBrain 2006 129(Pt 2):306-20.10.1093/brain/awh68516317024 [Google Scholar] [CrossRef] [PubMed]
[9]. Kim YH, Kim KW, Effects of single-dose methylphenidate on cognitive performance in patients with traumatic brain injury: a double-blind placebo controlled studyClin Rehabil 2006 20(1):24-30.10.1191/0269215506cr927oa16502746 [Google Scholar] [CrossRef] [PubMed]
[10]. Maeshima S, Osawa A, Stroke rehabilitation in a patient with cerebellar cognitive affective syndromeBrain Injury 2007 21(8):877-83.10.1080/0269905070150427317676445 [Google Scholar] [CrossRef] [PubMed]
[11]. Bhatia MS, Saha R, Gautam P, Cerebellar cognitive affective syndrome: A case reportPrim Care Companion CNS Disord 2016 18(2):1010.4088/PCC.15l0185127486531 [Google Scholar] [CrossRef] [PubMed]
[12]. Pesic D, Peljto A, Lukic B, Milovanovic M, Svetozarevic S, Tosevski DL, Cerebellar cognitive affective syndrome presented as severe borderline personality disorderCase Rep Med 2014 2014:89426310.1155/2014/89426324715924 [Google Scholar] [CrossRef] [PubMed]