Imaging of soft tissue swellings is becoming more frequent as clinicians increasingly require good quality diagnostic information in order to determine clinical management [1]. Soft tissue masses have a varied presentation. Though all masses cannot be optimally imaged on Ultrasonography (USG), its easy availability, real time capability and cost effectiveness, as well as, the freedom it provides to be examined in any direction, makes it the investigation of choice as a first line of modality for superficially located masses [2].
Prime function of USG is to differentiate tumour from pseudotumour, followed by characterizing the lesion depending on its nature and its surrounding relations. Vascularity of the mass lesion is assessed with the help of Colour Doppler [2]. USG provides definitive characterization of solid and cystic mass lesions, their size and volume and compartmental localization of the mass lesion [3].
Application of high resolution USG in musculoskeletal system has evolved tremendously in the past two decades and is useful in not only evaluating the nature of soft tissue swellings but also aids in detection of histology in some cases [4].
Due to its inherent properties of being safe, low cost and real time imaging high resolution sonography is tailor made investigation for soft tissue swellings. Apart from providing the nature and characteristics of swelling, ultrasound guides the surgeon for appropriate surgical treatment with least complications [3]. The purpose of this study was to elaborate the preoperative sonographic features of superficial soft tissue swellings and compare it to the corresponding histopathological results.
Materials and Methods
This was a comparative prospective study conducted in the Department of Radiodiagnosis, KVG Medical College Sullia, Karnataka, India, on 100 subjects with superficial soft tissue swellings referred from various clinical departments. The sample size was determined by statistical analysis of existing data of prior referrals to the department. Ethical committee approval was obtained prior to the study. Informed consent was obtained from all the patients in their native language. Patients presenting with thyroid and breast swellings were excluded from the study. Study was conducted for a period of two years from October 2014 to October 2016.
All the soft tissue swellings were imaged by an experienced radiologist who was having an experience of 8 years with high resolution USG transducer of 6-12 MHz with GE Voluson 730 Pro. Patients were made to sit or lie down in supine or prone position depending on the location of the soft tissue swelling. The sonographic indices of the soft tissue swellings noted were location/plane, nature, size, margin, echo pattern and calcification. Vascularity of the lesions was assessed with colour and spectral Doppler parameters. Maneuvers such as panoramic views were obtained for large lesions for better assessment. The low frequency curvilinear transducer was also required for deep seated swellings of superficial origin.
The ultrasonographic diagnosis was then correlated initially on the clinical diagnosis. Soft tissue swellings such as foreign bodies and haematomas were readily confirmed to evaluate the accuracy of USG in these lesions. All patients with non inflammatory soft tissue swellings underwent histopathological examination either by biopsy or fine needle aspiration cytology, further treated with surgical excision. Patients with inflammatory soft tissue swellings were subjected to surgery [Table/Fig-1]. Probable diagnosis obtained by USG was then correlated with histopathology.
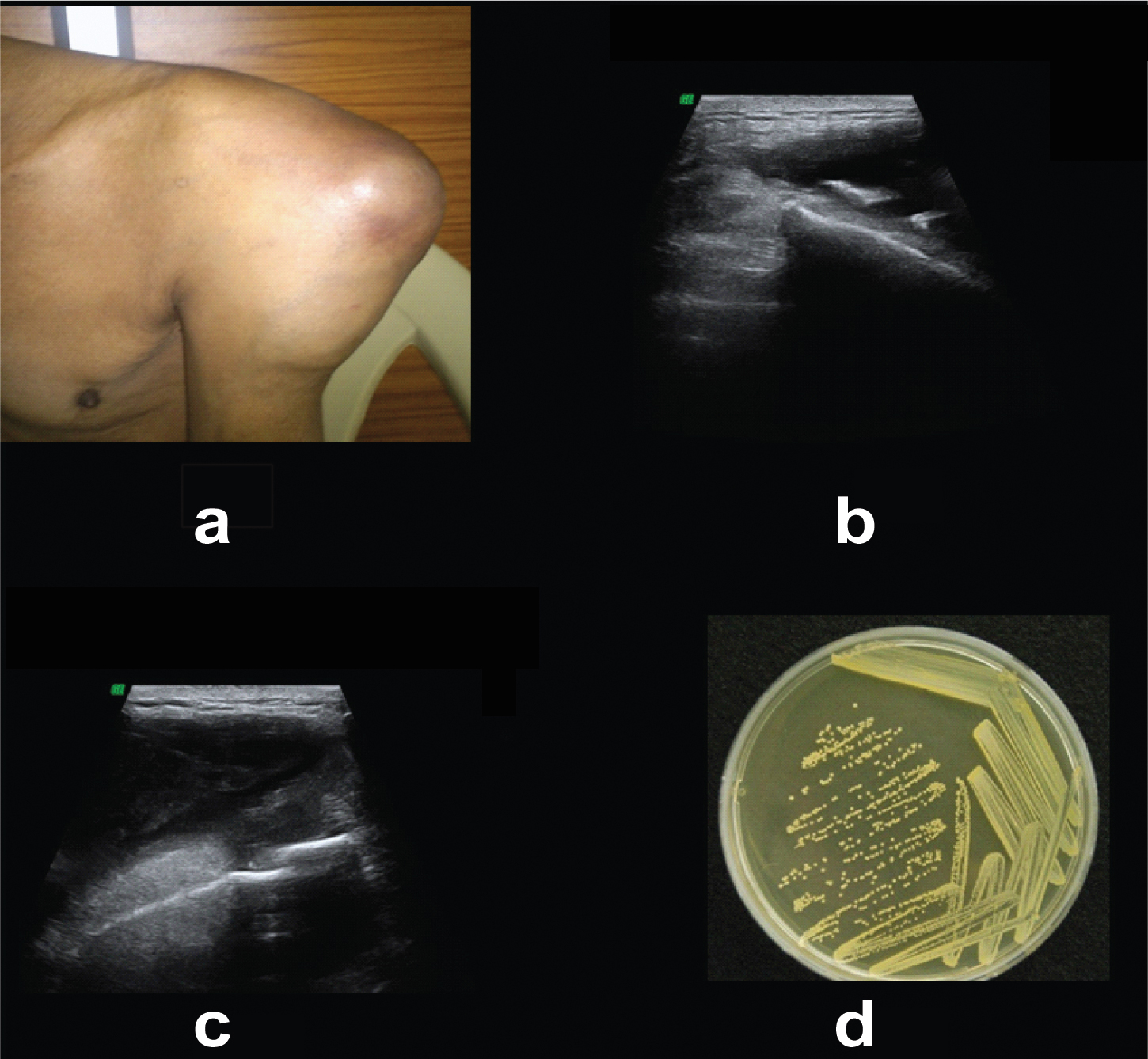
(a) Swelling and pus discharge over the back on the left side; (b,c) USG of swelling showed echogenic collection with dependent hyperechoic foci overlying the scapular bone with discontinuity of the cortex- Osteomyelitis; (d) Culture confirmed the diagnosis – Staphylococcus Aureus was isolated.
Statistical Analysis
The data obtained was statistically analysed using SPSS (Software Package used for Statistical Analysis) software version 16.0, Sensitivity, frequency and other appropriate statistical tests were calculated.
Results
In the current prospective study we obtained 100 subjects with superficial soft tissue swellings, out of which 59 were females and 41 were males. Subjects of varied age groups were included in the current study ranging from 10 years to 72-year-old. Maximum number of soft tissue swellings was obtained in the fourth decade and minimum number of soft tissue swellings was obtained in eighth decade. On distributing soft tissue swellings according to the anatomical plane of origin, maximum number of cases were observed in the subcutaneous plane (48) followed by muscular plane (28). Least cases were observed in the plane of skin (3). The remaining was in the deeper structures (21).
Sonographic features of swellings were evaluated for each soft tissue swelling. Depending on the nature of the swelling the lesions were classified into cystic, solid and mixed lesions. The current study depicted majority of solid lesions accounting for 61 cases followed by cystic (34) and mixed lesions (5).
Depending on the margins of the swelling, the lesions were classified into well defined, poorly defined, and lobulated and spiculated. The present study depicted majority of lesions with well defined margins (88) followed by poorly defined margins (11). Only one lesion had lobulated margins.
Based on the echo pattern of the swelling the lesions were divided into anechoic, hypoechoic, isoechoic, hyperechoic and heteroechoic. This study depicted majority of lesions were hypoechoic (37), closely followed by hyperechoic (28) heteroechoic (23), anechoic (10) and Isoechoic (2) lesions. Depending on the vascularity of the soft tissue swellings, on colour Doppler the lesions were divided into nonvascular, minimally vascular, profoundly vascular and peripherally vascular lesions. Most of the lesions were avascular (49), minimally vascular (41), profoundly vascular (07) and peripherally vascular (03).
Lesions were divided according to the presence or absence of calcifications within the lesion. If the calcifications were present they were further subdivided into micro and macro calcifications. In our study non calcific soft tissue lesions were in high majority accounting for 89 lesions. Among the remaining (5 lesions) showed microcalcifications and (6 lesions) showed macro calcifications.
Another way of classifying soft tissue swellings were Tumoural and Non Tumoural. Non Tumoural swellings had upper hand in the current study comprising of 76 of cases, where as Tumoural soft tissue swellings were 24 in number. Non Tumoural soft tissue swellings were sub classified as cystic, post traumatic and reactive/inflammatory. Reactive/inflammatory soft tissue swellings stood the majority with 45 lesions, followed by cystic swellings (21) and post traumatic (10).
Among the non tumoural soft tissue swellings, the most important one was foreign bodies in soft tissues with its complications. There were a total of 11 cases of soft tissue foreign bodies with granuloma /abscess formation. Six cases were obtained in the upper limb and remaining five was in the lower limb. All 11 foreign bodies were echogenic with variable shadowing and were readily detected on USG. Eight foreign bodies turned out to be wooden material, two metal and one plastic.
Ganglion cysts were one of the common cystic swellings in the present study along with branchial and dermoid cysts. Four ganglion cysts were obtained, two each in both the hands. Of these, three were present in the palmar aspect and one in the dorsal aspect. Palmar ganglion cysts were hypoechoic on ultrasound, where as the cyst in the dorsal aspect of the hand was anechoic.
According to the recent WHO classification amended in 2013, there are 10 different categories of tumours depending on the origin of tissue. Current study depicted maximum number of adipocytic tumours accounting for 16. This was followed by the neural origin tumours which were five in number. Only one malignant soft tissue swelling was obtained in the present study which was metastatic melanoma in the scalp.
Among the Tumoural soft tissue swellings adipocytic tumours (lipoma) were most common. Out of 24 tumoural soft swellings 16 were lipoma, followed by nerve sheath tumours (5). On subdivision of lipoma based on their location in the body; nine were in the torso followed by four in the lower limb. Eight lipomas were hypoechoic with echogenic septations, seven were homogenously hyperechoic and one was isoechoic.
Soft tissue swellings diagnosed by USG were correlated with their histopathological (HPE) and surgical diagnoses [Table/Fig-2]. In accordance with above mentioned results the sensitivity of the study was 97% with confidence interval of 91.48% to 99.38%. The positive likely hood ratio was 0.97. Positive predictive value of the study was 100% with confidence interval of 96.27% to 100% [Table/Fig-3].
Correlation between the USG with their histopathological and surgical diagnosis.
| Diagnosis By USG | No. | Concordant With HPE/Surgery | Discordant with HPE/Surgery and diagnosis |
|---|
| Lipoma | 16 | 16 | |
| Lymphadenopathy | 8 | 8 | |
| Tenosynovitis | 7 | 7 | |
| Foreign body/Foreign body inflammatory reaction | 11 | 11 | |
| Branchial cyst | 6 | 6 | |
| Sebaceous cyst | 5 | 5 | |
| Muscle haematoma | 5 | 5 | |
| Dermoid | 4 | 4 | |
| Abscess | 4 | 4 | |
| Ganglion | 4 | 4 | |
| Osteomyelitis | 4 | 4 | |
| Nerve sheath tumour | 3 | 3 | |
| Pleomorphic adenoma | 2 | 2 | |
| Bursitis | 2 | 2 | |
| Abscess/ haematoma | 1 | 1 | |
| Achilles tendinosis | 1 | 1 | |
| Epidermal cyst | 1 | 1 | |
| Haemangioma | 1 | 1 | |
| Haematoma | 1 | 1 | |
| Infective collection | 1 | 1 | |
| Intramuscular myxoma | 1 | 0 | 1-Arteriovenous malformation |
| Intramuscular haematoma | 1 | 1 | |
| Lipoma /neurofibroma | 1 | 0 | 1-Liposarcoma |
| Lymphadenopathy with abscess | 1 | 1 | |
| Melanoma metastasis | 1 | 1 | |
| Parotid collection | 1 | 1 | |
| PNST – schwanoma | 1 | 1 | |
| Rectus muscle tear with haematoma | 1 | 1 | |
| Submandibular mass | 1 | 0 | 1-Sialadenitis |
| Synovitis with collection | 1 | 1 | |
| Tonsillar abscess | 1 | 1 | |
| Urachal cyst | 1 | 1 | |
| Carotid body tumour | 1 | 1 | |
PNST - peripheral nerve sheath tumour
Sensitivity, Specificity, PPV of the current study.
| Value | Confidence interval |
|---|
| Sensitivity | 97% | 91.48% to 99.38% |
| Positive predictive value | 100% | 96.27% to 100%. |
| Positive likely hood ratio | 0.97 | |
Discussion
Superficial soft tissue swellings comprise a wide spectrum of swellings which can be primarily classified into various types based on their origin, histological type, USG features and anatomical location. In the recent past, the ability of USG to assess and diagnose a superficial soft tissue swelling has greatly increased, as technology has advanced by leaps and bounds and so is the knowledge and confidence of radiologists to ascertain a narrow differential diagnosis. USG has always been a preferred modality due to its advantages of low cost, non invasiveness, easy availability, patient comfort, no harmful radiation and faster reporting.
USG is a low cost, non invasive, readily available, safe and a patient comfortable modality which has high specificity and predictive value to diagnose superficial soft tissue swellings and it wouldn’t be erroneous to infer that USG is almost equivalent to the pathological diagnosis especially in non tumoural superficial soft tissue swellings.
In this prospective study 100 subjects were enrolled, out of which 59 were females and 41 were males. Subjects of varied aged group were included in this study ranging from 10 years to 72-years of age with a mean of 39.9 years. Various retrospective studies done by different regions of the world also showed similar variations in the age groups in soft tissue swellings. Hung E et al., conducted a retrospective study in Hong Kong on 247 soft tissue tumours superficial to the investing fascia [5]. In his study the age group varied from 1-96 years. Another retrospective study performed by Hong-Jen Chiou et al., on superficial soft tissue masses in Taipei enrolled patients with age group from 1 to 104 years [6]. Ju-Wen Cheng et al., conducted a retrospective study of sonographic features of soft tissue tumours in hand and forearm [3]. In his 31 cases the age group of the patients varied from 22-72 years. Hence, by correlating with these above mentioned studies we can conclude that superficial soft tissue swellings have a varied age group of presentation, youngest being one-year-old upto a grand old age. With reference to the above studies and results of current study it can be concluded that there is no significant gender distribution of superficial soft tissue swellings.
Based on the present study and with comparison with previous studies conducted by Hung E et al., and Hong-Jen Chiou et al., the most common site of presentation of superficial soft tissue swelling was the upper limb and the second most common in our study was the torso due to inclusion of inflammatory/reactive swellings [5,6]. The most common swelling was lipoma.
Amended version of WHO classification of tumours of soft tissues and bone was published in 2013 [7]. This classification helps to classify and understand pathogenesis, histological and genetic findings of tumours. In the current study out of 100, 24 soft tissue tumours were enrolled, among which adipocytic tumours predominated accounting for 66%.
Characterization of the swelling and getting to a narrow differential diagnosis and further the definite diagnosis was made by various ultrasound examination parameters. In the current study, the main parameters about the swelling recorded were its plane, nature, margins, echopattern, vascularity and presence or absence of calcification. We observed that no single soft tissue swelling had specific parameters through which it can be diagnosed. Also, no single parameter can suffice to diagnose a swelling. It is a combination of all the parameters with other variables that specifies a diagnosis. All swellings in each parameter were variable. The diagnosis was made by considering clinical history, demographics and by using variable parameters of which the ultrasound parameters were a part of.
Hong-Jen Chiou et al., in his study opined that there was no significant difference between the malignant and benign soft tissue tumours based on USG and Doppler parameters [6]. Hung E et al., had a different conclusion that differentiation between benign and malignant tumours on USG parameters is pretty high [5]. No previous study has interpreted the specificity of USG parameters in the diagnosis of non tumoural lesions. Our study had a majority of non tumoural lesions. So, with these studies and our study we may conclude that USG and Doppler parameters alone are not adequate to make a specific diagnosis of superficial soft tissue tumours and also nor is any single parameter of help for the same. Tumoural soft tissue swellings may relatively have USG parameters that differentiate benign and malignant.
Lipoma was the most common benign tumour encountered as soft tissue masses. These tumours often are located in the subcutaneous plane, though intra muscular and inter muscular planes aren’t infrequent. On USG, most of the lipomas are homogenously hyperechoic relative to the surrounding structures. Peculiar pattern of echogenic parallel lines was also depicted by these tumours. However, some of the lipomas may be hypoechoic or even isoechoic to the surrounding structures. Out of 16 lipomas in the current study 8 were homogenously hyperechoic, 7 were hypoechoic with parallel echogenic lines and one was isoechoic. Ju-Wen-Chang et al., in his study had 6 lipomas in which 5 were hyperechoic and 1 was isoechoic [3]. In contrary Hong-Jen Chiou et al., in his study had 66 lipomas among which 26 were heterogenously hypoechoic and 40 were heterogeneously hyperechoic [6]. Even in his study 59 lipomas showed parallel echogenic lines.
We may infer that lipomas have an echogenic pattern ranging from hyperechoic to hypoechoic with parallel echogenic lines being a characteristic feature.
Neurofibromas and schwanommas are the two most common neural tumours presenting as soft tissue swellings. Both the tumours are heterogeneous and predominantly hypoechoic. Current study comprised of four nerve sheath tumours among which three were diagnosed on USG and one was discordant. Among the 3 tumours diagnosed on USG, 2 originated from ulnar nerve and one from the median nerve [Table/Fig-4]. Out of the three, two tumours were heterogeneously hyper echoic and one was hypoechoic. The discordant mass lesion was also hypoechoic on USG.
A 50-year-old male patient presented with a swelling in the right distal forearm: (a,b) Well defined ovoid solid mass lesion deep to the subcutaneous tissue in the flexor aspect of distal forearm proximal to the wrist contiguous with the median nerve (White Arrow)- Peripheral Nerve Sheath Tumour; (c) Biphasic pattern with both Antony A and Antony B fibers confirmed the diagnosis. (Stain – H&E stain, Magnification – 40X).

Ju-wen-Chang et al., had six nerve sheath tumours and all of them were heterogeneously hypoechoic solid masses [3]. Hong-Jen Chiou et al., enrolled 11 nerve sheath tumours among which nine were solid with heterogeneous hypo echogenicity [6]. Two nerve sheath tumours showed solid and cystic changes. Sixteen nerve sheath tumours accounted in the superficial soft tissue tumour study conducted by Hung E et al., [5]. The study showed accuracy of 69% with 5 incorrect diagnoses. Even in his study most of the tumours were heterogeneously hypoechoic. In the present study the diagnosis of nerve sheath tumour was entertained primarily due to the ‘exiting and entering’ phenomenon . With these results it can be concluded that on USG, features of nerve sheath tumour are non specific with varied echogenicity. The diagnosis can be entertained primarily due to the proximity to the nerves or the nerve running through the mass lesion.
Non tumoural swellings predominated in the current study costing for 76% of the cases. These non tumoural swellings were sub classified into cystic (27.6 %), post traumatic (13.15 %) and inflammatory/reactive (59.2 %). Soft tissue foreign bodies and its complications are very commonly encountered in day to day practice of USG referred by various surgical departments especially in the rural population. Secondary to the availability of high resolution USG probes and sophisticated softwares, it is a cake walk to diagnose soft tissue foreign body and its complications. Eleven cases of soft tissue foreign body with granuloma/abscess formation were enrolled in the current study among which 6 were in the upper limb and 5 in the lower limb. All the eleven cases were confidently diagnosed on USG with sensitivity of 100%. Foreign bodies seen as linear or punctate echogenic lesions with variable acoustic shadowing surrounded by hypoechoic granulation tissue or abscess formation.
A study conducted in a rural Indian center by Sonali et al., on 123 patients showed similar high sensitivity corresponding to 94.5% [8]. Majority of the composition of the foreign body was wood (8) in the current study followed by metal pieces (2). Even in the study conducted by Sonali et al., 82% of foreign bodies were wooden in nature and 99% were in the extremities [8].
With reference to the above study we can conclude that foreign bodies are usually identified as hyperechoic structure with variable acoustic shadowing with surrounding hypoechogenicity suggestive of abscess or granuloma.
Ganglion is a cystic mass lesion and may present as unilocular or multilocular cystic lesion with myxoid matrix. Four ganglion cysts were obtained in the current study of which three were hypoechoic and one was anechoic. A prospective study was conducted by George Wang et al., on 20 wrist ganglia [9]. Fifteen cysts were in the volar aspect and 5 in the dorsal. Among 20, ten were anechoic, 7 hypoechoic and 3 were depicting mixed echogenicity. With the reference to the above, ganglion cysts can present in both the dorsal and palmar aspects. They can present as hypoechoic, anechoic and rarely with mixed echogenicity [Table/Fig-5].
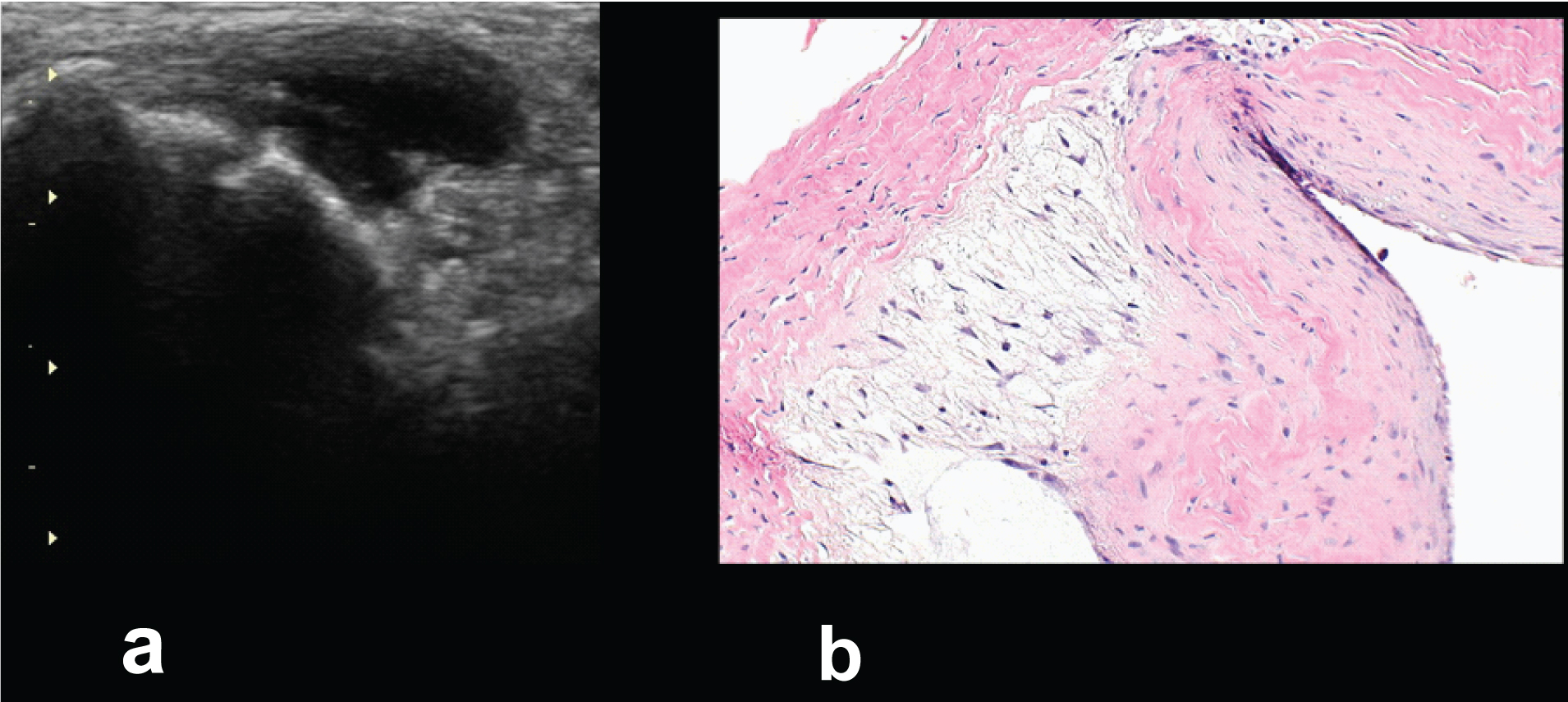
A 29-year-old female presented with a swelling in the left wrist: (a) USG wrist showed thick walled cystic structure in the dorsal aspect of left wrist joint along the extensor carpi brevis tendon- Ganglion Cyst; (b) Pathological slide showing features of Ganglion Cyst. (Stain – H&E stain, Magnification – 40X).
Hung E et al., had similar results for the USG diagnosis of soft tissue tumours superficial to the investing fascia with a sensitivity and specificity of 95.2% and 94.3% respectively for lipoma; 73% and 97.7% for vascular malformation; 80% and 95% for epidermal cyst and 68.8% and 95.2% for nerve sheath tumour [5]. The high sensitivity obtained in the current study could be due to majority of non tumoural lesions (inflammatory and cystic lesions).
Limitation
The possible limitations of the current study were a majority of the lesions were inflammatory/reactive. Therefore, the conclusion of our study on soft tissue tumours may be subjected to further evaluation. Also, ultrasound contrast and elastography were not part of the study which if used would possibly widen the spectrum of collection of data (USG features), results and diagnosis.
Conclusion
With this elaborate discussion we may conclude that USG is capable of diagnosing superficial soft tissue swellings but no single parameter such as demographics, location and individual USG parameter is sufficient enough to specify USG diagnosis. With all parameters complimenting each other, USG has a high specificity to accurately diagnose superficial soft tissue swellings.
PNST - peripheral nerve sheath tumour