We preface that CAD is a chronic degenerative condition of arteries responsible for significant cardiovascular morbidity and mortality. It is complicated by myocardial infarction stroke, embolisation, thrombosis and aneurysm [1].
Recent study has shown that the incidence of acute myocardial infarction is on the increase in developing countries such as Nigeria, because of rapid urbanisation with its tendency to a sedentary habit, western type dietary habit, obesity and the scourge of hypertension and diabetes related hypercholesterolaemia [2].
Studies done in Sub-Saharan Africa between the 1940s and 1970s had shown that CAD and its complications were extremely uncommon [3-6]. However, more recent reports indicate that CAD is now more frequently recognised in Nigeria, although the incidence is still low compared with previous studies done in developed countries [7-13].
Major advances in surgical, medical and interventional therapy have resulted in improvement in quality of life of most patients with CAD. However, in spite of these innovations, the prevalence of CAD still appears to be on the high side [14]. In western countries it accounts for 50% of all deaths in middle aged and the elderly [15,16]. In Asia and other Middle East countries including Africa, it is the leading cause of deaths [17].
The exact global incidence of coronary atherosclerosis is extremely difficult to calculate and where available, the figures are extremely variable [17]. Since, some of the cases could be asymptomatic, these fatal asymptomatic cases can only well be determined in an autopsy study [18,19]. Vyas P et al., reported that assessment of atherosclerotic lesion in living patients appears difficult and expensive due to its invasiveness and that autopsy based studies have proven to be a reliable and valuable method for studying these lesions in deceased patients [1]. The aim of this study is to determine the prevalence of fatal myocardial infarction in Lagos, Nigeria and to observe the morphological patterns of deaths resulting from myocardial infarction in all the autopsies done in the last eight years in our centre.
Materials and Methods
This was an eight year (January 2008 to December 2015) retrospective study of all autopsy cases in which deaths were caused by fatal myocardial infarction following coronary atherosclerosis. The autopsies were conducted in the Department of Pathology and Forensic Medicine, Lagos State University Teaching Hospital, Ikeja, Lagos, Nigeria. Consent for this study was sought and approval was given by the Department of Pathology and Forensic Medicine.
The standard routine autopsy and dissection method were followed during these autopsies. The coronary arteries were dissected and sectioned at 5.0 mm interval. The percentages of occlusions were noted with the aid of hand lens and degrees of narrowing recorded in each of the three coronary arteries namely; Left Anterior Descending (LAD) coronary artery, Left Circumflex Artery (LCA) and Right Coronary Artery (RCA). A grading system previously used by Prabhu MH et al., in India was adopted for classification of the level of occlusion [19]. It comprises five grades: Grade-0: Normal, Grade-I: 1-25%; Grade-II: 26-50%, Grade-III: 51-75% and Grade -IV: 76-100%.
The autopsy reports of these cases where deaths were caused by fatal myocardial infarction following coronary arteriosclerosis were retrieved. The level of occlusion of the three coronary arteries was recorded in a predesigned form. Heart weights in excess of 300 gm and 350 gm for females and males respectively were classified as hypertensive heart disease. In addition, for genders, papillary muscle thickness on the left side and left ventricular wall thickness in excess of 1.5 cm was regarded as hypertensive heart disease. Other causes of cardiomegaly such as valvular diseases or cardiomyopathy were excluded from the study.
Other parameters extracted included the age, sex, weight of the heart, evidence of old infarct and any other contributory disease seen at autopsy where applicable, clinical evidence of accompanying illness such as diabetes mellitus was retrieved from the clinical notes.
Statistical Analysis
The data retrieved were analysed using the SPSS Software version 20. These were presented in tables, percentiles, pie charts and bar charts. Chi-square was used to test for level of significance and p-value of <0.05 was considered to be statistically significant.
Results
A total of 79 cases of myocardial infarction deaths spanning the period of eight years from (January 1st, 2008 to December 31st, 2015) were seen out of 8334 autopsies performed which represents 0.9% of the total autopsy cases during the period of study. The autopsy rate in our centre is 38.6% of the total hospital deaths. The age range of deaths from myocardial infarction was from 27 to 80 years with mean age of 57±10 years. The females were more affected with a male to female ratio of 1:3.4.
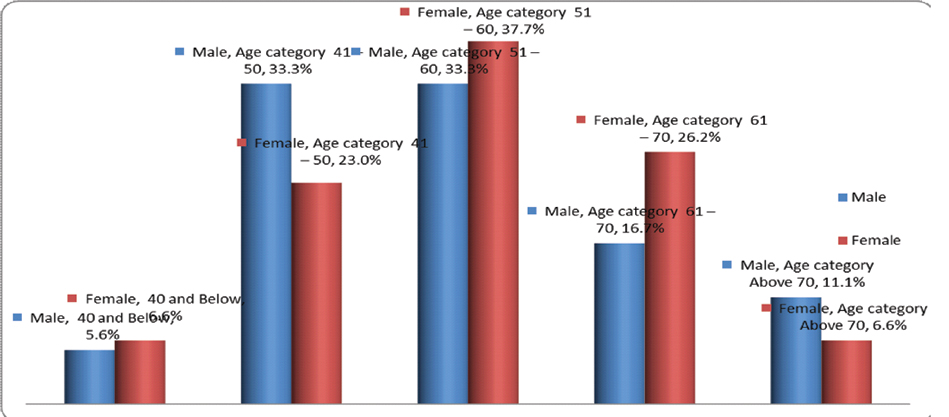
The highest incidence of myocardial infarction occurred in the sixth decade while the lowest occurred before the third decade. In addition, the incidence increased with each decade reaching a maximum in the sixth decade and began to fall steadily from the sixth decade [Table/Fig-1]. In all the age groups there was a female predominance except the fifth and eighth decades which revealed a slight increase in incidence among males over females. This value showed no statistical significance. p=0.81 [Table/Fig-2].
Demographic profile of the participants.
| Parameter | Frequency | Percentage (%) |
|---|
| Gender |
| Male | 18 | 22.8 |
| Female | 61 | 77.2 |
| Total | 79 | 100.0 |
| Age (years) |
| 40 and Below | 5 | 6.3 |
| 41–50 | 20 | 25.3 |
| 51–60 | 29 | 36.7 |
| 61–70 | 19 | 24.1 |
| Above 70 | 6 | 7.6 |
| Total | 79 | 100.0 |
Distribution of frequency and age with gender in decades.
The [Table/Fig-3] shows the grade of the atherosclerosis in each of the three epicardial coronary arteries. The most common grade in the LAD was Grade IV while Grade I occurred as the most common in the RCA and LAD coronary artery. Of those with occlusion of the LAD, 46.8% had a Grade IV occlusion.
Grades of Atherosclerosis.
| LAD | N (%) | RCA | N (%) | LCA | N (%) |
|---|
| Grade I | 32 (40.5) | Grade I | 51 (64.6) | Grade I | 67 (84.8) |
| Grade II | 6 (7.6) | Grade II | 3 (3.8) | Grade II | 3 (3.8) |
| Grade III | 4 (5.1) | Grade III | 4 (5.0) | Grade III | 2 (2.5) |
| Grade IV | 37 (46.8) | Grade IV | 21 (26.6) | Grade IV | 7 (8.9) |
| Total | 79 (100.0) | Total | 79 (100.0) | Total | 79 (100.0) |
LAD=Left Anterior Descending Coronary Artery
RCA=Right Coronary Artery
LCA=Left Circumflex Artery
Of all the three epicardial coronary arteries, the LAD was the most commonly involved (59.5%), this was followed by RCA (12.7%) and lastly the LCA (2.5%). Furthermore, in this study, single vessel involvement as a cause of myocardial infarction was the most common (LAD 59.5%) with double vessels and triple vessels accounting for (12.7%) and (10.1%) respectively [Table/Fig-4].
Table showing the frequency and combination of arteries involved in myocardial infarction.
| Atherosclerosis | Frequency | Percent (%) |
|---|
| LAD only | 47 | 59.5 |
| LCA only | 2 | 2.5 |
| RCA only | 10 | 12.7 |
| LAD and LCA | 2 | 2.5 |
| LAD and RCA | 10 | 12.7 |
| LAD, LCA and RCA | 8 | 10.1 |
| Total | 79 | 100.0 |
LAD=Left Anterior Descending Coronary Artery
CRA=Right Coronary Artery
LCA=Left Circumflex Artery
The [Table/Fig-5] shows evidence of old infarct, hypertension and clinical evidence of accompanying diabetes mellitus. Only 48.1% and 64.6% of study population had accompanying old myocardial scars and hypertensive heart disease respectively and only 6.3% had accompanying diabetes mellitus.
Table showing other associated conditions with the myocardial infarction.
| Chronic MI | N (%) | HHD | N (%) | DM | N (%) |
|---|
| Absent | 41 (51.9) | Absent | 28 (35.4) | Absent | 74 (93.7) |
| Present | 38 (48.1) | Present | 51 (64.6) | Present | 5 (6.3) |
| Total | 79 (100.0) | Total | 79 (100.0) | Total | 79 (100.0) |
Chronic MI=Chronic Myocardial Infarction; HHD=Hypertensive Heart Disease
DM=Diabetes Mellitus
Discussion
One of the major and catastrophic manifestations of coronary atherosclerosis is myocardial infarction. This is a common contributor of mortality and morbidity worldwide. For example, the incidence of coronary atherosclerosis has doubled during the past three to four decades in India and will soon emerge as the single largest disease accounting for almost one-third of all deaths in India [20]. Similarly, the incidence of myocardial infarction has been shown to be on the increase in Nigeria due to its rapid urbanisation and adoption of the Western diets [2]. In investigating this disease, autopsy has proven to be a reliable and valuable method [18,19].
One of the aim of the present study was to assess the prevalence rate of myocardial infarction at autopsy in this centre. The prevalence rate of myocardial infarction in this study was 0.9 % and this is lower than 2.6 % from the findings of Oke DA and Adetola AP in Lagos, Nigeria [10]. A similar eight-year clinicopathological study (1992-1999) in South Nigeria reported a prevalence of 1.6% which is fairly close to the findings of our study [21]. The mean age as seen in this present study was 57±10 years. This is closely in tandem with that of the previous study by Essien OK et al., which reported 51.3±8.3 and of 53.6±12.8 for males and females respectively [21].
The prevalence in this study is also closely compatible with the works of Edington GM, Florentin RA et al., and Williams AO who all observed myocardial infarction to be extremely uncommon in Africa [4-6]. It is worthy of note that our prevalence of 0.9% in this study is less than what was obtained in the Asia which ranged from 9.72% to 10.8% [22]. Hertz JT et al., did a systematic review on the trend in the prevalence of acute myocardial infarction in sub Saharan Africa and found a wide range of prevalence varying from 0.1% in Senegal to 10.4% in Sudan [23]. Similarly, Maru M, reported a prevalence of 6.5% in Ethiopia [24]. The varying prevalence rate might be due to the heterogeneity of the study population. Various studies outside African continent especially in India, Asia have reported rates between 3.0% and 10.8% [1,20,22].
Our study revealed an increasing incidence of myocardial infarction with age and it was most common in the sixth decade with a decline afterwards. This finding is compatible with previous studies in India [14,19,20]. Dauntingly, we found a female preponderance with a female to male ratio of 3.4:1 which was in contrast to many other studies which reported a high male to female ratio [7,6,14,24]. The reason why more women died of myocardial infarction in this centre is unknown. This we believe could be due to the fact that the level of oestrogen in the premenopausal years which offers protection against myocardial infarction declines drastically after the fifth decades and could probably explain the high prevalence in the older age groups in this study.
Of all the three epicardial coronary arteries, the LAD was the most commonly involved (59.5%), this was followed by RCA (12.7%) and lastly the LCA (2.5%) in this study. This is in concordance with previous other studies [14,25,26]. We also found out that single vessel involvement as a cause of myocardial infarction was the most common (LAD 59.5%) with double vessels and triple vessels involvements accounted for 12.7 % and 10.1% respectively. This findings of Dhruva GA et al., and Virmani R et al., greatly corroborated our observations [22,27]. However, the works of Agravat HA et al., and Yadzdi SA et al., gave a different pictures and all showed triple vessels as the most common [14,26].
It is not unusual for patients who suffered from fatal Myocardial infarction to have had past episode of myocardial infarction. About half (48.1%) of our study population had evidence of Chronic myocardial infarction (old scar). This figure is quite higher than the work of Vyas P et al., who reported a chronic MI rate of 13.25% [1]. Associated Diabetes Mellitus (DM) was seen in 6.3% of cases while 64.6% showed accompanying hypertension. Previous studies have shown that individuals with Diabetes mellitus have increased risk of CAD morbidity and mortality, they also revealed that absolute risk of death was higher for DM than non-DM patients [28-30].
Limitation
A major limitation in this study is the absence of the premorbid states and clinical history of these patients. Since, most were Brought-in-Dead (BID) or found dead, information such as antihypertensive drug usage, anti-lipid drugs compliance or hypoglycaemic agents were unknown.
In addition, we could not determine whether the infarction was commoner in the anterior or posterior wall since it was a retrospective study.
Conclusion
The outcome of this study revealed a prevalence of 0.9% with highest incidence in the sixth decade. There was female predominance with myocardial infarction. Involvement of single artery (LAD coronary artery) was the commonest in this study while approximately half of the deceased had concomitant old myocardial scars. A future study to find the reason for this new development of female preponderance is advocated considering that most studies within and outside the country have reported male preponderance.
Abbreviations
MI: Myocardial Infarction
BID: Brought–In-Dead
LAD: Left Anterior Descending coronary artery
LCA: Left Circumflex Artery
RCA: Right Coronary Artery
LAD=Left Anterior Descending Coronary Artery
RCA=Right Coronary Artery
LCA=Left Circumflex Artery
LAD=Left Anterior Descending Coronary Artery
CRA=Right Coronary Artery
LCA=Left Circumflex Artery
Chronic MI=Chronic Myocardial Infarction; HHD=Hypertensive Heart Disease
DM=Diabetes Mellitus