Eagle’s syndrome is a symptomatic anomaly due to elongation of styloid process or calcification of stylohyoid ligament manifesting as a pain in cervicofacial region.
The present report is of a 45-year-old female who presented with bilateral cervical pain and vague throat complains, not relieved by medical line of management. She was diagnosed with bilateral elongated styloid process on radioimaging. Intraoral styloidectomy was performed, following which she was completely relieved of her symptoms. This is a rarely performed approached for removal of elongated styloid procedure due to the grave vascular complications, but it has several advantages including minimally invasive, scarless, cost-effective technique with good patient compliance.
Calcification, Cervicofacial pain, Stylohyoidligament
Case Report
A 45-year-old female patient presented to the otorhinolaryngology clinic with complaints of pain on both sides of the neck, dysphagia and foreign body sensation in throat since six months. Pain was insidious in onset, intermittent in nature and sharp shooting in character. Neck pain was aggravated during swallowing. Previous history of surgery or trauma is unremarkable.
On routine physical examination, no other otorhinolaryngological abnormality was found. All third molars were completely erupted and in proper occlusion and temporomandibular joint was normal.
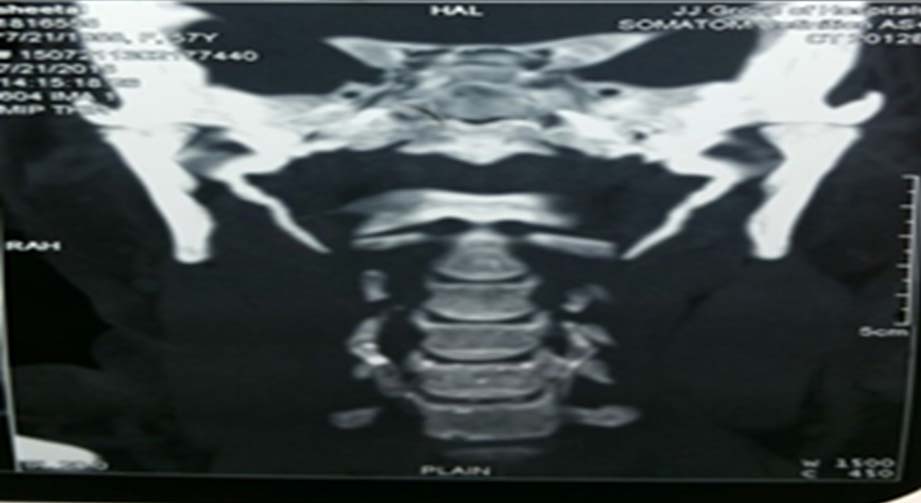
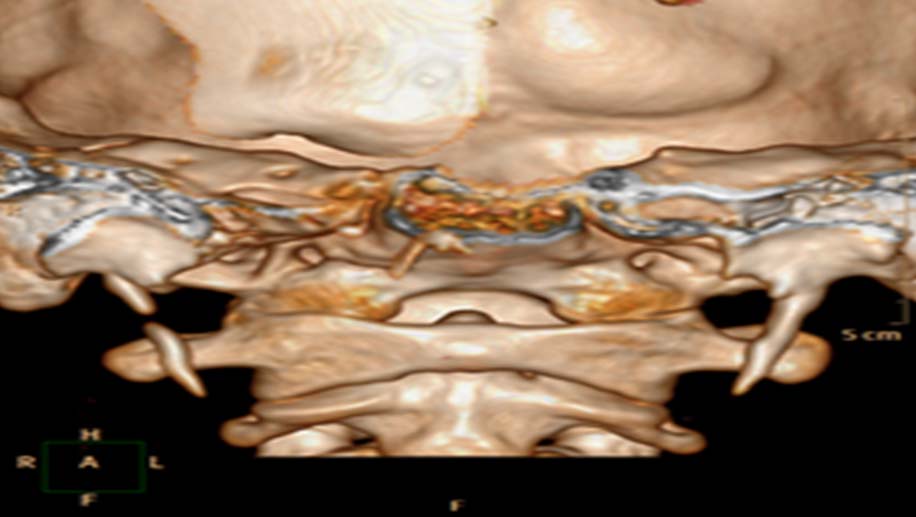
Suspecting an elongated styloid process we palpated the tonsillar fossa at the anterior pillar which elicited a painful response. This was relieved by application of 1% lignocaine in both tonsillar fossa. Orthopantogram and 3D-CT was done which showed bilateral elongated styloid process [Table/Fig-1,2].
Coronal CT showing elongated styloids.
After routine investigations and informed consent for general anaesthesia, patient was posted for surgery. A Boyle-Davis mouth gag was applied to visualise both the tonsils. Bilateral tonsillectomy was done by Dissection and Snare technique. Tonsils were grasped with tonsil holding forceps and drawn medially. Incision was made in the area of mucosa medial to free edge of anterior pillar to depth of surgical capsule. By doing blunt dissection in the loose areolar tissue plane between capsule and superior constrictor muscle inferior pole of tonsil was reached and severed with Eve’s tonsillar snare. After achieving haemostasis, superior constrictor muscles were divided on the tonsillar bed by blunt dissection. Use of epinephrine soaked peanut and bipolar cautery minimized the oozing during dissection. Once the styloid apparatus was exposed, incision was given along the periosteum to deglove it. Styloid process was freed from all its attachments using blunt Cottle’s elevator and angled hypophysis ring curette [Table/Fig-3]. Use of hypophysis ring curette and cottle elevator facilitated preparation of styloid process up to the skull base without any complications like bleeding and carotid sinus reflex. Finally, styloid process was resected by large artery forceps along with its periosteum [Table/Fig-4]. Haemostasis was achieved and the fossa was sutured on both sides using vicryl. Postoperative period was uneventful. Patient is asymptomatic on one year follow up.
Intraoperative view of skeletonized elongated Styloid process.

Resected styloid process.

Discussion
Eagle’s syndrome is caused by elongation of styloid process or calcification of stylohyoid ligament. It is frequently seen in 30 to 40-year-old females. Bilateral elongation of styloid process is common but symptoms are typically unilateral [1,2].
The exact cause of elongation is unknown [2]. Symptoms present diversely, according to length and width of styloid process. Angulation of styloid process is responsible for many of the symptoms, anterior angulation is more important than medial angulation [3].
Cases of carotid artery dissection, stroke and sudden death due to this syndrome are also noted in literature [4]. Sudden death is due to mechanical irritation of carotid sinus by an elongated styloid process which may cause heart to stop resulting in cardiac arrest.
Confirmation of diagnosis should be done by imaging. A 3D-CT is the investigation of choice, as it is most advanced technique available for definitively measuring the length of the styloid process, angulation, and anatomical relation [5]. In our case, right styloid process measured approximately 5cm while the left styloid was about 3cm in length.
At present, Eagle’s syndrome can be treated either pharmacologically or surgically. Conservative management includes Nonsteroidal Anti-Inflammatory Drugs (NSAIDS), drugs used to treat neuralgic pain like Gabapentin and Tianeptine. In addition, 1mL of triamcinolone 10 mg combined with 0.3% Mepivacaine 3 mg injected once in the tosillar fossa can also be tried [6]. All of the above treatment provides temporary relief; hence, surgical management involving resection of elongated styloid process by intraoral or extraoral approach is the treatment of choice for Eagle’s syndrome. Severity of symptoms, degree of elongation and location of styloid process are considered as important factor in establishing the most suitable technique [7]. No matter which approach is adopted excision of styloid processs from its complex anatomical location, in a precise and minimally invasive way is a challenging task.
Intraoral styloidectomy: It was first described by Watt W Eagle [7]. It involves conventional tonsillectomy and approach to styloid by dividing the superior constrictor muscle. Working in between the internal and external carotid artery, for resection of styloid process is associated with the risk of uncontrolled bleeding and even death on table, hence this approach is not preferred by many.
Preoperative planning which includes case selection and arrangement of adequate blood is important. In our experience once the tonsillar bed is open only blunt dissection is advisable. Meticulous dissection with adequate haemostasis to visualise the styloid process is required. Complete resection of styloid process along with its periosteum is essential to avoid recurrence. Though the intraoral approach may seem complicated but the results are gratifying.
Based on our experience this approach is minimally invasive, cost-effective, and cosmetic with quicker postoperative recovery and good patient compliance. Use of angled hypophysis ring curette for skeletonization of elongated styloid prevent damage to surrounding neurovascular structure. Poor visualisation of the operative field is the only considerable disadvantage of this approach. Postoperative care for good oral hygiene is necessary [8,9].
Over the time, some modifications has been made in the conventional technique of intraoral styloidectomy either by changing the site of incision or use of advanced surgical tools like endoscope or surgical navigation.
Scheller K et al., described Retromolar, paratonsillar approach for styloidectomy [10]. As the name suggests, incision for this approach starts from retromolar trigone and extends vertically for approximately 3-4 cm along the mucosa of ascending ramus of mandible. Careful digital palpation of elongated styloid process followed by its exposure by blunt dissection is a key step in this approach. The styloid process is stripped free of soft tissue and ligaments by different angled hypophysis curette and resected by Luer Bone Rongeur or neurosurgical bone punch.
Matsumoto F et al., described use of endoscope to tackle the adjacent important neurovascular structure, but spoiling of scope by blood and need for repeated defogging disfavours its use [11].
Application of Surgical Navigation further revolutionized the technique of styloidectomy. It orients the surgeon about the spatial relationship between styloid process and pharyngeal mucosa. Proponents of surgical navigation pressurize the immunological function of tonsil, which can be preserved by planning incision close to styloid process as directed by navigation without tonsillectomy. It is particularly useful in resection of pseudoarticulated and segmented styloid process with minimal tissue dissection, which by conventional approach might not be fully excised without extensive dissection, which will result in deep neck space infections and of course a longer recovery time [12,13].
Another advancement in the transoral styloidectomy is the use of da vinci Robotic system. It provides excellent visualisation of cephalic parapharyngeal space and adjacent neurovascular structure. Besides its superior magnification and illumination, it allows four-handed surgery in this anatomically complex area [14].
Though this sophisticated technique increases precision in styloidectomy, it simultaneously affects medical cost and patients financial burden.
Extraoral approach: It was described by Caldwell and Loeser. It involves making a cervical incision from proximal portion of sternocleidomastoid muscles to hyoid bone and then dissecting the fascial plane and removing styloid process. Though this approach provides good exposure, it is more invasive and results in a visible scar along with risk of greater auricular paresthesia [15].
Conclusion
Though intraoral styloidectomy is criticised due to its detrimental complication, if well planned and executed, results are rewarding. Surgeons need to be familiar with complex anatomy of styloid process, operative technique and handling of possible complications.
[1]. Strauss M, Zohar Y, Laurian N, Elongated styloid process syndrome: intraoral versus external approach for styloid surgeryTheLaryngoscope 1985 95(8):976-79.10.1288/00005537-198508000-00018 [Google Scholar] [CrossRef]
[2]. Moon CS, Lee BS, Kwon YD, Choi BJ, Lee JW, Lee HW, Eagle's syndrome: a case reportJournal of the Korean Association of Oral and Maxillofacial Surgeons 2014 40(1):43-47.10.5125/jkaoms.2014.40.1.4324627843 [Google Scholar] [CrossRef] [PubMed]
[3]. Yavuz H, Caylakli F, Yildirim T, Ozluoglu LN, Angulation of the styloid process in Eagle’s syndromeEuropean Archives of Oto-Rhino-Laryngology 2008 265(11):1393-96.10.1007/s00405-008-0686-918427825 [Google Scholar] [CrossRef] [PubMed]
[4]. Faivre A, Abdelfettah Z, Rodriguez S, Nicoli F, Bilateral internal carotid artery dissection due to elongated styloid processes and shaking dancingJournal of Neurology, Neurosurgery & Psychiatry 2009 80(10):1154-55.10.1136/jnnp.2008.15995419762905 [Google Scholar] [CrossRef] [PubMed]
[5]. Lee S, Hillel A, Three-dimensional computed tomography imaging of Eagle’s syndromeAmerican Journal of Otolaryngology 2004 25(2):10910.1016/j.amjoto.2003.09.01314976656 [Google Scholar] [CrossRef] [PubMed]
[6]. Wong ML, Rossi MD, Groff W, Castro S, Powell J, Physical therapy management of a patient with Eagle syndromePhysiotherapy Theory and Practice 2011 27(4):319-27.10.3109/09593985.2010.49803620690875 [Google Scholar] [CrossRef] [PubMed]
[7]. Eagle WW, Elongated styloid processes: report of two casesArchives of otolaryngology 1937 25(5):584-87.10.1001/archotol.1937.00650010656008 [Google Scholar] [CrossRef]
[8]. Ceylan A, Köybaşioğlu A, Çelenk F, Yilmaz O, Uslu S, Surgical treatment of elongated styloid process: experience of 61 casesSkull Base 2008 (05):289-95.10.1055/s-0028-108605719240828 [Google Scholar] [CrossRef] [PubMed]
[9]. de Souza Carvalho AC, MagroFilho O, Garcia IR, de Holanda ME, de Menezes JM, Intraoral approach for surgical treatment of Eagle syndromeBritish Journal of Oral and Maxillofacial Surgery 2009 (2):153-54.10.1016/j.bjoms.2008.07.19518771827 [Google Scholar] [CrossRef] [PubMed]
[10]. Scheller K, Eckert AW, Scheller C, Transoral, retromolar, para-tonsillar approach to the styloid process in 6 patients with Eagle’s syndromeMedicina Oral, Patologia Oral Y Cirugiabucal 2014 19(1):e6110.4317/medoral.1874924121903 [Google Scholar] [CrossRef] [PubMed]
[11]. Matsumoto F, Kase K, Kasai M, Komatsu H, Okizaki T, Ikeda K, Endoscopy-assisted transoral resection of the styloid process in Eagle's syndrome. Case reportHead & Face Medicine 2012 8(1):2110.1186/1746-160X-8-2122846221 [Google Scholar] [CrossRef] [PubMed]
[12]. Andrews BT, Thurston TE, Tanna N, Broer PN, Levine JP, Kumar A, A multicenter experience with image-guided surgical navigation: broadening clinical indications in complex craniomaxillofacial surgeryJournal of Craniofacial Surgery 2015 26(4):1136-39.10.1097/SCS.000000000000167226080143 [Google Scholar] [CrossRef] [PubMed]
[13]. Dou G, Zhang Y, Zong C, Chen Y, Guo Y, Tian L, Application of surgical navigation in styloidectomy for treating eagle’s syndromeTherapeutics And Clinical Risk Management 2016 12:575-83.10.2147/TCRM.S10303927110119 [Google Scholar] [CrossRef] [PubMed]
[14]. O’Malley Jr BW, Quon H, Leonhardt FD, Chalian AA, Weinstein GS, Transoral robotic surgery for parapharyngeal space tumorsORL 2010 (6):332-36.10.1159/00032059620924206 [Google Scholar] [CrossRef] [PubMed]
[15]. Diamond LH, Cottrell DA, Hunter MJ, Papageorge M, Eagle's syndrome: a report of 4 patients treated using a modified extraoral approachJournal of Oral And Maxillofacial Surgery 2001 59(12):1420-26.10.1053/joms.2001.2827611732028 [Google Scholar] [CrossRef] [PubMed]