Cor Triatriatum Dexter in a Male Cadaver
Pooja Bhadoria1, Neelam Vasudeva2
1 Senior Resident, Department of Anatomy, Maulana Azad Medical College, Ghaziabad, Uttar Pradesh, India.
2 Professor and Head, Department of Anatomy, Maulana Azad Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pooja Bhadoria, Senior Resident, Department of Anatomy, Maulana Azad Medical College, New Delhi-110002, India.
E-mail: dr.poojabhadoria@gmail.com
Cor Triatriatum Dexter (CTD), is a very rare congenital anomaly in which right atrium is partitioned to form three chambered heart. It is caused by the persistence of the right valve of the sinus venosus. We herein report a case, where during routine dissection on the heart of male cadaver, a well-developed membrane was seen, separating the smooth and rough parts of right atrium. This can have varying clinical manifestations depending on the degree of partition of the right atrium. Knowledge about presence of such membrane is important for physician’s, as severe partition can lead to obstruction of the tricuspid valve, the right ventricular outflow tract, or the inferior vena cava associated with right-sided heart failure and elevated central venous pressures.
Central venous pressures, Right atrium, Sinus venosus, Tricuspid valve
Case Report
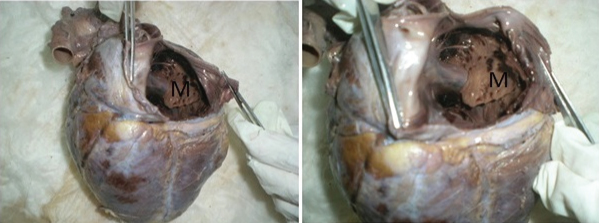
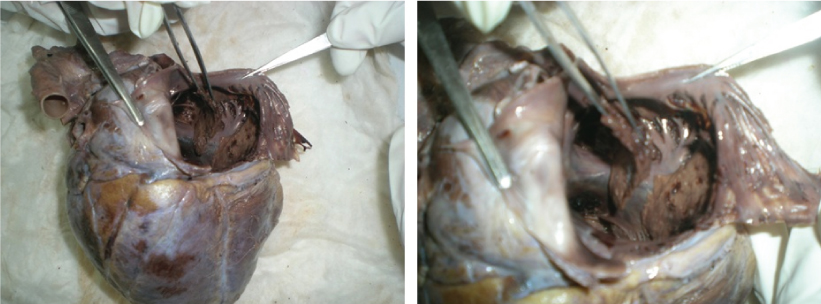
This is a case of 40-year-old male cadaver in the Department of Anatomy at Maulana Azad Medical College, Delhi, India. His medical records mentioned that he died of cardiorespiratory arrest. During routine dissection, as a part of undergraduate teaching of thoracic region, thoracic cage was cut and reflected, after that heart was separated from the great vessels and pericardium. Heart was taken out and using dissecting scissors and an incision was made extending from the opening of superior vena cava to inferior vena cava in right atrium and the walls were carefully retracted. The interior was washed thoroughly with normal saline. A fibromuscular membrane was seen attached to the crista terminalis separating the posterior smooth and anterior rough parts. This membrane displayed many fenestrations with well-defined margins [Table/Fig-1]. Fine dissection revealed that the right edge of this membrane was attached to the crista terminalis and the left edge was free with well-defined curved (inverted C shaped) concave margin [Table/Fig-2]. The size of right atrium, interatrial septum and the opening of coronary sinus guarded by thebasian valve appeared normal. The rough part of right atrium displayed musculi pectinati, which extended into the auricle and the smooth part received the superior vena cava, inferior vena cava and coronary sinus. All other chambers of the heart and the inteventricular septum were normal in appearance. There was no other associated vascular anomaly of major branches of aortic sinus and the arch of aorta appeared to be normal.
The image is showing the fibromuscular fenestrated membrane (M) in the right atrium of heart.
The image is showing the fibromuscular fenestrated membrane (M) in the right atrium of heart. It is separating the smooth part from rough part which can be appeciated after reflecting the cut edges of membrane.
Discussion
The incidence of CTD, an extremely rare malformation is approximately 0.025% of all congenital heart diseases. Cor triatriatum is a congenital heart defect where the left atrium or right atrium is divided by a thin membrane, resulting in three chambered heart i.e Cor triatriatum sinistrum and Cor triatriatum dextrum respectively [1]. The cor triatriatum sinistra is more common form of abnormal atrial septation and is associated with pulmonary venous obstruction. CTD represents the more severe form of abnormal venous valve regression with complete or near complete septation of the right (i.e., dexter) atrium. Septation of the right atrium (CTD), can interfere with normal blood flow into the right atrium and can lead to broad range of clinical symptoms [2].
Jain A et al., in 2013 showed presence of eustachian valve in 27 out of 40 patients. Author reported variety of variations in the valve like being either ridge like or membranous or associated with fine network of strands [3].
The membrane in the right atrium is mostly an incidental finding and in some cases it is found in trans-echocardiography. Zainudin AR et al., in 2012 reported a case of a nine-year-old boy, showing trans-echocardiography; a membrane across right atrium [4]. Juan A et al., reported two cases of CTD in adults, who were diagnosed by echocardiography. First case was of a 76-year-old woman came with complain of dyspnea. Her transthoracic echocardiography findings were suggestive of severe aortic stenosis with membrane in right atrium. Second case was 68-year-old woman, her echocardiogram showed a membrane running from the lateral side of right atrium upto interatrial septum [5].
Schuchlenz HW et al., reported presence of persistent eustachian valve in 174 out of 306 patients [6]. Yavuz T et al., reported a case of giant eustachian valve that extended from orifice of Inferior Vena Cave(IVC) to the interatrial septum which appeared as a septal structure that divided right atrium into two halves [7].
In the process of embryogenesis, the smooth posterior portion of the right atrium is formed by the incorporation of the right horn of the sinus venosus into the right atrium whereas the trabeculated anterior portion is formed by original embryologic right atrium The connection between the right horn of the sinus venosus and the embryologic right atrium is the sinoatrial orifice, which is consists of two valvular folds (the right and left venous valves) on either side [8]. The right valve of the right horn of the sinus venosus divides the right atrium into two and this directs the oxygenated venous blood from the inferior vena cava to the left side of the heart during the foetal life [9]. Normally, the valve regresses by 10-12 weeks of gestation and leaves behind the crista terminalis superiorly and the eustachian valve of the inferior vena cava, and the thebesian valve of the coronary sinus inferiorly. It can be due to exaggerated foetal eustachian and thebesian valves, which together forms an incomplete septum across the lower part of the atrium [10].
The Fibroblast Growth Factor (FGF-8) is important for the expression of cardiac specific proteins; once cardiac tube is formed, venous portions are indicated by retinoic acid. Incorporation of sinus venosus into the right part of primitive atrium is under control of T-box transcription factor. So any alteration in either of the factors can be responsible for such type of variations [11].
Presence of such a membrane can be associated with ventricular septal and atrioventricular septal defect. Other anomalies like tetralogy of Fallot, double outlet right ventricle, coarctation of the aorta, partial anomalous pulmonary venous connection, and persistent left superior vena cava with unroofed coronary sinus, has also been described [12].
It has also been associated with foetal right ventricular hypoplasia and has been hypothesized to result from abnormal fetal circulation leading to growth restriction of the fetal right ventricle [13].
Conclusion
Cor triatriatum dexter is usually asymptomatic but the knowledge about presence of such membrane is important for physicians, as severe septation can cause right-sided heart failure and elevated central venous pressures. Early diagnosis will facilitate timely treatment of the defect.
[1]. García GM, Alonso DP, Guerrero AA, Cor triatriatum dexter in adulthoodCor Salud 2013 5(3):305-07. [Google Scholar]
[2]. Lasa JJ, Westover T, Khandelwal M, Cohen MS, Cor triatriatum dexter and right ventricular hypoplasia in a fetusJ Ultrasound Med 2011 30(12):1744-47.10.7863/jum.2011.30.12.174422124011 [Google Scholar] [CrossRef] [PubMed]
[3]. Jain A, Angel Kumar R, Persistent eustachian valve in adults: A cadaveric studyInternational Journal of Basic and Applied Medical Sciences 2013 3(3):132-37.10.4103/2229-516X.11710424083153 [Google Scholar] [CrossRef] [PubMed]
[4]. Zainudin AR, Tiong KG, Mokhtar SA, Cor triatriatum dexter: A rare cause of childhood cyanosisAnn Pediatr Cardiol 2012 5(1):92-94.10.4103/0974-2069.9372522529613 [Google Scholar] [CrossRef] [PubMed]
[5]. Juan A, Brotons S, Francisco J, Pardo L, María J, Puras R, Cor Triatriatum Dexter in adultsRev Esp Cardiol 2010 63(8):997-1003.10.1016/S0300-8932(10)70214-1 [Google Scholar] [CrossRef]
[6]. Schuchlenz HW, Saurer G, Weihs W, Rehak P, Persistent eustachian valve in adults: Relation to patent foramen ovale and CVAJ Am Soc Echocardiogr 2004 17(3):231-33.10.1016/j.echo.2003.12.00314981420 [Google Scholar] [CrossRef] [PubMed]
[7]. Yavuz T, Nazli C, Kinay O, Kutsal A, Giant eustachian valveTex Heart Inst J 2002 29(4):336-38. [Google Scholar]
[8]. Drake LR, Vogl AW, Mitchell AW, Gray’s Anatomy, The anatomical basis of clinical practice40th edChurchill Livingstone:1016-26. [Google Scholar]
[9]. Anderson RH, Understanding the nature of congenital division of the atrial chambersBr Heart J 1992 68(1):01-03.10.1136/hrt.68.7.11515284 [Google Scholar] [CrossRef] [PubMed]
[10]. Embrey RP, Cor triatriatum, pulmonary vein stenosis, atresia of the common pulmonary veinPediatric cardiac surgery 1994 2nd edSt LouisMosby-Year Book:503-04. [Google Scholar]
[11]. Sadler TW, Langman’s Medical Embryology 1990 6th edBaltimore MDWilliams & Wilkins:373-374. [Google Scholar]
[12]. Vaideeswar P, Tullu MS, Sathe PA, Nanavati R, Atresia of the common pulmonary vein: a rare congenital anomalyCongenit Heart Dis 2008 3(6):431-34.10.1111/j.1747-0803.2008.00225.x19037984 [Google Scholar] [CrossRef] [PubMed]
[13]. Fesslova V, Saracino A, Nuri H, Pomé G, Cor triatriatum dexter: unusual features in utero and after birthInteract Cardiovasc Thorac Surg 2012 14(3):330-32.10.1093/icvts/ivr09622159265 [Google Scholar] [CrossRef] [PubMed]