“Teenage” or “Adolescence” is the transition from childhood to adulthood. World Health Organization (WHO) defined teenage pregnancy as period between 10 and 19 years of age. Adolescence represents a key stage in the development and a critical opportunity for ensuring a successful transition to adulthood [1].
Every year about 16 million adolescent girls give birth, among them one million are aged below 15 years. Middle and low income countries are mostly affected. For some adolescents, pregnancy and childbirth are planned and wanted, but for many they are not. Adolescent pregnancies are more prevalent in poor, uneducated and rural communities. By contrast, some girls may face social pressure to marry and, once married, to have children. More than 30% of girls in Low and Middle-Income Countries (LMIC) marry before they are 18; Around 14% of them are aged below 15 [2].
Complications from pregnancy and childbirth are the leading cause of death in girls aged 15-19 years in LMIC where almost all of the estimated three million unsafe abortions occur. Perinatal deaths are significantly higher in babies born to adolescent mothers than in those born to mothers aged 20–29 years, other complications of pregnancy and child birth such as preterm labour, pregnancy-induced hypertension, anaemia and low birth weight babies are strongly associated with adolescent pregnancy [3–5].
India is home to one of the world’s largest youth populations, where 358 million young people (10–24 years) represent 20% of India’s population. One-third of married rural girls are adolescents (10–19 years) and early conception is common [6].
National Family Health Survey (NFHS)-4 revealed that 9.2% teenage pregnancy is prevailing in rural India where as in rural Bengal the scenario is even worse where the prevalence is as high as 20.6% [7,8].
The ASHAs were introduced as integral component of National Rural Health Mission (NRHM) launched in 2005 [9]. They are grass root level workers who are in constant touch with the community. They work as an interface between the community and the public health system. They have a huge role to play if we want to reduce the burden of teenage pregnancy [10]. Their views and suggestions regarding teenage pregnancy will help policy makers to design suitable interventions to overcome the burden of teenage pregnancy. Studies on teenage pregnancy are very few in number [11]. Those which exists are mostly quantitative in nature which at times fails to reveal many facts which are very useful in designing interventions [3,4,12]. Focus group is a form of research where a moderator leads a discussion amongst a group who share a need, lifestyle, or social characteristic, for some specific research aims. It is most commonly used for social or market research and is often viewed as more cost-effective than qualitative interviewing or ethnography [13]. With this background, the present Focussed group discussion was conducted among selected ASHAs of Singur block to understand the perception of ASHAs regarding teenage pregnancy and its preventive measures.
Materials and Methods
The present study was a qualitative study/Focussed Group Discussion (FGD) conducted on 30th March 2017 among ASHAs of Singur block which is rural field practice area of All India Institute of Hygiene and Public Health (AIIH and PH), Kolkata West Bengal. There is total 64 villages with 64 ASHAs. Inclusion criteria were experience of atleast one year as ASHA and giving consent for participation.
All the ASHAs were found to be meeting our study selection criteria, 12 of them were selected by convenience sampling and were sent invitations to participate in the study. Ten accepted our invitation and participated in our study.
Before the session ASHAs were informed about their autonomy, confidentiality and right to leave the study at any given point of time. Informed written consent of all the participants were taken before taking part in the study. Permission from the local health authorities and the Institute Ethics Committee was taken to perform the research work.
The instructions to the participants before commencing FGD were as below:
Please talk one at a time and speak up as much as possible. There is nothing such as right or wrong answers of our questions and this is not an evaluation process.
The FGD was conducted under following themes:
Theme 1: Knowledge of teenage pregnancy, legal age of marriage and pregnancy, Theme 2: Burden of teenage pregnancy, Theme 3: Reasons behind teenage pregnancy, Theme 4: Harmful effects of teenage pregnancy, Theme 5: Role of health workers in reducing burden of teenage pregnancy, Theme 6: Role of government in reducing burden of teenage pregnancy and Theme 7: Suggestions for reducing burden of teenage pregnancy. Themes were selected by extensive review of literature and finalised by the experts of Department of community medicine and Department of health education of AIIH and PH.
Theme 1: Knowledge of Teenage Pregnancy, Legal Age of Marriage and Pregnancy
Questions asked:
What do you mean by teenage?
When a pregnancy is called a teenage pregnancy?
What is legal age of marriage for a girl?
Theme 2: Burden of Teenage Pregnancy
Questions asked:
How many of you have seen teenage pregnancy in your area?
If yes, Is it a common finding?
Theme 3: Reasons Behind Teenage Pregnancy
Questions asked:
What do you think about the reasons behind this increasing trend of teenage pregnancies?
Is lack of education a cause?
Is it due to culture?
Is poverty a cause?
Is gender bias a cause?
Theme 4: Harmful Effects of Teenage Pregnancy
Questions asked:
Do you think teenage pregnancy is harmful for the mother/child?
If yes, what are the hazards of teenage pregnancy?
Theme 5: Role of Health Workers in Reducing Burden of Teenage Pregnancy
Questions asked:
Do you (health care provider) have any role in reducing the burden of teenage pregnancy?
If yes, How?
Does increase in awareness regarding family planning services help to reduce teenage pregnancy?
Theme 6: Role of Government in Reducing Burden of Teenage Pregnancy
Does current government schemes like beti bachao beti padhao is helping in reducing teenage pregnancy? (sufficiency of schemes).
Theme 7: Suggestions for Reducing Burden of Teenage Pregnancy
According to you, what to be done to reduce burden of teenage pregnancy?
All questions asked were open ended. The Focussed group discussion was held in the conference cum meeting room of Rural Heath Unit and Training Centre (RHUTC), Singur.
A meeting was held among the moderator, other experts in community medicine and health education to prepare the focus group guide. A set induction involved greetings, ice breaking, and was followed by the discussion proper.
The FGD was conducted in the local language of Bengali which is spoken and well understood by all study participants. Questions were asked to the group and each participant was given an opportunity to respond. The researchers played the role of moderator and note takers role in focus group discussion. Simple language with short well-constructed and understandable questions was used in the discussion. All nonverbal communication such as laughter, disagreements by shaking head was also documented. Questions were asked until there was no new information that was generated from the study participants. At the end of FGD, study participants were given an opportunity to ask questions related to the discussion. The group discussion lasted for 55 to 60 minutes. Semicircular sitting arrangement was planned to ensure there was a good communication between the study participants and interviewers.
Two separate note-takers were involved in the process of note-taking. To increase the reliability of data, standard norms for note taking were followed.
During the session, validity was ascertained using the following methods:
All persons involved in conducting the session of FGD except the moderator refrained from talking. The note-takers produced notes as exact as possible
Analysis was done thematically as per [Table/Fig-1]. To improve the credibility of the results, meeting with the note-takers, and two independent expert observers were held separately.
Flowchart showing steps of thematic analysis for the study.
Peer debriefing with was performed to ensure disclosure of blind spots and compare the working hypothesis and results.
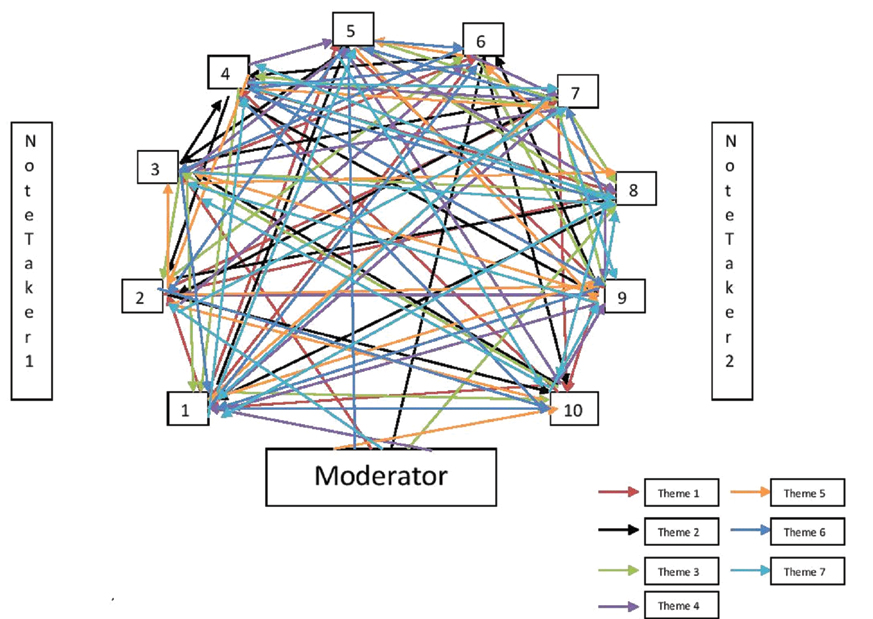
A sociogram was used to keep a record of conversation and participation [Table/Fig-2].
Sociogram show pattern of participation of the study participation (n=10).
Results
The age of the recruited participants varied from 30 to 45 years. Most of them have five years experience. While one had completed secondary level of education, and another higher secondary level of education, the others completed graduate or postgraduate level of education [Table/Fig-3].
Background characteristics of the study participants (n=10).
| Participant | Age/Gender | Educational level | Years of experience |
|---|
| P-1 | 38/F | Graduate | 5 |
| P-2 | 30/F | Postgraduate | 3 |
| P-3 | 39/F | Graduate | 5 |
| P-4 | 42/F | Secondary | 5 |
| P-5 | 45/F | Graduate | 5 |
| P-6 | 44/F | Graduate | 7 |
| P-7 | 38/F | Graduate | 5 |
| P-8 | 38/F | Postgraduate | 5 |
| P-9 | 41/F | Graduate | 8 |
| P-10 | 45/F | Higher secondary | 5 |
Theme 1: knowledge of Teenage Pregnancy, Legal Age of Marriage and Pregnancy
Meaning of teenage pregnancy: Most of them said that it is pregnancy before 19 years of age. P-7 stated that “pregnancy after 10 years and before 19 years is called teenage pregnancy”. Some of them said it is pregnancy in 14-19 years in married/unmarried woman.
Legal age of marriage: Most of them said that it is after completion of 18 years.
Age of pregnancy: There were different views regarding age at pregnancy as some of them said 19 as minimum age of pregnancy and some suggested 20-21 as minimum age of pregnancy. P-3 suggested that “even if a girl get married before 18 years she should made aware about not to take pregnancy before 18 years”.
Theme 2: Burden of Teenage Pregnancy
All of them had seen teenage pregnancy in their area of service.
Incidence in their respective service areas: Most of them said that though teenage pregnancy is still prevalent in their community but the incidence is much reduced from past. P-9 said that “...There were no teenage pregnancies in my area in past one year...” P-4 reported “...There are many teenage pregnancies in Daipukur area where Scheduled Caste (SC)/Scheduled Tribe (ST) population is more prevalent…” Most of them had seen two to three teenage pregnancy in their respective area in past one year. P-1 had seen two teenage pregnancy last year of which one resulted in spontaneous abortion.
Theme 3: Reasons Behind Teenage Pregnancy
Lack of awareness: Most of them highlighted lack of awareness is the predominant cause of teenage pregnancy. According to them, the villagers were not at all aware of the fact that teenage pregnancy is dangerous for the health of the mother and her child too. Many of them were told by the teenage mothers that “when they are married it means that they are ready for the child bearing.”
Lack of family planning knowledge: Some of them also highlighted the fact that lack of knowledge regarding family planning practices may be one of the predominant cause of teenage pregnancy. P-1 reported while promoting family planning they come across comments like “we are careful we do not need any family planning”. P-7 told “...... though early marriage happens, if they use family planning methods properly, they do not have to face catastrophe of teenage pregnancy......”
Lack of education: Furthermore, they said lack of education is the major contributor in lack of awareness while some identified lack of education as predominant cause. According to them, lack of education is the foundation block of the vicious cycle which ultimately leads into an underage marriage and teenage pregnancy.
Caste: P-4 said that it is more in SC/ST prevalent areas and less in areas of other castes. P-8 accepted that in spite of their regular house to house visits to promote family planning they failed to motivate teenagers to use family planning especially to the families of SC/ST. P-3 said other caste people even if get married early takes pregnancy in later age contrary to that SC/ST people get married and pregnant early.
Gender discrimination: Some of them said that it is men driven society where a girls opinion and choice regarding family planning practices hardly matters. P-8 said “......if women are not being empowered and cannot find herself in a position to take her decision alone and for her well-being, it is not possible to eradicate problems like teenage pregnancy, because though its major bearing on health, it is more of a social problem rather than a medical one..........”
Pressure from in-laws: According to two of them (P-3, P-7), sometimes there in-laws force them to take early pregnancy as they are desirous of grandchild. P-3 given an example by saying “……..I know a teenage girl who used to take condom from me but when her in-laws came to know about it they were angry like anything, (laughing). After that she stopped taking condoms from me…..”.
Financial insecurity: Most of them said that financial and social insecurity forces a father to get her daughter married early. Chance of a good relationship (nice groom) is another factor which entices father to get her daughter married early. P-6 criticised this as “.......By giving early marriage, a father is promoting his daughter to be raped.....”
Rape: P-9 highlighted increasing incidences of rape are foremost cause of teenage pregnancy.
Theme 4: Harmful Effects of Teenage Pregnancies
All agrees to the fact that it is harmful for both mother and child. Some said that it may result into death of mother and the child. Some said that it may result into abortion. Some of them said that teenage pregnancy may result into underweight child. P-2, P-4, P-7 and P-8 said “...... it may cause anaemia, haemorrhage [APH (Ante-Partum Haemorrhage)/PPH (Post-Partum Haemorrhage)] and even miscarriage of the mother.....” One of them said that it may damage mother’s liver and kidney.
Theme 5: Role of Health Workers in Reducing Burden of Teenage Pregnancy
All of them agree that that they have a substantial role in reducing teenage pregnancy. They told that they may aware people regarding family planning services to avoid teenage pregnancy. Some of them said that they may conduct monthly meetings at village level with eligible couples in order to counsel those regarding ill effects of teenage pregnancy and improving their knowledge regarding various family planning practices. P-10 opined “...........we may try to counsel the parents of girl child about the ill effects of teenage pregnancy to convince them not to get their daughter married before 18 years.....”. They told that there is lack of manpower to generate awareness. They need support of panchayets and government to conduct various awareness generation activities such as rallies against teenage pregnancy.
Theme 6: Role of Current Government in Reducing Burden of Teenage Pregnancies
All of them agreed that current government initiatives are certainly helping in reducing teenage pregnancy but there is need of increase in awareness regarding these initiatives.
Theme 7: Suggestions for Reducing Burden of Teenage Pregnancy
Provision of more stringent law: Some of them said that registry marriage should be made compulsory to reduce teenage marriage which is one of the predominant causes of teenage pregnancy and P-3 told “....... those who found to be culprit of teenage marriage should be sent to jail......”
Increase manpower for awareness generation: Most of them said that government should deploy more health workers in order to generate awareness regarding ill effects of teenage pregnancy.
Strengthening of existing programmes: Some said government should do more publicity of schemes like “Beti Bachao Beti Padhao”, “SABALA”, “Kanyashree Prakalpa” etc. To encourage woman empowerment and discourage teenage pregnancy.
IEC for awareness generation: Government should organise rallies to increase awareness regarding teenage pregnancy and its ill effects. Meetings should be organised at gram panchayat level with the parents and teenagers. P-1 said “.......TV advertisements discouraging teenage pregnancy should be done as it is ongoing for “swachh Bharat Mission” by some actor or actress.....”
Provision of sex education at school curriculum: According to most of them, proper sex education should be introduce into the school curriculum to educate the teenagers about the ill effects of teenage pregnancy and importance of family planning methods to avoid it.
The sociogram showed that all the participants participated in an equal manner and this was an even discussion [Table/Fig-2]. The summary of the findings are depicted in [Table/Fig-4].
Highlights of the findings of the study according to the themes (n=10).
| Themes | Highlights of findings |
|---|
| Theme 1 | Pregnancy <19 years in married/unmarried women. Some said pregnancy at 19 years, Some said pregnancy at 20-21 years. |
| Theme 2 | In some area none in past one year.In some area 2-3 in past one year.More in SC/ST area. |
| Theme 3 | Lack of awareness, lack of family planning knowledge, lack of education, caste, gender discrimination, pressure from in-laws, financial insecurity, rape. |
| Theme 4 | Death of mother and the child, malnourished child, anaemia of mother, APH, PPH, abortion. |
| Theme 5 | Generate awareness in community regarding harmful effects of teenage pregnancy and family planning services.Monthly meeting of eligible couple.Organising rallies against teenage pregnancy.Counselling of parents of girl child. |
| Theme 6 | Certainly helping in reducing teenage pregnancy but there is need of increase in awareness regarding these initiatives. |
| Theme 7 | Provision of more stringent law.Increase manpower for awareness generation.Strengthening of existing programmes.IEC for awareness generation.Provision of sex education in school curriculum. |
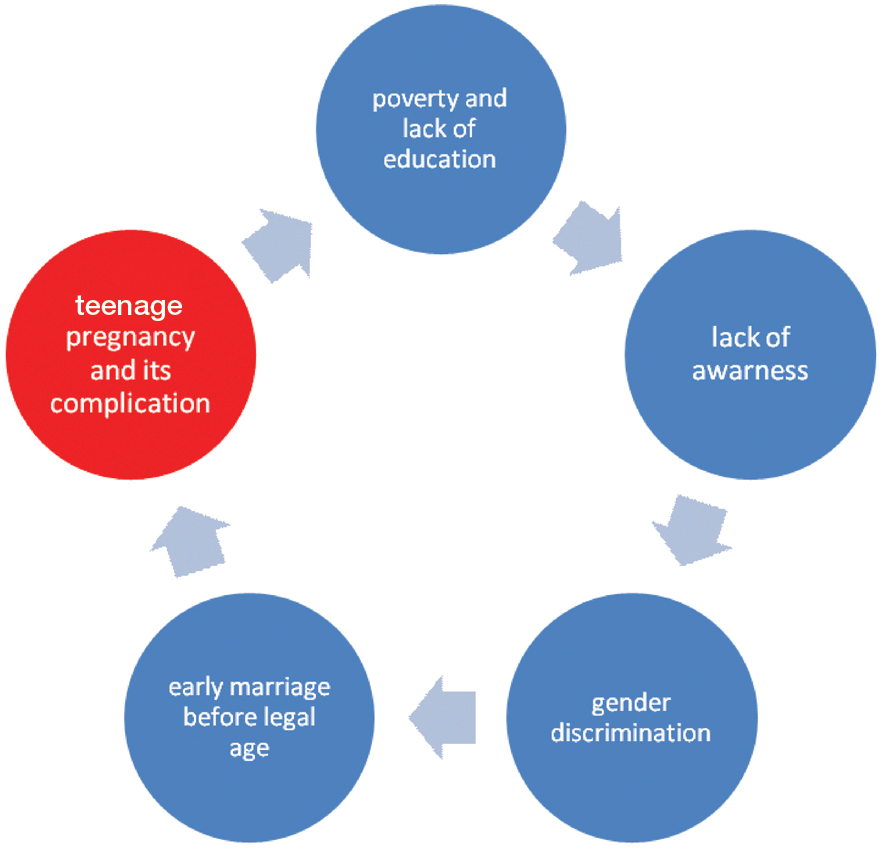
[Table/Fig-5] depicts vicious cycle of reasons behind teenage pregnancy as per current study findings.
Flowchart depicting vicious cycle of reasons behind teenage pregnancy as per current study findings (n=10).
Discussion
Present FGD was carried in a rural block of West Bengal among ASHAs to know their views, experiences and perspectives regarding teenage pregnancy.
Theme 1 and 4
Most of the ASHAs were aware regarding meaning of teenage pregnancy and correct age of marriage. Overall knowledge of ASHAs regarding teenage pregnancy though found to be satisfactory had certain lacunae which need to be addressed. As they are ground level health workers, proper knowledge of teenage pregnancy will enable them counsel eligible couples and pregnant women regarding its ill effects. It will also help them identify complications of pregnancy at early stage and refer the mother to the relevant management.
Theme 2 and 3
Most of the study participants reported that incidence of teenage pregnancy declined compared to past which was a positive finding but they also opined that there are certain pockets in the community where it is still prevalent which is worrisome. As per the ASHAs reasons behind prevailing teenage pregnancies in the community were as following.
Lack of awareness: Lack of awareness regarding family planning services and ill effects of teenage pregnancy was found out to be a predominant cause of teenage pregnancy. The study conducted by Boustani MM et al., [14] had findings concurrent to ours.
Lack of family planning knowledge: Some of the ASHAs reported during promotion of family planning they come across resistance. People used to report that they are careful and don’t need family planning. There is a myth that by using traditional contraceptive methods like “coitus interruptus”, ”periodic abstinence” etc. one is safe from getting pregnant but the truth is even with correct use, periodic abstinence has three times higher odds of resulting in unintended pregnancies compared with modern contraception which indirectly adds on to the burden of teenage pregnancy [15].
Lack of education: Education enables a person to take right decision at right time. In rural settings, lack of education is a predominant cause of teenage pregnancy. Similar findings were observed in our study. Dutta I et al., [12] reported higher proportion of primi teenage mothers (53.5%) had not even gone to school compared to adult primi (8.1%). Yasmin G et al., [16] and Gyesaw NYK et al., [17] had similar findings.
Caste: ASHAs reported that SC/STs marry early and are reluctant to use family planning services. The studies conducted by Dubey R et al., [18] and Sah RB et al., [19] supports our findings. It may be due to traditional beliefs regarding preserving a girl’s chastity and family needs to reduce expenditure.
Financial insecurity: Poverty evolved as an important factor responsible for teenage pregnancy. India is a country where a substantiate proportion of population is still living below poverty line [20]. Poverty has direct influence on education, awareness, health seeking behaviour etc. A socioeconomically poor father accounts a girl child as burden. He tries to get her daughter married as soon as he gets a plausible chance. In this study, ASHAs reported the same. The study conducted by Pati RN et al., [21] had similar findings.
Gender discrimination and pressure of in-laws: Gender discrimination emerged as an important factor responsible for teenage pregnancy. There is a very little role of an adolescent girl in decision making process such as marriage, contraceptive use, pregnancy etc. which makes them vulnerable to conceive early. Early marriage and pregnancy robs an adolescent girl’s opportunity for education. The findings of the study were in concordance to Paul M et al., [22] and Dubey R et al., [18].
Rape: Rape is another factor where teenage girl is exposed to many physical, mental and social sufferings. Rape resulting in pregnancy is more common in adolescents compared to adults. The study conducted by Suthapom S et al., [23] reported that Adolescent victims had a higher pregnancy rate than adult victims (9.0% vs. 3.6%).
Theme 5
ASHAs suggested that improving awareness of family planning services will help to reduce teenage pregnancy. They suggested that monthly meeting of eligible couple, organising rallies against teenage pregnancy, counselling of parents of girl child will help to reduce burden of teenage pregnancy. A systematic review on this regard conducted by Salam RA et al., [24] reported similar findings and suggested that sexual and reproductive health education, counselling, and contraceptive provision are effective in increasing sexual knowledge, contraceptive use, and decreasing adolescent pregnancy.
Theme 6
The study revealed that certain government schemes like “Beti Bachao Beti Padhao”, “SABALA”and “Kanyashree Prakalpya” are helping in counteract the problems of early marriage and teenage pregnancy (as per ASHAs). These schemes are mainly targeted towards adolescent girls. Under the schemes, adolescent girls are given monitory incentives to continue their education. It is envisaged that they will use the opportunity to gain skills and knowledge that will help them to become economically independent [25,26]. However, there was need of popularisation of these schemes.
Theme 7
ASHAs also reported that there is huge scarcity of manpower at grass root level and suggested government to deploy more manpower in this regard. In India there are always financial constrains so deploying more manpower may not be a feasible option every time. The solution may be by peer monitoring suggested by Mezey G et al., [27]. The study reported that peer educator may act as an mentor and may help in support and guidance of an adolescence. Recently such initiatives are also taken by Government of India [28].
Limitation
Only one FGD was conducted which may not reflect views and perceptions of ASHAs working in the whole block. So, generalizability of the study is limited.
Conclusion
The study revealed that burden of teenage pregnancy is though low but still exists. To empower ASHAs, regular training sessions regarding pregnancy and its complications should be conducted. In the current study, ASHAs highlighted their experiences, purviews and gave some useful suggestions which will help policy makers to design suitable interventions to counsel and educate people regarding ill effects of teenage pregnancy to reduce its burden. Popularisation of government financial schemes to demotivate teenage marriage and pregnancy is also warranted in this regard.