Biclonal Gammopathy in Multiple Myeloma with Vertebral Compression Fracture
Amit Ranjan1, Rukmini Mysore Srikantiah2, K Ashok Prabhu3, Urmila N Khadilkar4
1 Postgraduate Student, Department of Biochemistry, Kasturba Medical College, Mangaluru, Karnataka, India.
2 Associate Professor, Department of Biochemistry, Kasturba Medical College, Mangaluru, Karnataka, India.
3 Associate Professor, Department of Biochemistry, Kasturba Medical College, Mangaluru, Karnataka, India.
4 Professor, Department of Pathology, Kasturba Medical College, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rukmini Mysore Srikantiah, Associate Professor, Department of Biochemistry, Centre for Basic Sciences, Kasturba Medical College, Bejai, Mangaluru-575003, Karnataka, India.
E-mail: rukmini.shetty@manipal.edu
Biclonal gammopathy is characterised by simultaneous appearance of two different monoclonal proteins. A rare case of Biclonal gammopathy [IgA lambda(λ) and IgG kappa (κ)] and D10 vertebral fracture in a 46-year-old male patient with complaints of sudden onset low back ache while lifting a heavy object, which was aggravated for one month presented to the Orthopaedic department of our institute. Magnetic Resonance Imaging (MRI) of dorso-lumbar spine revealed anterior wedge collapse of D10 vertebral body with enhancement causing compressive myelopathy. Bone marrow biopsy of D10 vertebrae was performed and the features were suggestive of plasma cell myeloma. Serum protein electrophoresis indicated biclonal gammopathy and immunofixation electrophoresis showed intense IgAλand faint IgGκ. The patient was started on chemotherapy following a decompression surgery of the D10 vertebra.
Dorso-lumbar spine, Immunofixation electrophoresis, Serum protein electrophoresis
Case Report
A male patient presented to the Orthopaedics department of our institute, India, with complaints of sudden onset low back ache while lifting a heavy object, which was aggravated in the past one month. General physical examination revealed pallor, BP-120/80 mm Hg, Pulse-72/ min. No abnormality was detected in systemic examination. Local examination of spine revealed tenderness and mild positive extensor plantar reflex.
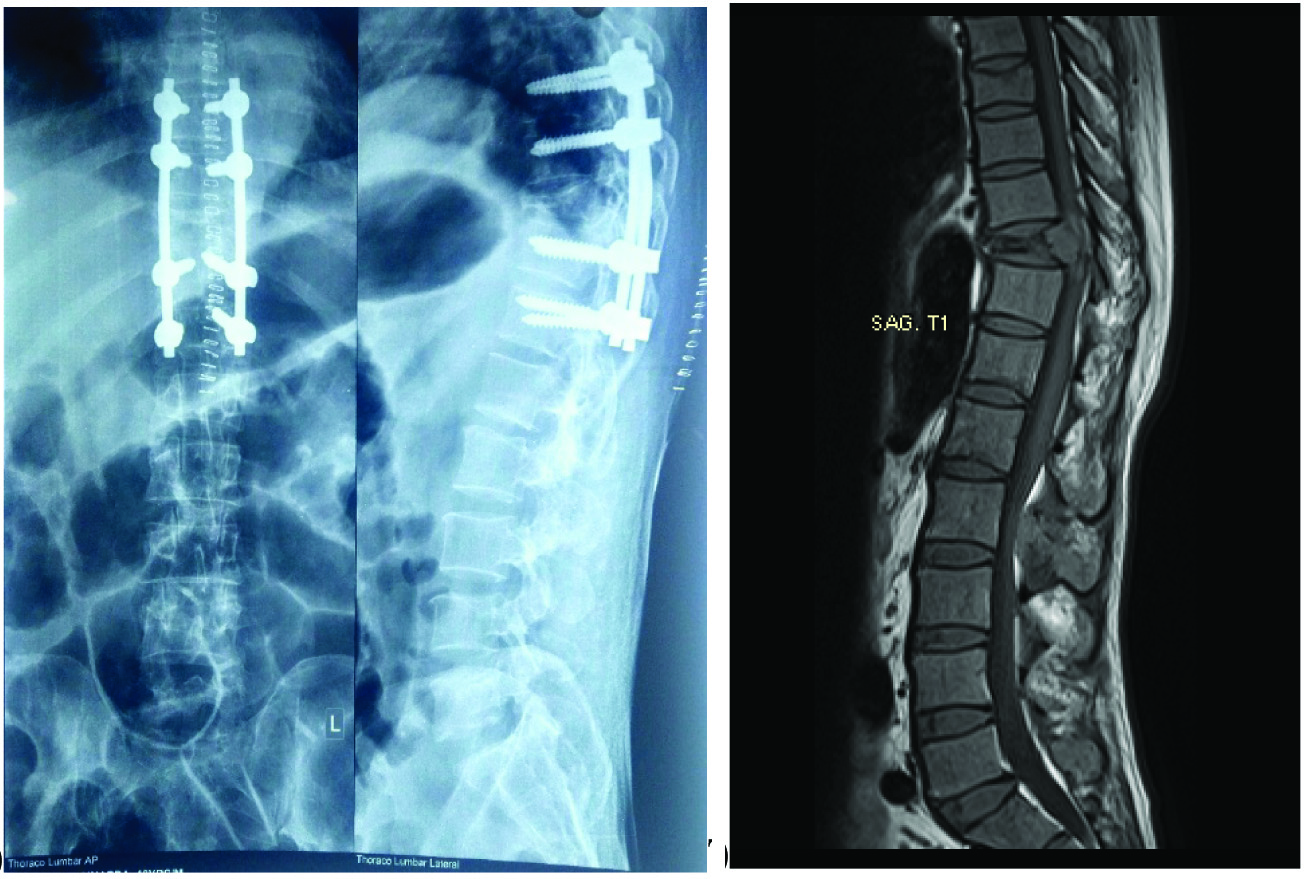
X-ray of the dorso-lumbar spine showed compression fracture of D10 vertebrae with decrease in height of D10 vertebral body [Table/Fig-1a]. MRI of dorso-lumbar spine revealed anterior wedge collapse of D10 vertebral body with enhancing causing compressive myelopathy. The MRI also reported altered signal intensity with diffusion restriction in D10 vertebral body and posterior elements and also in the spinous process of the L2 vertebra with enhanced soft-tissue component and intraspinal extension causing filum terminale indentation [Table/Fig-1b]. The imaging features were in favour of metastasis. The differential diagnosis was lymphoma and histopathological examination was suggested for further correlation.
a) X-ray of dorso-lumbar spine shows compression fracture of the D10 vertebra with decrease in height of vertebral body which was corrected by decompression surgery; b) MRI of the dorsolumbar spine showed anterior wedge collapse of D10 vertebra.
Significant laboratory findings were Haemoglobin-9.9 gm/dL, packed cell volume (PCV) 29.7%, Red Blood Cell (RBC) count 3.20 million/cumm. Peripheral smear showed normocytic normochromic anaemia with rouleaux formation. Total protein was 10.8 gm/dL, albumin and globulin were 2.6 gm/dL and 8.2 gm/dL respectively. Urine analysis was not done because the serum total protein and globulin were high on admission and immediately serum protein electrophoresis done was suggestive of multiple myeloma.
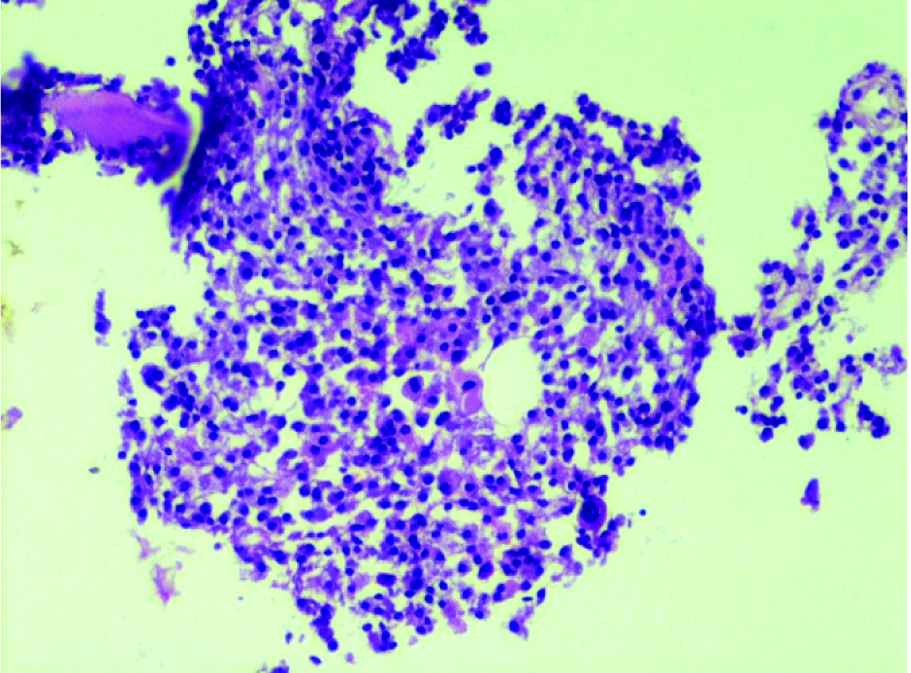
Bone marrow biopsy revealed features suggestive of plasma cell myeloma, with diffuse infiltrate of mononuclear and binuclear cells having eccentric nuclei and basophilic cytoplasm [Table/Fig-2]. Sections from bone marrow showed broad bony trabeculae and nodular interstitial as well as diffuse infiltrate of monotonous mononuclear cells having eccentric nuclei and pink cytoplasm. Haematopoiesis appeared to be relatively preserved in the inter trabecular marrow space.
D10 vertebral body biopsy showing replacement of haematopoietic marrow by eccentric uninucleate and binucleate plasma cells with perinuclear halo.
Discussion
The incidence of biclonal gammopathy is around 1% [1]. The combinations often seen are IgA and IgG (33%), followed by IgM and IgG (24%) among the gammopathies described so far [2]. Approximately 90 % of patients with multiple myeloma develop osteolytic bone lesions often complicated by Skeletal-Related Events (SRE) such as severe bone pain, hypercalcaemia, pathological fractures, vertebral collapse, and spinal cord compression [3]. Multiple myeloma can be the cause of compression fractures along with osteoporosis. About 40% of the patients with biclonal gammopathy present with suggestive clinical signs and symptoms, including significant percentage of the symptomatic patients having underlying lymphoproliferative disease most commonly Waldenstrom Macroglobulinemia (WM) [4]. Nafia Al-Riyami N et al., had presented a rare case of biclonal gammopathy associated with Chronic Lymphocytic Leukemia (CLL) [5]. Nae Yu Kim et al., presented a rare case of biclonal gammopathy accompanied by prostate cancer [6]. Multiple myeloma is an unusual malignancy seen in nearly 10% of all haematological malignancies [7]. According to Pradhan D et al., the most common biclonal pair is IgG and IgA in more than 50% of biclonal gammopathies [8]. Biclonal gammopathy is rare, which is approximately in 1 % of all gammopathies however, the range between 0.14% to 3.2% [9]. Most often observed combinations are IgA and IgG (33%) and IgM and IgG (24%) [2]. For the clinical assessment, Serum Protein Electrophoresis (SPE), immunofixation electrophoresis (IFE) and histopathological study are of great value.
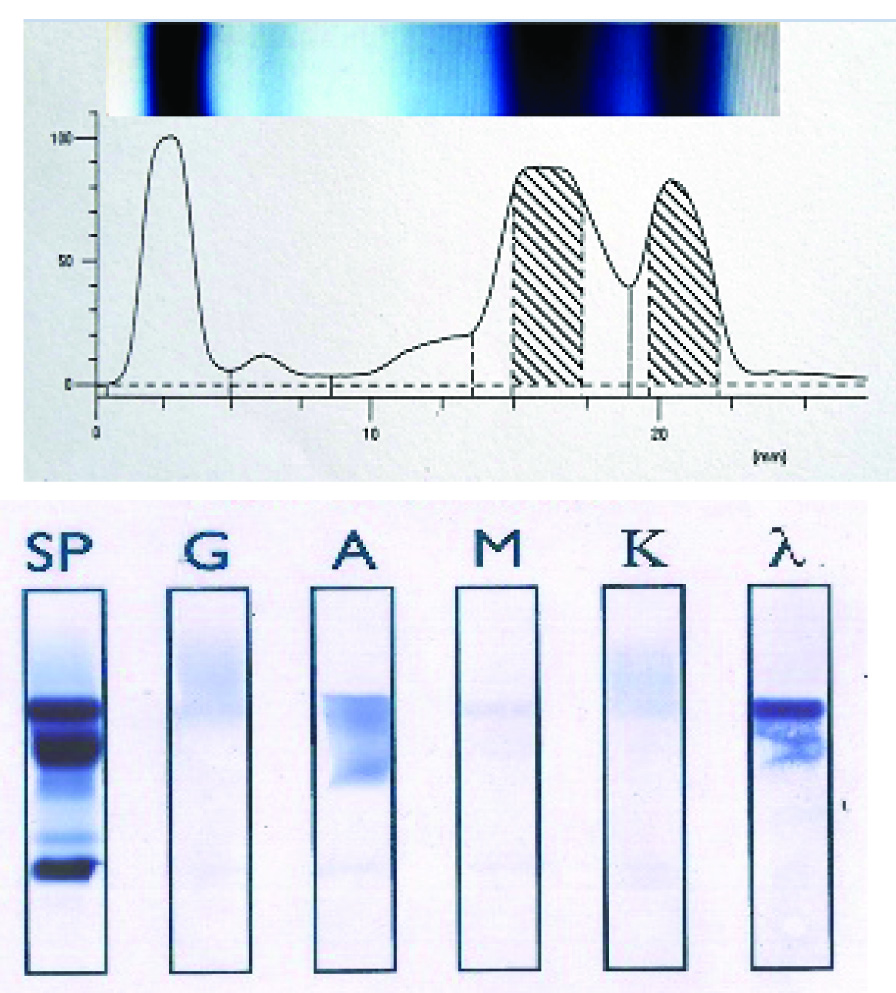
This case showed one spike each in gamma and beta region on SPE [Table/Fig-3a]. M spike is commonly seen in gamma region, but is rare in beta region, IgA λ (γ M spike) and IgG κ (βM spike) on IFE [Table/Fig-3b]. [Table/Fig-4] biclonal gammopathy is considered when, there are two proteins with different mobilities comprising two different monoclonal heavy chains with their respective monoclonal light chains. [Table/Fig-5] shows the criteria for the diagnosis of multiple myeloma.
a) Serum protein electrophoresis. M-spikes in β region and γ region. X-axis is gel pixel value 0-50-100. Y-axis is distance in millimeter starting from albumin band (0 mm) upto gamma band; b) Immunofixation electrophoresis depicting two distinct monoclonal bands of IgA λ (intense) and IgG κ(faint). SP-serum protein, G-IgG, A-igA, M-IgM, K-kappa, λ-lambda.
Serum protein electrophoresis.
| Band | Relative area (%) | Concentration (gm/dL) | Range (gm/dL) |
|---|
| Albumin | 24.21 | 2.59 L | 3.20-5.00 |
| α 1 | 2.99 | 0.32 | 0.10-0.40 |
| α2 | 6.60 | 0.71 | 0.60-1.00 |
| β | 40.54 | 4.34 H | 0.60-1.30 |
| γ | 25.66 | 2.75 H | 0.70-1.50 |
| βM-spike 1 | 23.44 | 2.51 H | |
| γM-spike 1 | 18.79 | 2.01 H | |
Criteria for diagnosis of multiple myeloma [10].
| Criteria for diagnosis of multiple myeloma | Findings in this patient |
|---|
| a) Ten per cent or more clonal plasma cells on bone marrow examination or biopsy-proven plasmacytoma | Bone biopsy of D10 vertebra revealed plasmacytoma |
| b) Occurrence of serum and/or urinary monoclonal protein | SPE and IFE showed biclonal gammopathy |
| c) Any evidence of end-organ damage, hypercalcaemia, renal insufficiency, anaemia, or bone lesions | No evidence of kidney damage.Anaemia (Hb- 9.9 g/dL), D10 vertebra fracture |
In the present case, SPE and immunofixation electrophoresis are suggestive of biclonal gammopathy. The immunohistochemistry with CD 38/138 and CD 20 was indicative for further evaluation, but unfortunately patient was discharged from the hospital and further confirmatory genetic studies could not be undertaken and immunoglobulins were not assayed. Chemotherapy was started prior to discharge from the hospital.
Conclusion
To the best of our knowledge in evidence-based practice in the laboratory context this is a rare presentation of multiple myeloma with para-spinal plasmacytoma, anaemia, biclonal gammopathy having a combination of IgA λ and IgG κ. Further to its rarity, this case may also signify the pathogenesis of plasma cell disorders and its various presentations such as spinal fracture.
[1]. Mahto M, Balakrishnan P, Koner BC, Lali P, Mishra TK, Saxena A, Rarecase of biclonal gammopathyInt J Case Rep Images 2011 2(2):11-14.10.5348/ijcri-2011-02-19-CR-3 [Google Scholar] [CrossRef]
[2]. Wintrobe MM, Clinical Hematology 1981 8th edPhiladelphiaLea and Febiger:1746 [Google Scholar]
[3]. Roodman DG, Pathogenesis of myeloma bone diseaseLeukemia 2009 23(3):435-41.10.1038/leu.2008.33619039321 [Google Scholar] [CrossRef] [PubMed]
[4]. Banerjee A, Pimpalgaonkar K, Christy AL, A Rare Case of Multiple Myeloma with Biclonal GammopathyJ Clin Diag Res 2016 10(12):BD03-BD04.10.7860/JCDR/2016/22466.898428208846 [Google Scholar] [CrossRef] [PubMed]
[5]. Al-Riyami N, Al-Farsi K, Al-Amrani K, Al-Harrasi S, Al-Huneini M, Al-Kindi S, Biclonal gammopathy in chronic lymphocytic leukemia: case report and review of the literatureOman Medical Journal 2015 30(3):216-18.10.5001/omj.2015.4526171130 [Google Scholar] [CrossRef] [PubMed]
[6]. Kim NY, Gong SJ, Kim J, Youn SM, Lee JA, Multiple myeloma with biclonal gammopathy accompanied by prostate cancerKorean J Lab Med 2011 31(4):285-89.10.3343/kjlm.2011.31.4.28522016684 [Google Scholar] [CrossRef] [PubMed]
[7]. Ranjan N, Mohanty B, Multiple myeloma: a case of atypical presentation protein electrophoresisInd J Clin Biochem 2012 27(1):100-02.10.1007/s12291-011-0178-323277721 [Google Scholar] [CrossRef] [PubMed]
[8]. Pradhan D, Arora P, Gami A, Kaur N, Immunoglobulin G kappa biclonal gammopathy associated with multiple myeloma, plasmacytoma and cast nephropathyJ Can Res Ther 2015 11(3):66010.4103/0973-1482.13937926458669 [Google Scholar] [CrossRef] [PubMed]
[9]. Wang E, Kulbacki E, Stoecker M, Concomitant Waldenstrom macroglobulinemia (WM) and IgA plasmablastic myeloma in a patient with untreated IgM paraproteinemia: Sequential development of biclonal B-cell neoplasms over a 10-year period in a single individualHum Pathol 2012 43(7):1135-41.10.1016/j.humpath.2011.11.00122404949 [Google Scholar] [CrossRef] [PubMed]
[10]. Rajkumar SV, Multiple myeloma:2011 update on diagnosis, risk-stratification and managementAm J Hematol 2011 86(1):57-65.10.1002/ajh.2191321181954 [Google Scholar] [CrossRef] [PubMed]