Quadricuspid Aortic Valve: A Rare Congenital Anomaly
Kasamshetty Subramanyam1, Vijay Shekar2, Chandrasekaran Dhanalakshmi3, Rangaraj Ramalingam4, Cholenahally Nanjappa Manjunath5
1 Associate Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiology, Bengaluru, Karnataka, India.
2 Postgraduate in DM cardiology, Department of Cardiology, Sri Jayadeva Institute of Cardiology, Bengaluru, Karnataka, India.
3 Echocardiographer, Department of Cardiology, Sri Jayadeva Institute of Cardiology, Bengaluru, Karnataka, India.
4 Professor, Department of Cardiology, Sri Jayadeva Institute of Cardiology, Bengaluru, Karnataka, India.
5 Director, Department of Cardiology, Sri Jayadeva Institute of Cardiology, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kasamshetty Subramanyam, Bannerghatta Main Road, Jayanagara 9th Block, Bengaluru-560069, Karnataka, India.
E-mail: ksubramanyam70@gmail.com
Quadricuspid Aortic Valve (QAV) is a rare, but well-recognised congenital anomaly, which may result in significant aortic regurgitation. We report a case of asymptomatic young male who was inadvertently diagnosed with QAV with moderately severe aortic regurgitation, through Transesophageal Echocardiography (TEE).
Aortic regurgitation, Transesophageal echocardiography, Transthoracic Echocardiography
Case Report
A 38-year-old asymptomatic male patient was found to have a diastolic murmur at the base of the heart on routine clinical examination and later on referred to our institute for further evaluation. There were no significant comorbidities or familial history of cardiac diseases. Upon examination, patient’s blood pressure was 130/84 mmHg and had regular heart beats (76 beats/minute). A diastolic murmur of Grade II intensity was heard at the left second intercostal space. No other additional sounds were present.
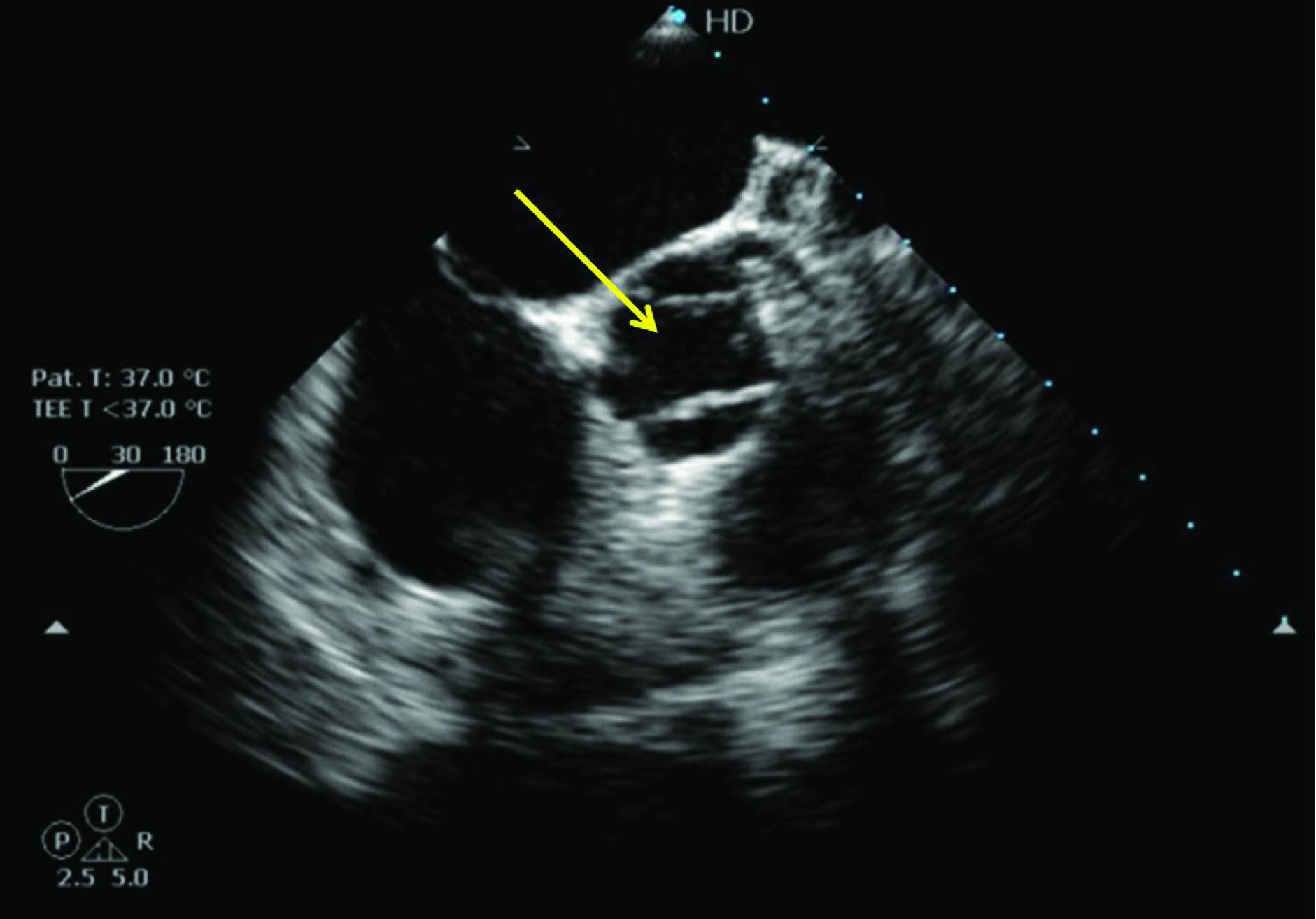
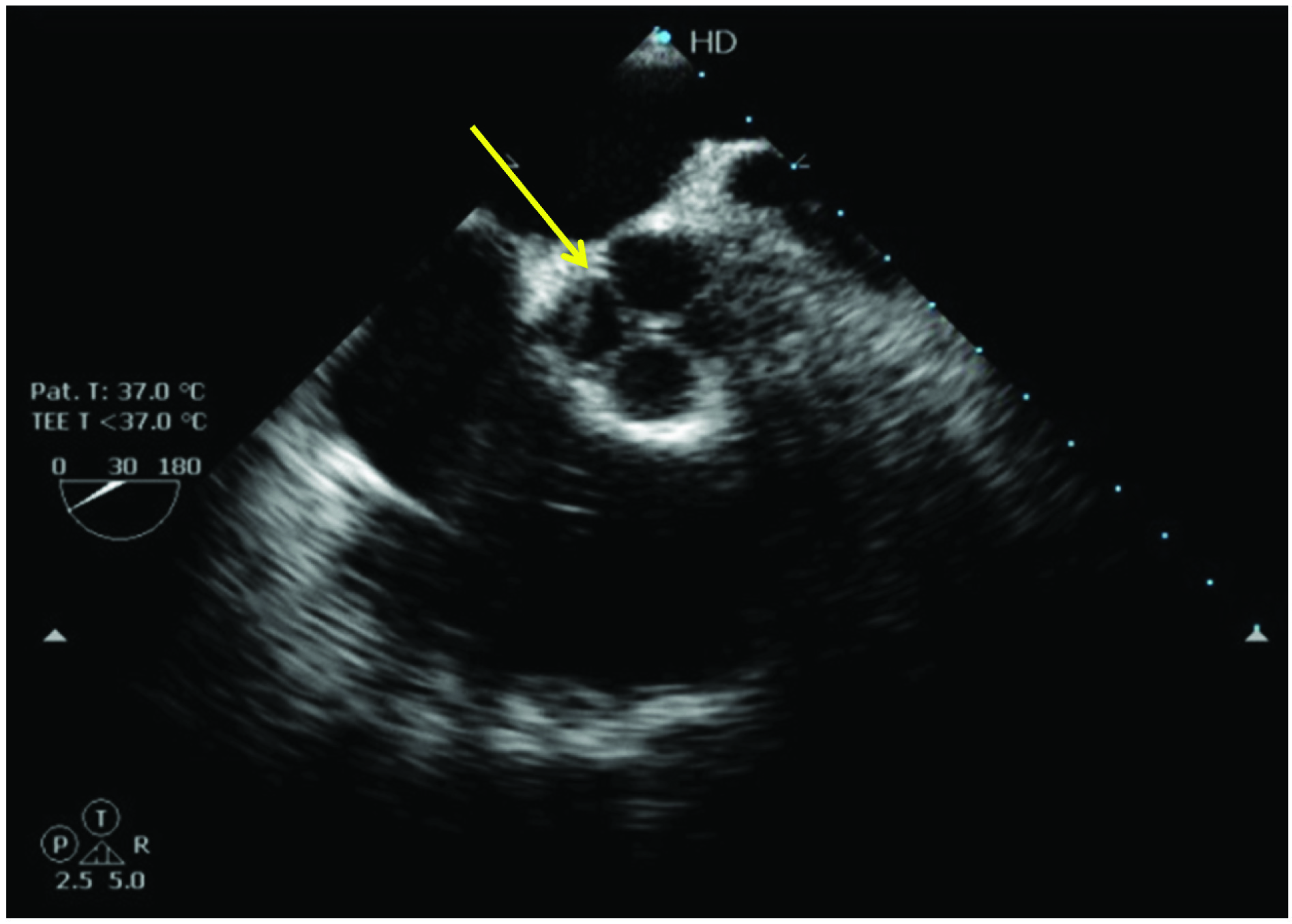
Patient underwent Transthoracic Echocardiography (TTE) which showed normal sized chambers and normal ventricular function. Colour flow imaging across aortic valve revealed moderate aortic regurgitation, which was confirmed by Doppler imaging. Due to poor echo windows, further imaging of the aortic valve and Left Ventricular Outflow Tract (LVOT) could not be obtained satisfactorily. Hence, after obtaining consent, patient was subjected to TEE. Long axis view of the aortic valve [Table/Fig-1] demonstrated moderate aortic regurgitation. There was no evidence of LVOT membrane. Short axis view of the aortic valve [Table/Fig-2,3] showed aortic valve with four cusps and non coaptating leaflets resulting in aortic regurgitation. All four cusps were of equal size. A diagnosis of QAV (Type A) with moderate aortic regurgitation was made. As patient was asymptomatic, he was advised for yearly follow up.
TEE long axis view of aortic valve (122 degrees) showing moderate aortic regurgitation with non coaptating leaflets.

TEE short axis view of aortic valve (30 degrees) showing aortic valve in open position during systole.
TEE short axis view of aortic valve (30 degrees) showing aortic valve in closed position during diastole. The “X” configuration confirms the presence of quadricuspid aortic valve.
Discussion
Quadricuspid aortic valve is a very rare congenital anomaly, unlike unicuspid or bicuspid valve congenital abnormalities, with incidence ranging from 0.008% according to autopsy series and a slightly higher incidence of 0.043% in an echocardiographic series [1,2]. Many a time, it is asymptomatic and may evolve as a progressive aortic insufficiency in the fifth and sixth decades of life. Hence, early diagnosis and regular follow up is essential in patients with such anomaly. Nowadays, the state of art technologies, like TEE, have made it possible to uncover this rare finding [3]. We report one such case of a young male, incidentally diagnosed with QAV through TEE.
The first ever case of this rare malformation was reported in 1862 by Balington J [4]. Since then, there have been more than 200 case reports and literature giving an account of this inherent defect [5]. Although, the exact mechanism underlying this congenital defect has not been completely elucidated, either aberrant fusion of the aorticopulmonary septum or abnormal division of one of the three mesenchymal ridges that give rise to the aortic cusps has been proposed [1,6].
The most usual clinical picture of QAV is dominated by aortic regurgitation, which is reflected in the initial physical examination as a high pitched diastolic murmur along the left lower sternal border [7]. In our study also, an initial examination revealed low grade diastolic murmur, which preliminary indicated the presence of aortic regurgitation. This was further confirmed by colour Doppler imaging, which is considered to be the most sensitive and precise method to diagnose aortic regurgitation, detecting even a mild aortic regurgitation by identifying a turbulent diastolic jet in the outflow tract of the left ventricle [8].
Furthermore, echocardiography is the modality which confirms the presence of QAV and measures the extent of aortic regurgitation. The leading mode of detection is echocardiography being 51.1%, followed by surgery 22.6%, autopsy 15.6% and aortography accounting for another 6.5% [9]. In many cases, TTE is not enough and further TEE is required [10,11]. Even in the current case, TEE was insufficient to establish the finding due to poor acoustic windows. Thus, TEE was performed. It demonstrated the “X” configuration of the cusps in the diastole in contrast to the “Y” configuration of the normal tricuspid valve.
Seven anatomical variants of the QAV have been described by Hurwitz LE and Roberts WC based on the size and equality of cusps [6], A=four equal cusps; B=three equal cusps, one smaller cusp; C=two equal larger cusps, two equal smaller cusps; D=one large, two intermediate, one small cusp; E=three equal cusps, one larger cusp; F=two equal larger cusps, two unequal smaller cusps; G=four unequal cusps. Type A, B and C accounts for more than 85% of cases. In our case, Type A, the second most common type, in which all the cusps are of equal size has been observed.
QAV has also been found to be associated with other anomalies like abnormal origin of coronaries, supravalvular and subvalvular stenosis, non obstructive hypertrophic cardiomyopathy, pulmonary stenosis and ventricular septal defect [12]. However, our patient was diagnosed with isolated congenital quadricuspid valve with mild aortic regurgitation.
Thus, the case emphasises on early diagnosis of QAV through suspicion and further confirmation through advanced techniques like TEE.
Conclusion
Although a rare entity, QAV can result in significant aortic regurgitation requiring aortic valve replacement in the fifth and sixth decade of life. The presence of QAV must be considered in differential diagnosis of patients presenting with isolated aortic regurgitation.
[1]. Simonds J, Congenital malformations of the aortic and pulmonary valvesAm J Med Sci 1923 166(1):584-95.10.1097/00000441-192310000-00013 [Google Scholar] [CrossRef]
[2]. Feldman BJ, Khandheria BK, Warnes CA, Seward JB, Taylor CL, Tajik AJ, Incidence, description and functional assessment of isolated quadricuspid aortic valvesThe American Journal of Cardiology 1990 65(13):937-38.10.1016/0002-9149(90)91446-D [Google Scholar] [CrossRef]
[3]. Bellamkonda S, Pasumarthy A, Velicheti S, Quadricuspid aortic valve diagnosed by multidetector computed tomography (MDCT)BJR| case reports 2015 1(3):2015004010.1259/bjrcr.20150040 [Google Scholar] [CrossRef]
[4]. Balington J, London Medical Gazette July; 1862 [Google Scholar]
[5]. Ginghinã C, Aschie D, Calin A, Popescu B, Calin C, Stoian F, Aortic regurgitation due to quadricuspid aortic valve-case report and literature reviewChirurgia 2012 107:260-64. [Google Scholar]
[6]. Hurwitz LE, Roberts WC, Quadricuspid semilunar valveThe American Journal of Cardiology 1973 31(5):623-26.10.1016/0002-9149(73)90332-9 [Google Scholar] [CrossRef]
[7]. Eugene Braunwald, Braunwald’s heart disease 1997 W. B. Saunders company [Google Scholar]
[8]. Ginghina C, Mic tratat de cardiologieEditura Academiei Române 2010 :843-51. [Google Scholar]
[9]. Armen TA, Vandse R, Bickle K, Nathan N, Three-dimensional echocardiographic evaluation of an incidental quadricuspid aortic valveEuropean Heart Journal-Cardiovascular Imaging 2008 9(2):318-20.10.1016/j.euje.2007.03.04118490326 [Google Scholar] [CrossRef] [PubMed]
[10]. Dencker M, Stagmo M, Quadricuspid aortic valve not discovered by transthoracic echocardiographyCardiovascular Ultrasound 2006 4(1):4110.1186/1476-7120-4-4117087838 [Google Scholar] [CrossRef] [PubMed]
[11]. Shankar B, Mehrotra R, Bansal M, Singh G, Kasliwal RR, Quadricuspid Aortic ValveJ Assoc Physicians India 2012 60:55-5. [Google Scholar]
[12]. Tutarel O, Quadricuspid aortic valves: A reviewClinical Cardiology 2003 26(5):A2410.1002/clc.496026051312769244 [Google Scholar] [CrossRef] [PubMed]