Iniencephaly is an extremely rare neural tube defect with incidence range from 0.1 to 10 in 10,000. It is diagnosed by a triad of fixed retroflexion of the head, variable degrees of cervical lordosis and dysraphism, and an occipital bone defect involving the foramen magnum. It is usually reported as an isolated anomaly and it rarely occurs along with anencephaly. We report here such a rare case of Iniencephaly in association with anencephaly and multiple rare congenital malformations such as asplenia, craniospinal rachischisis, occipital cervical spina bifida and congenital diaphragmatic hernia. It was rare type of congenital diaphragmatic hernia in which intestine coils were lying in front of vertebrae. These anomalies are rare in themselves.
Case Report
A 25-year-old primigravida was referred at 20 weeks of gestation for ultrasound examination. On examination, foetal cardiac activity was present with normal placenta with three vessel cords and amniotic fluid volume was reduced. However, there was absence of cranial vault, cerebral hemispheres and diencephalic structures. The facial structures and orbits were present. Findings were consistent with “acrania-anencephaly sequence”. During pregnancy, several tests conducted like HIV, VDRL, routine urine examination, haematological profile, thyroid function tests were found to be within normal limits. As antenatal findings were incompatible with life, the patient was offered for termination of pregnancy. Abortus was sent to pathology department for postmortem examination.
We received a female foetus weighing 175 gm for autopsy. On external examination, face showed batrachian phenotype (it is due to absence of frontal bone and shallow orbit causing protrusion of eyeballs), scalp, calvarium and normal brain were absent and replaced by an angiomatous mass (area cerebrovasculosa). The base of the skull was also malformed. Posteriorly, the skin was lacking all over the ill-developed vertebrae revealing the spinal cord (“craniospinal rachischisis”) and spina bifida at occipital cervical region (iniencephaly with anencephaly) as shown in [Table/Fig-1a-c].
a,b) shows lateral and dorsal view of the anencephalic foetus showing craniospinal rachischisis. c) shows frontal view of the foetus showing batrachian phenotype. d) (anterior posterior view) e) (lateral view): Infantogram of the foetus showed abnormal vertebrae with spina bifida in first vertebrae (arrow). f) In situ examination showing enlarged liver, asplenia with undisplaced heart and lung in chest cavity (arrow). g) After dissecting and removing liver, heart, both lungs and diaphragm. We observed that intestine coils were herniated into the chest cavity and were lying just in front of vertebrae, h) shows intestine protruding from spinal bifida at occipital cervical region (arrow).
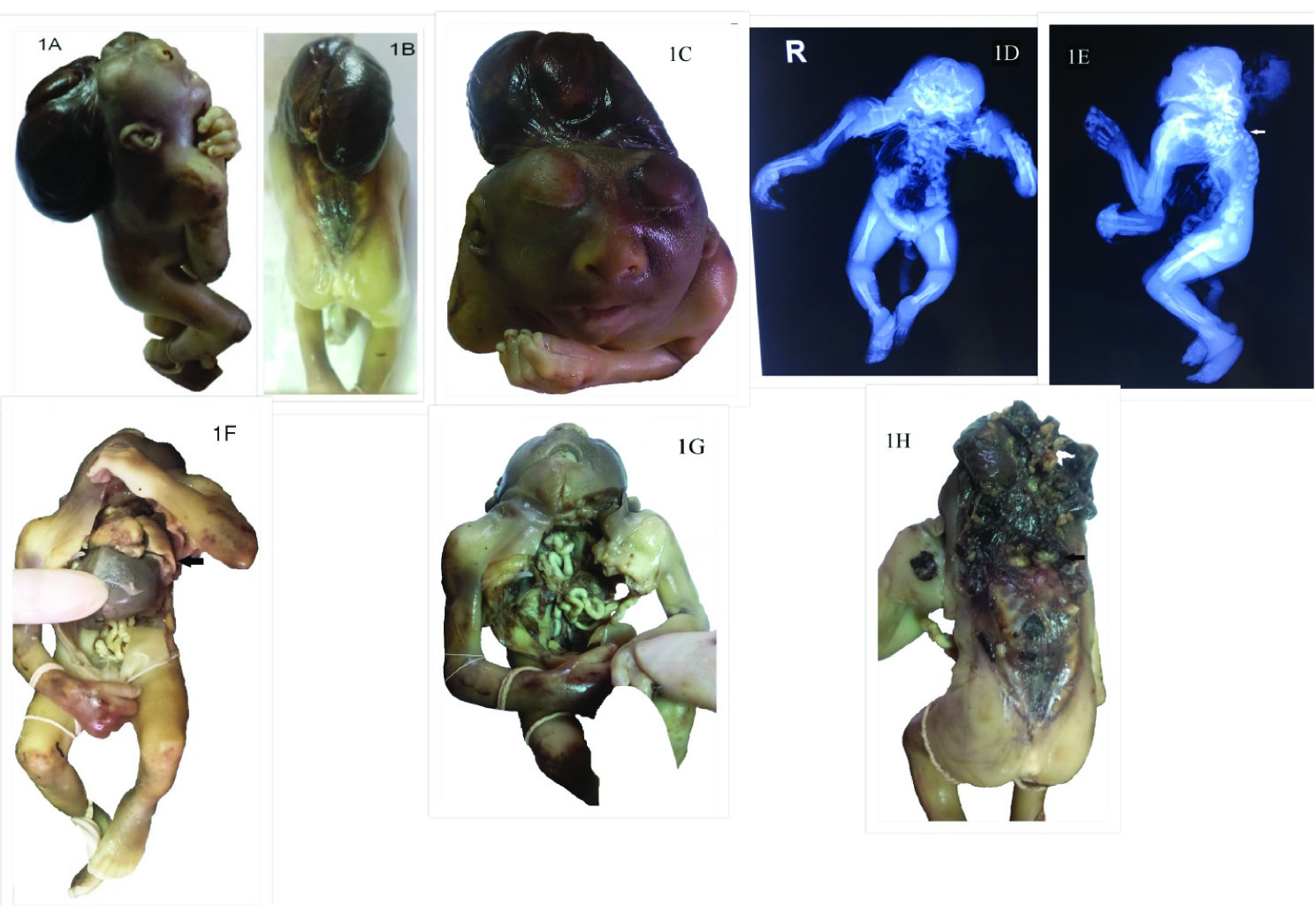
Infantogram of the foetus showed vertebrae were abnormal and absent and spina bifida was seen in first vertebrae [Table/Fig-1d,e].
On dissection, liver was enlarged and it occupied the whole of the abdomen. Spleen was absent; heart and both the lungs were normal and were not displaced in the chest cavity. In abdominal cavity, both the kidneys and both adrenals were normal [Table/Fig-1f].
After dissecting and removing liver, heart, both lungs and diaphragm. We observed that intestine coils were herniated into the chest cavity and were lying just in front of vertebrae and could be seen from spinal defect at occipital cervical region [Table/Fig-1g,h].
Histological examination of the angiomatous mass (area cerebrovasculosa) showed cystically dilated vascular spaces; normal lungs; extramedullary haemopoiesis in the liver and congested kidneys showing nephrogenic zone.
Hence, a diagnosis of congenital asplenia with craniospinal rachischisis in an iniencephaly with anencephaly foetus with spina bifida at occipital cervical region and rare posterior paravertebral congenital diaphragmatic hernia was offered. Genetic studies were not undertaken on the foetal samples.
Discussion
Iniencephaly is derived from the Greek word “Inion” which means nape of the neck and was first described by scientist Étienne Geoffroy Saint-Hilaire [1,2]. Iniencephaly implies to deficiency of occiput in the region of foramen magnum, spina bifida with rachischisis of cervical and thoracic spine and retroflexion (extreme extension) of the spine, which are also three major diagnostic criteria [3]. It is a rare and fatal neural tube defect with incidence of ~0.1-10:10,000 [4]. The incidence of iniencephaly reported by Jayant K et al., was between one in 900 to one in 2200 deliveries in the world; whereas in India it has been reported to be 1:60,000 deliveries or ~0.1-10:10,000 birth [3-5]. Jayant K et al., and Morocz I et al., both reported female preponderance (1:9) in iniencephaly [4,5-7], whereas anencephaly is most common neural tube defect with incidence of ~1:1000 with female predominance (4:1) [4].
Etiology of both iniencephaly as well anencephaly is polygenic and multifactorial wherein genetic (trisomy 18, trisomy 13, monosomy X), environmental factor (poor socioeconomic, low parity, lack of folic acid supplements, obesity), drugs (sulphonamide, tetracycline, antihistamines, antitumor agents, clomiphene citrate, sedatives), nutrients (deficiency of iron and folic acid) and maternal factors (congenital syphilis, maternal use of teratogenic chemicals (streptonigrin, triparanol and vinablastine), cigarette smoking, alcohol use and substance abuse); individually or in combination play an important role [1,2,4,8].
Lewis in 1897 classified iniencephaly on the basis of presence or absence of encephalocele as iniencephaly apertus’ (iniencephaly with encephalocele) and ‘iniencephaly clausus’ (iniencephaly without encephalocele). Howkins and Lawrie in 1939 classified iniencephaly into simple iniencephaly and anencephaly with spinal retroflexion [4].
Present diagnostic criteria for iniencephaly was given by Cimmino CV et al., and Bose S et al., which is [4,9,10]:
Occipital bones deficit resulting in an enlarged foramen magnum. The defect of the occiput can vary from a minimal defect to an acrania;
Cervical and thoracic vertebrae are partially or totally absent as well as they can be irregularly fused, along with incomplete closure of the vertebral arches and/or bodies (rachischisis) (Vertebral malformation results in retroflexion and crowding of ribs which causes lack of space hence, increased pressure in thoracic and abdominal cavity causing various hypoplasia or malformation);
Accentuated retroflexion of the head, a significant shortening of the foetal spine is also present as a result of extreme lordosis and hyperextension (or retroflexion) of a malformed neck spinal column due to absence of neural arches. Eberhard Merz et al., suggested that because of absent cervical vertebra and large foramen magnum, head assumes an extreme dorsiflexion [11,12] classified retroflexion of the cervical spine on the basis of severity [Table/Fig-2] [13];
Face is turned upward and due to the lack of neck, mandibular skin is directly continuous with that of the chest [4].
Degree of retroflexion [8].
| Features | Severe Retroflexion | Moderate Retroflexion | Mild Retroflexion |
|---|
| Neck | Absent | Short | Short |
| Face looks | Upward | Upward and forward at an angle of about 450 with the horizontal plane | Forward |
| Mentothoracic junction | Convex | Flat | Shallow groove |
| Hairline | Hairline extends on the back to the lumbar region | Hairline extends on the back to the midthoracic level | Hairline extends on the back to the lower cervical region |
| Cervical and upper thoracic vertebrae | Are drastically reduced in number | Normal | Normal |
| Anterior spina bifida | Frequent | Present | Absent |
| Diaphragmatic defect | Present | Present | Absent |
Our case showed all the above features.
Iniencephaly is usually associated with other congenital malformations of various systems [Table/Fig-3] [1,12,14]. Only few cases of iniencephaly with anencephaly have been reported till now [Table/Fig-4] [1,7,15-22]. Our case had iniencephaly with anencephaly, congenital diaphragmatic hernia, occipito cervico spinal bifida and asplenia. Asplenia was first time reported in our case.
Systemic anomalies associated with Iniencephaly [1,6].
| System | Anomaly |
|---|
| Central Nervous System (CNS) | AnencephalyVentriculomegalyEncephaloceleMicrocephalyHoloprosencephalyPosterior fossa defectsDandy walker malformation |
| Spine | Spina bifidaRachischisis |
| Head and neck | Thymic hyperplasia |
| Respiratory | Pulmonary hypoplasia |
| Cardiovascular | Single umbilical arteryCardiac defects |
| GIT | OmphaloceleDiaphragmatic hernia (posterior diaphragmatic defect is most obvious) |
| Renal | Inguinal hernia Adrenal hypoplasiaHydronephrosisPolycystic kidney |
| Skeletal | Club foot |
Reported cases of iniencephaly with anencephaly.
| Authors | Reference number | No: of cases reported | Gestational age at diagnosis (weeks) | Gender | Cytogenetic analysis | CNS anomalies | Other anomalies |
|---|
| Our Study | - | 01 | 20 | Female | NA | iniencephaly with anencephaly | craniospinal rachischisis, spina bifida at occipital cervical region, asplenia, posterior paravertebral congenital diaphragmatic hernia |
| Gupta A et al., | [1] | 01 | 18 | Female | NA | iniencephaly with anencephaly, | craniospinal rachischisis |
| Mórocz I et al., | [7] | 02 | 33 | Female | NA | iniencephaly with anencephaly | omphalocele |
| | | 36 | Female | NA | iniencephaly with anencephaly | spina bifida, ventricular septal defects, pulmonary hypoplasia |
| Meizner I and Bar-Ziv | [15] | 01 | 26 | Female | NA | iniencephaly with anencephaly | craniospinal rachischisis, omphalocele, bilateral club feet, bilateral cleft lip and palate |
| Sherer DM et al., | [16] | 01 | 26 | Female | 46, XX | iniencephaly with anencephaly | craniospinal rachischisis |
| Dogan MM et al., | [17] | 12 | 31 | Female | NA | iniencephaly with anencephaly | spina bifida, congenital diaphragmatic hernia, duodenal atresia, bilateral club feet |
| | | 30 | Female | NA | iniencephaly with anencephaly | spina bifida, craniospinal rachischisis, congenital diaphragmatic hernia, single umbilical artery |
| | | 20 | Male | NA | iniencephaly with anencephaly | craniospinal rachischisis, single umbilical artery |
| | | 21 | Male | NA | iniencephaly with anencephaly | spina bifida, craniospinal rachischisis, omphalocele, bilateral cleft lip, |
| | | 31 | Female | NA | iniencephaly with anencephaly | cervicothoracic spina bifida, posterior encephalocele, duodenal atresia, bilateral club feet |
| | | 32 | Female | NA | iniencephaly with anencephaly | craniospinal rachischisis, congenital diaphragmatic hernia, Single umbilical artery, hypoplastic lungs, |
| | | 26 | Female | NA | iniencephaly with anencephaly | cervicothoracic spina bifida, unilateral cleft lip, left club foot |
| | | 26 | Male | NA | iniencephaly with anencephaly | craniospinal rachischisis, omphalocele |
| | | 25 | Female | NA | iniencephaly with anencephaly | cervical spina bifida, omphalocele, single umbilical artery, left club foot |
| | | 26 | Female | NA | iniencephaly with anencephaly | spina bifida, cleft lip, duodenal atresia, bilateral club feet |
| | | 25 | Female | NA | iniencephaly with anencephaly | cervical spina bifida, omphalocele, single umbilical artery |
| | | 28 | Female | NA | iniencephaly with anencephaly | spina bifida, single nostril, dysplastic kidneys |
| Balci S et al., | [18] | 01 | 20 | Male | NA | iniencephaly with anencephaly | craniospinal rachischisis, |
| Jeanne-Pasquier C et al., | [19] | 01 | 13 | Female | NA | iniencephaly with anencephaly | omphalocele |
| Rousso D et al., | [20] | 01 | 21 | Male | NA | iniencephaly with anencephaly | cervicothoracic rachischisis, agenesis of left kidney |
| Halder A et al., | [21] | 01 | 21 | Male | Mosaictrisomy 13 | iniencephaly with anencephaly | single umbilical artery, left cleft lip and palate, club foot, dilated right side of the heart |
| Tonni G et al., | [22] | 01 | 12 | Female | Trisomy X | iniencephaly with anencephaly | Flat face, Absent nasal bones, Micromelia of left forearm, Club foot, Spinal defect from occiput to sacrum |
Pathogenesis of isolated iniencephaly is developmental error occurring in early pregnancy at 24 days gestational age i.e., prior to closure of cephalic neural folds [3]. In early stages of embryo development, paravertebral sclerotome (mesoderm) differentiates into a ventral mass which forms the vertebral bodies, pedicles and their cranial homologous and a dorsal mass which forms neural arches and vault bones of the cranium. In iniencephaly, either one or both of ventral mass or dorsal mass are hypoplastic or ill developed [8]. Trenouth MJ reported that brain growth in normal fetuses influe reported that brain growth in normal foetuses influences the development of cranial base and position of the face and the nasomaxillary segment, so in anencephaly, as the influence of the expanding brain is removed, it causes secondary adaptive alterations in the cranial base like ill-developed squamous occipital bones [4,23] . Simple iniencephaly, is characterized by arrest as well as imperfect development of base of skull (portion of neural tube) i.e., occipitocervical region and vertebral column (cervicothoracic region mainly) i.e., caudal end of rhombencephalon [3,6]. When iniencephaly occurs with anencephaly where vault and facial bones as well as lower vertebrae are involved, defects are seen in five sites that are mid cervical, between prosencephalon and mesencephalon, at stomodeum, caudal end of rhombencephalon and most caudal end of neural tube [6].
To differentiate iniencephaly with anencephaly with spinal retroflexion is that in iniencephaly, cranial cavity is present with uninterrupted skin covering the retroflexed region and the head whereas, latter has partial or complete absence of the neurocranium, and the affected region of nervous tissue is not covered with skin [24]. It is related to time of onset as iniencephaly occur few days later than anencephaly [4,13]. The cervical vertebrae are abnormal in iniencephaly whereas it is normal in anencephaly [4]. When there is both an absent calvarium as well as abnormal cervical vertebrae, it is a case of iniencephaly with anencephaly (our case) [4].
Differential diagnosis of iniencephaly includes anencephaly with spinal retroflexion (described above) and Klippel–Feil malformation complex i.e., shortness of the neck with fusion of the cervical vertebrae, patients are compatible with life; incidence is one in 50,000 and 65% of are female [12].
Prognosis is usually fatal and depends on the severity of associated anomalies and the degree of retroflexion [1]. The recurrence risk in further pregnancy is 1-4%. Adequate counselling about recurrence risk, folic acid supplementation and early foetal surveillance are advisable to the parents [4].
Conclusion
Iniencephaly and anencephaly are two different entities and association of both together is extremely rare and only few cases have been reported in the past. Both iniencephaly and anencephaly have fatal prognosis. So, early diagnosis of these conditions allows termination of pregnancy to avoid undue stress to the parents. This case of iniencephaly with anencephaly is being reported for its rare occurrence and also for its association with unusual findings. This case report will enrich information on this entity.
[1]. Gupta A, Patel P, Yadav C, Iniencephaly with Anencephaly: Case ReportSch J App Med Sci 2014 2(5D):1781-84. [Google Scholar]
[2]. Inencephaly. In: Chen CP editor. Prenatal diagnosis and genetic counseling of Neural tube defects: An overview and Atlas of Cases. 1th ed. Taiwan: Elsevier; 2009. Pp.51-64 [Google Scholar]
[3]. Halder A, Pahi J, Pradhan M, Pandey A, Gujral R, Agarwal SS, Iniencephaly: A Report of 19 CasesInd Ped 1998 35:891-96. [Google Scholar]
[4]. Pratibha B, Neural tube defects with gastrointestinal malformations. [Blog]Indian Health Journal 2011 Available from: https://indianhealthjournal.wordpress.com/2011/10/01/neural-tube-defects-with-gastrointestinal-malformations-dr-baldawa-pratibha. [last assessed on 2017, March 16] [Google Scholar]
[5]. Jayant K, Mehta A, Sanghvi LD, A study of congenital malformations in MumbaiJ Obstet & GynaecolIndia 1961 11:280-94. [Google Scholar]
[6]. Kandhare B, Chitnis A, Bansal D, Patel B, Congenital malformations associated with iniencephalyJournal of Evolution of Medical and Dental Sciences 2013 l2(34):6438-43.10.14260/jemds/1157 [Google Scholar] [CrossRef]
[7]. Morocz I, Szeifert GT, Molnar P, Toth Z, Csecsei K, Papp Z, Prenatal diagnosis and pathoanatomy of iniencephalyClin Genet 1986 30:81-6.10.1111/j.1399-0004.1986.tb00574.x3530565 [Google Scholar] [CrossRef] [PubMed]
[8]. Panduranga C, Kangle R, Suranagi VV, Pilli GS, Patil PV, Anencephaly: A pathological study of 41 casesJ Sci Soc 2012 39:81-4.10.4103/0974-5009.101852 [Google Scholar] [CrossRef]
[9]. Cimmino CV, Painter JW, IniencephalyRadiology 1962 79:942-44.10.1148/79.6.94214021377 [Google Scholar] [CrossRef] [PubMed]
[10]. Bose S, Makhani JS, Thaker SV, IniencephalyIndian J Med Sci 1964 18:590-94. [Google Scholar]
[11]. Merz E, Bahlmann F, Ultrasound in Obstetrics and Gynecology 2005 2nd editionGermanyGeorg Thieme Verlag Publishers:212-45. [Google Scholar]
[12]. Guala A, Massa P, Foscolo AM, Olivero F, Van Maldergem L, Danesino C, Association of iniencephaly, anencephaly and fusion of cervical vertebral bodies: a new autosomal recessive syndrome?Clin Dysmorphol 2013 22(1):29-32.10.1097/MCD.0b013e3283590b0423011585 [Google Scholar] [CrossRef] [PubMed]
[13]. Bustami MF, Hadidi MT, Iniencephaly and anencephaly with spinal retroflexion: A comparative study of twelve human specimensJ Med J 2007 41(1):19-27. [Google Scholar]
[14]. Chen CP, Prenatal diagnosis of iniencephalyTaiwan J Obstet Gynecol 2007 46(3):199-207.10.1016/S1028-4559(08)60021-2 [Google Scholar] [CrossRef]
[15]. Meizner I, Bar-Ziv J, Prenatal ultrasonic diagnosis of a rare case of iniencephaly apertusJ Clin Ultrasound 1987 15:200-3.10.1002/jcu.18701503103134417 [Google Scholar] [CrossRef] [PubMed]
[16]. Sherer DM, Hearn-Stebbins B, Harvey W, Metlay LA, Abramowicz JS, Endovaginal sonographic diagnosis of iniencephaly apertus and craniorachischisis at 13 weeks, menstrual ageJ Clin Ultrasound 1993 21:124-7.10.1002/jcu.18702102098381132 [Google Scholar] [CrossRef] [PubMed]
[17]. Dogan MM, Ekici E, Yapar EG, Soysal ME, Soysal SK, Gokmen O, Iniencephaly: sonographic-pathologic correlation of 19 casesJ Perinat Med 1996 24:501-11.10.1515/jpme.1996.24.5.5018950731 [Google Scholar] [CrossRef] [PubMed]
[18]. Balci S, Aypar E, Altinok G, Boduroglu K, Beksac MS, Prenatal diagnosis in three cases of iniencephaly with unusual postmortem findingsPrenat Diagn 2001 21:558-62.10.1002/pd.9711494291 [Google Scholar] [CrossRef] [PubMed]
[19]. Jeanne-Pasquier C, Jacob B, Dreyfus M, Herlicoviez M, Iniencephaly and early prenatal diagnosisJ Gynecol Obstet Biol Reprod 2002 31:387-9. [Google Scholar]
[20]. Rousso D, Psara A, Venizelos I, Tsimas V, Kourtis A, Panidis D, Prenatal ultrasonographic diagnosis of iniencephalyJ Obstet Gynaecol 2003 23:572-3.10.1080/014436103100015662712963531 [Google Scholar] [CrossRef] [PubMed]
[21]. Halder A, Agarwal S, Pandey A, Iniencephaly and chromosome mosaicism: a report of two casesCongenit Anom (Kyoto) 2005 45:102-5.10.1111/j.1741-4520.2005.00076.x16131369 [Google Scholar] [CrossRef] [PubMed]
[22]. Tonni G, Azzoni D, Panteghini M, Ventura A, Cavalli P, First trimester diagnosis of iniencephaly associated with fetal malformations and trisomy 18: report of a new case and gene analysis on folate metabolism in parentsCongenit Anom (Kyoto) 2007 47(3):101-04.10.1111/j.1741-4520.2007.00154.x17688469 [Google Scholar] [CrossRef] [PubMed]
[23]. Trenouth MJ, Craniofacial shape in the anencephalic human fetusJ. Anat 1989 165:215-24. [Google Scholar]
[24]. Lemire RJ, Beckwith JB, Shepard TH, Iniencephaly and anencephaly with spinal retroflexion. A comparative study of eight human specimensTeratology 1972 6(1):27-36.10.1002/tera.14200601055056790 [Google Scholar] [CrossRef] [PubMed]