Laser Assisted Management of Telangiectatic Granuloma in Third Trimester of Pregnancy – A Case Report
Aparna Venkatasubramanyam1, Rashmi Hegde2, Shradha Sigtia3, Sangeeta Muglikar4, Varsha Shourie5
1 Postgraduate Student, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India.
2 Reader, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India.
3 Postgraduate Student, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India.
4 Professor and Head, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India.
5 Reader, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Aparna Venkatasubramanyam, Postgraduate Student, Department of Periodontology, M A Rangoonwala College of Dental Sciences and Research Centre, Azam Campus, Pune-411001, Maharashtra, India.
E-mail: draparnavs@yahoo.in
Telangiectatic granuloma is an uncommon overgrowth of the tissues that occurs as a result of various stimuli such as low grade local irritation, traumatic injury or hormonal factors. It generally develops as a solitary, granuloma like, pedunculated, easily bleeding tumour which mostly affects the gingiva followed by buccal mucosa, tongue, lips and palate. Telangiectatic granuloma is also known as granuloma pyogenicum, granuloma gravidarum, pregnancy tumour, vascular epulis, benign vascular tumour and haemangiomatous granuloma. Commonly involved treatment protocols include conventional surgical excision, electrocautery and lasers. The purpose of this article is to report the laser assisted management of an unusual case of telangiectatic granuloma in a 22-year-old female patient in her 32nd week of pregnancy.
Fibroblasts, Gingival Hyperplasia, Histology, Pain
Case Report
A 22-year-old female patient, in her 32nd week of pregnancy reported with a localised overgrowth on the gingiva extending from the distal surface of the mandibular left central incisor to the mesial surface of the mandibular left first premolar, associated with difficulty in speech and mastication along with pain [Table/Fig-1].
Overgrowth extending from mandibular left lateral incisor to mandibular left first premolar. interfering with occlusion, speech and mastication.

On examination, the overgrowth measured approximately 1.2 (width) ×1.5 (length) centimetres in size [Table/Fig-2,3].
Overgrowth measuring 1.5 centimetres in width.

Overgrowth measuring 1.2 centimetres in length.

It was solitary, reddish pink, exophytic, pedunculated, with a warty surface, irregular borders and bled spontaneously on provocation. On palpation, the swelling was tender and firm in consistency.
Following routine blood investigations, a written informed consent was obtained from the patient. Excisional biopsy was performed using a 980 nm diode laser (Zolar Photon Plus) fibre tip with 2.5 W continuous wave in contact mode, under 2% lignocaine infiltration (local anaesthesia) following which a routine scaling and curettage of the area was carried out. The excised tissue was then sent for histopathological examination [Table/Fig-4,5].
Excision of the overgrowth using 980 nm diode laser with fibre tip, continuous wave and in contact mode.

Immediate postoperative view.

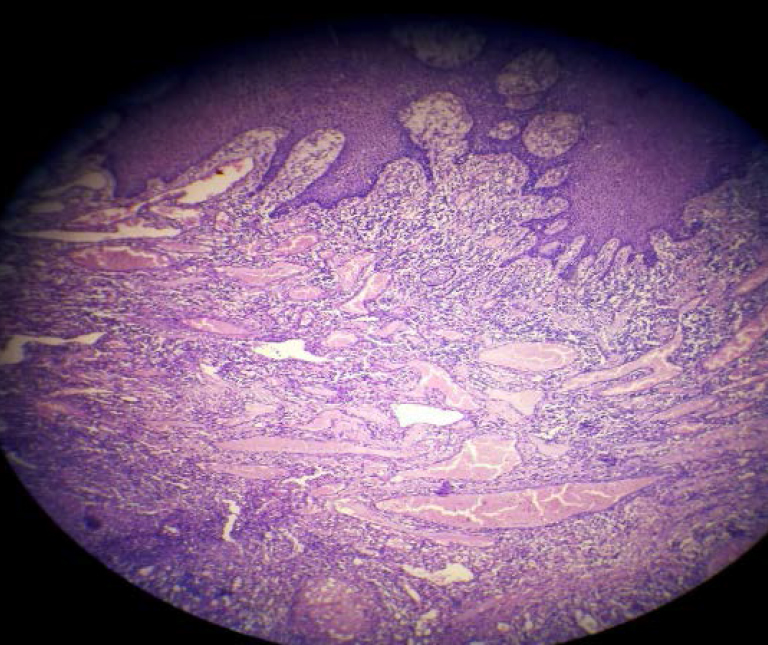
Patient was discharged with all necessary postoperative instructions without any antibiotics and analgesics prescribed to her. Histopathological examination under 4X magnification revealed parakeratinised stratified squamous epithelium which was fibropurulent over an ulcerated surface. The connective tissue showed numerous capillaries, budding endothelial cells and inflammatory cell infiltration giving a clear picture of telangiectatic granuloma [Table/Fig-6].
Histopathology of the overgrowth in H&E stain under 4X magnification suggestive of Telangiectatic granuloma.
Gingivoplasty was carried out one week postoperatively using Carbon Dioxide (CO2) laser 2.5-4 W continuous wave in non-contact defocussed mode, short pulse, hollow wave guide to obtain maintainable gingival contour [Table/Fig-7,8].
One week postoperative image showing slight recurrence of the overgrowth.

Gingivoplasty using carbon dioxide laser 2.5-4 W, continuous wave, non-contact defocussed mode, short pulse, hollow wave guide.

Patient was put on a maintenance protocol till the end of pregnancy after which sequential follow-up for 18 months postoperatively, failed to show any recurrence of the lesion [Table/Fig-9].
18 months postoperative showing no recurrence of the overgrowth.

Discussion
Telangiectatic granuloma is a reactive tumour like lesion that arises in response to various stimuli such as chronic low grade local irritation, traumatic injury, hormonal factors or certain kinds of medication. It is more prominent in the second and the third trimester of pregnancy because of the alteration of the hormones that evokes the activity of proinflammatory cytokines. It even has an effect on the gingival vasculature causing stasis and increased susceptibility to irritation [1]. Local factors and hormonal alteration could cause such a lesion as reported in this case.
Management of patients with such lesions involves conventional surgery along with the control of local factors [2]. Other protocols include the use of flash lamp dye laser, cryosurgery, injection of ethanol, sodium tetradecyl sulphate sclerotherapy, intralesional corticosteroid injection and lasers [3].
Lasers offer advantages of providing a sterile field, haemostasis, good tissue management with less time involved for the procedure and reduced postoperative pain. Reduced postoperative discomfort, oedema, scarring and shrinkage have all been associated with laser excision [4]. Thus, considering the late stage of pregnancy for this patient, minimally invasive laser treatment was opted.
Since pyogenic granuloma is highly vascular, the use of laser is advantageous as laser energy ablation seals the blood vessels, thus, minimising the bleeding potential, leading to excellent haemostasis. Laser not only provides a better incision performance, allowing good modelling of the tissues but also seals the lymphatics and nerve endings. Thus, reducing the postoperative pain and swelling. The healing was uneventful and satisfactory with no clinical evidence of charring or any thermal damage to the lateral tissues [5]. Therefore, considering the stage of pregnancy where any kind of invasive surgical removal of the lesion would be contradicted, treatment with laser was well tolerated by the patient, without any adverse effects.
Treatment considerations during pregnancy are very important as lesions removed during this period may have a higher recurrence rate. Although, it is a non-specific, sharply marked off, non-neoplastic growth in the oral cavity, proper diagnosis, prevention and management of the lesion is very important. Thorough removal of local factors by the clinician, good oral hygiene maintenance during pregnancy and regular follow-up might prevent the occurrence and recurrence of the disease.
Conclusion
The use of lasers offer a new tool that can change the way in which existing treatments are performed, or serve to compliment them.
[1]. Ricardo JH, Alvarez AL, Gomez KR, Oral telangiectatic granuloma. Case series presentationRev Fac Odontol Univ Antioq 2012 23(2):366-75. [Google Scholar]
[2]. Sills ES, Zegarelli DJ, Hoschander MM, Strider WE, Clinical diagnosis and management of hormonally responsive oral pregnancy tumour (pyogenic granuloma)J Reprod Med 1996 41:467-70. [Google Scholar]
[3]. Epivatianos A, Antoniades D, Zaraboukas T, Zairi E, Poulopoulos A, Kiziridou A, Pyogenic granuloma of the oral cavity: comparitive study of its clinicopathological and immunohistochemical featuresPathol Int 2005 55(7):391-97.10.1111/j.1440-1827.2005.01843.x15982213 [Google Scholar] [CrossRef] [PubMed]
[4]. Cobb CM, Lasers in periodontics: a review of the literatureJ Periodontol 2006 77(4):545-64.10.1902/jop.2006.05041716584335 [Google Scholar] [CrossRef] [PubMed]
[5]. Goharkhay K, Moritz A, Wilder-Smith P, Schoop U, Kluger W, Jakolitsch S, Effects on oral soft tissue produced by a diode laser in vitroLasers Surg Med 1999 25(5):401-06.10.1002/(SICI)1096-9101(1999)25:5<401::AID-LSM6>3.0.CO;2-U [Google Scholar] [CrossRef]