Pregnancy is a physiologic state which induces many multiorgan changes. Increased water retention in all organs is partially due to decreased plasma osmolality [1,2].
Water retention during late pregnancy is nearly 6.5 liters divided into 3 liters each in blood circulation, gravid uterus and breasts, and another 3.5 liters in uterine pregnancy content. Water retention in pregnancy results in oedema in dependent areas of the lower extremity, which is more prominent in the evenings. The pathophysiology of this phenomenon is mostly a partial obstruction of venous return [3]. The role of hormonal changes in fluid retention during pregnancy should also be mentioned [4]. The changes and side effects in visual system in pregnancy sometimes indicate systemic disturbances [5].
RNFL is located in the undersurface of the retina. This layer includes axons which come from the neural cells of the retina. In many diseases, the optical review of RNFL is clinically usefull [6-9]. OCT is helpful and a new technology for the determination of RNFL thickness. Practically, in summarising the characteristics of OCT, it has high-resolution (3-10 μm longitudinal resolution), is non-invasive, time saving and has on-line modality which provides new information in comparison with other conventional methods [10]. OCT measures RNFL thickness by identifying the RNFL as a highly reflective layer under the retinal surface and change in thickness is used as a biomarker for axonal damage [11]. The use of OCT is on increase when it comes to daily ophthalmology practice for the determination of optic nerve and retinal physiologic and pathologic states [12]. This new method in pregnancy might help clarify retinal oedema, probably due to increased fluid retention in this area in comparison with other body organs [13].
Therefore, the aim of the present study was to assess the change in thickness of RNFL in healthy women during pregnancy and postpartum, by means of OCT.
Materials and Methods
The study was designed as a prospective cohort study, conducted at the Department of Obstetrics and Gynaecology in collaboration with Department of Ophthalmology of Imam Hossein Medical Center affiliated to Shahid Beheshti University of Medical Sciences, Tehran, Iran, between April 2013 and March 2015.
The study followed the principles of the declaration of Helsinki and was approved by the Medical Ethics Review Board of Shahid Beheshti University. Written informed consent was obtained from the volunteers regarding confidentiality and anonymity of data collected, also details and purpose of the study were disclosed.
From April 2013 to July 2015, 43 out of 157 pregnant women (16 to 38-year-old) with 28 weeks or more gestational age until maximum 48 hours postpartum, who referred to the Obstetrics and Gynaecology Department, were included in the study.
Gestational age was based on the precise data of the last menstrual period and/or ultrasound gestational age measurement in the first trimester.
Potential participants were clinically examined and excluded in case of history of any medical or obstetrical problems, taking any medication or prediagnosed with hypertension, diabetes or other systemic disease and lack of informed consent and/or authorisation form to the processing of personal data. Finally, demographic data collection form was completed for each participant.
Ophthalmologic Examination
All women in pregnant period underwent a comprehensive ophthalmologic examination and RNFL thickness measurement by OCT, using an automatic Topcon model device and analysis was done using OCT software in four quadrants. After delivery, all studied women were called at least three times for the second OCT analysis. Above mentioned assessment was repeated, once again during 2 to 8 months in postpartum period. Two months time period was selected due to complete regression of pregnancy-induced changes. All measurements were carried out by the same professional. RNFL thickness as main outcome was compared during pregnancy and 2-8 months after delivery.
Statistical Analysis
Statistical analyses were done by using the program SSPS version 17.0 (SPSS, Inc., Chicago, IL, USA). Because all quantitative parameters according to the Kolmogorov-Smirnov test had normal distribution, paired t-test was used for comparison of continuous parameters between the two assessments, respectively. The results were expressed as mean±Standard Deviation (SD), and/or range (minimum–maximum). A p-value less than 0.05 was considered statistically significant.
Results
A total of 43 women were included in the analysis, of which 32 came back for follow up. The study group included 64 eyes of 32 women. None of the patients had retinopathy, retinal haemorrhages and optical papilloedema.
The mean age of the studied women was 26.2±5.7 years and the median age was 25 (16-38) years. The mean gestational age in the primary exam (during pregnancy) was 36.5±2.4 weeks and median gestational age was 37 (31-40) weeks.
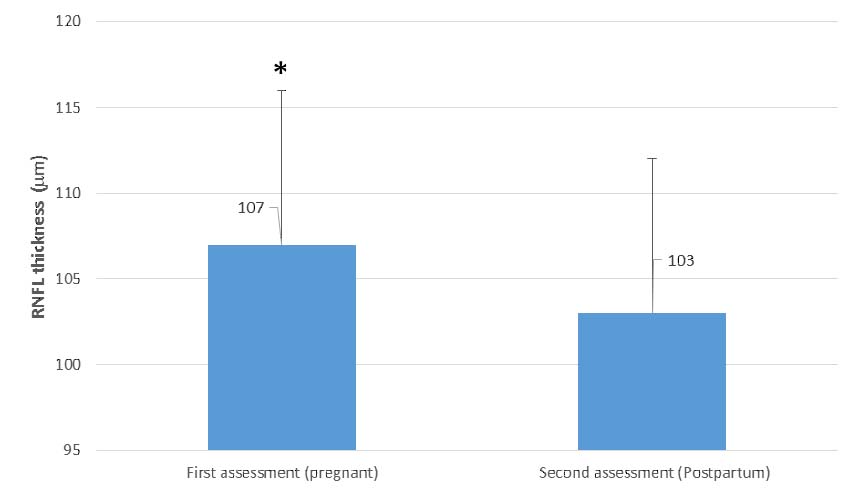
Mean and median of RNFL thickness were 107±9 μm and 106 μm (81-123) during pregnancy and 103±9 μm and 102 μm (80-130) in postpartum period, respectively (p=0.013). The second visit was prepared at least two months after delivery; so that the regression of pregnancy induced changes occur, until 8 months after delivery.
Mean RNFL thickness in the first (during pregnancy) and second assessments (2-8 months after delivery) are presented in [Table/Fig-1].
Comparison of RNFL thickness during pregnancy and postpartum period.
*Significant in p=0.013
t-test
Discussion
Pregnancy involves an extensive change of state in all body systems, of which progressive oedema is specific and supportive to this physiologic state. These physiologic changes are observed in all organs, including cardiovascular, renal, pulmonary, immunologic and visual [14,15]. Among the main systems involved by pregnancy, visual system is mentioned. Increased pigmentation in the skin around the eye, melasma, chloasma, dry eye syndrome, decrease in corneal sensitivity, increase in corneal thickness due to oedema, are reported eye changes during pregnancy [16-19]. In the present study, RNFL was significantly thicker in late pregnancy in comparison with 2-8 months postpartum period, indicating thicker RNFL in pregnancy as oedema observed in all other organs.
Another case-control study by Demir M et al., compared 40 healthy pregnant women with 37 non pregnant women as control. In this study, RNFL thickness was similar in two groups. Mean intraocular pressure was higher in the control group with probable impact on RNFL thickness [13]. In our study design, re-evaluation of the same population with no intraocular pressure difference, clarified more RNFL thickness in pregnancy with regression in postpartum period.
In clinical practice the finding of thicker RNFL in pregnancy might be helpful in diagnosis of retinopathy in some chronic diseases including diabetes and hypertension. Decreased thickness of RNFL thickness in these chronic diseases might be misdiagnosed in pregnancy due to pregnancy induced increased thickness [20-24].
Diabetes is the most common medical disease co-existing with pregnancy and had shown a significant increase, from 1989 to 2004. In 4.2% of American pregnant women, diabetes was diagnosed [25]. Existing diabetic retinopathy might progress during pregnancy, probably due to tight control recommended in pregnancy. McElvy SS et al., reported 30% progression of retinopathy in studied pregnant women [26]. Park HYL et al., compared 40 normal individuals, 37 diabetic without retinopathy and 89 diabetic with retinopathy patients. In all the patients, OCT was performed in order to assess RNFL thickness. The NFL thickness around the optic disc differed statistically among all groups and tended to become thinner as the degree of diabetic retinopathy progressed. The mean, superior and inferior peripapillary NFL thickness differed among groups. As the severity of diabetic retinopathy progressed, the mean, superior, temporal, inferior and nasal macular NFL thickness tended to become thinner. However, only the macular NFL thickness of the superior sector differed significantly among the groups and especially between the control and no diabetic retinopathy groups [22]. In another study using case-control design, 100 type 2 diabetic patients and 50 matched control non-diabetic individuals were compared according to RNFL thickness measured by OCT. In diabetic patients, RNFL thickness was significantly lower than the control group [23].
Chronic hypertension is among the common and most disturbing diseases in pregnancy. Among women in the age group of 18-39 years, hypertension was detected in 7% [4], while the incidence of chronic hypertension co-existing with pregnancy was 1-5% [20,24]. In a study by Gangwani RA et al., in 110 hypertensive patients under anti-hypertensive medications, RNFL thickness was measured by OCT. In higher mean arterial pressure patients, decrease in RNFL thickness was observed [21].
Clinicians commonly face diabetic and sometimes hypertensive pregnant women. Due to the probable progression of diabetic retinopathy in pregnancy, retinal assessment is performed in these patients. A consideration of the increased RNFL thickness in late pregnancy besides the decreased RNFL thickness in diabetes in general, might be helpful in clinical management and decision making for further treatments, such as laser therapy, for this subgroup of pregnant diabetic women. In clinical practice of chronic hypertension and pregnancy, increased RNFL thickness in normal pregnancy in contrast to decreased RNFL thickness due to retinopathy of chronic hypertension should be considered to prevent missing hypertensive retinopathy.
Limitation
The first limitation of the present study was the limited sample population. The second limitation was the lack of control group; although, the study subjects during their second evaluation might be regarded as control group.
Conclusion
The present study revealed an increase in RNFL thickness in late pregnancy, with regression to normal range, 2-8 months after delivery. In common medical diseases during pregnancy, such as diabetes and chronic hypertension with decreased RNFL thickness before pregnancy, these two contra-effects should be considered. More prospective studies should be conducted to investigate final effect of increased RNFL thickness in pregnancy of hypertensive and diabetic women in comparison to normal pregnancy.
Author Contribution
ME, MA, AAB and HG contributed to the conception and design of the study, acquisition of data, analysis and interpretation of results. AAB, HG, BG, SS participated in administrative, technical, and material support. ME and MA supervised the study. All authors participated in the drafting of the manuscript, critical revision of the manuscript for important intellectual content and approved the final manuscript.