Improved Outcome with Gefitinib in Recurrent Middle Ear Squamous Cell Carcinoma
Satyajeet Rath1, Madhup Rastogi2, Ajeet Kumar Gandhi3, Paritosh Pandey4, Sambit Swarup Nanda5
1 Senior Resident, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
2 Professor and Head, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
3 Assistant Professor, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
4 Consultant, Department of ENT, Lucknow Cancer Institute, Lucknow, Uttar Pradesh, India.
5 Senior Resident, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Madhup Rastogi, Professor and Head, Department of Radiation Oncology, Dr. Ram Manohar Lohia Institute of Medical Sciences, Vibhuti Khand, Lucknow-226010, Uttar Pradesh, India.
E-mail: drmadhup1@gmail.com
Middle ear and external ear malignancies are rare. There is lack of consensus in managing such cases. Surgery followed by radiotherapy is the best option for advanced cancers, while radiotherapy alone in radical doses is sufficient for early disease. There is also dearth of literature in management of recurrence or metastasis. We present the case of a 25-year-old boy who had recurrence following surgery and radiotherapy for middle ear Squamous Cell Carcinoma (SCC). He was started on gefitinib and showed remarkable improvement in symptoms within two months of the treatment.
Malignancy of ear, Radiotherapy, Recurrence
Case Report
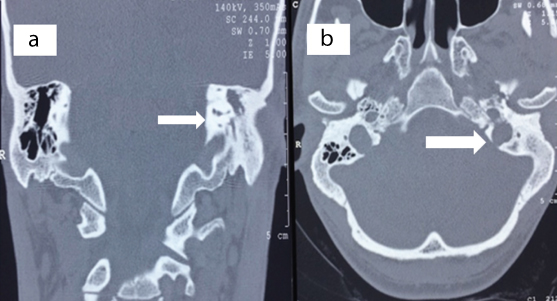
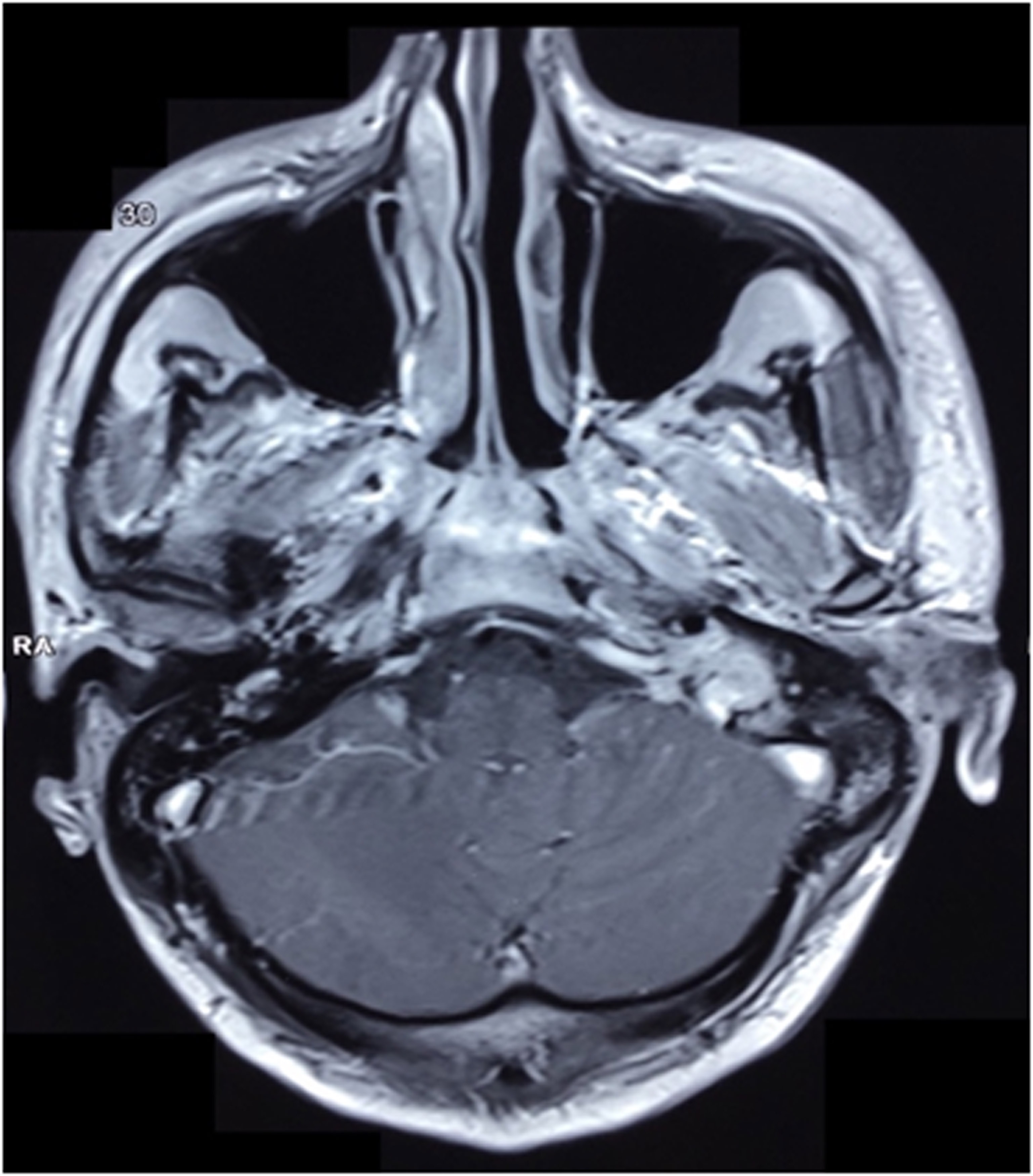
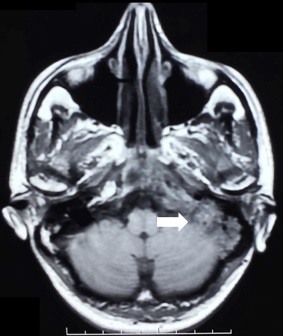
A 25-year-old male presented with discharge from left ear for around 20 years, facial weakness for six months and pain in left ear since three months. A thorough Ear, Nose, Throat (ENT) evaluation revealed chronic otitis media left side with aural mass and grade V facial nerve palsy. A Contrast Enhanced Computed Tomography (CECT) of temporal bone revealed left chronic tympanomastoiditis associated with cholesteatoma formation [Table/Fig-1a,b]. There was a mildly enhancing soft tissue component in the left external and middle ear cavity with partial erosion of middle ear ossicles and bony canal of the facial nerve. Partial erosion of jugular fossa, anterior wall and tegmen tympani was also there, although, no evidence of intracranial extension of the lesion was found. A magnetic resonance imaging (MRI) of brain [Table/Fig-2] confirmed the same. It was followed by treatment with left modified radical mastoidectomy with facial decompression and excision of tumour from middle ear, attic and anterior epitympanum with meatoplasty.
CT Coronal and axial view showing cholesteatoma with tympano-mastoiditis.
MRI Brain showing lesion in the middle ear with surrounding erosion.
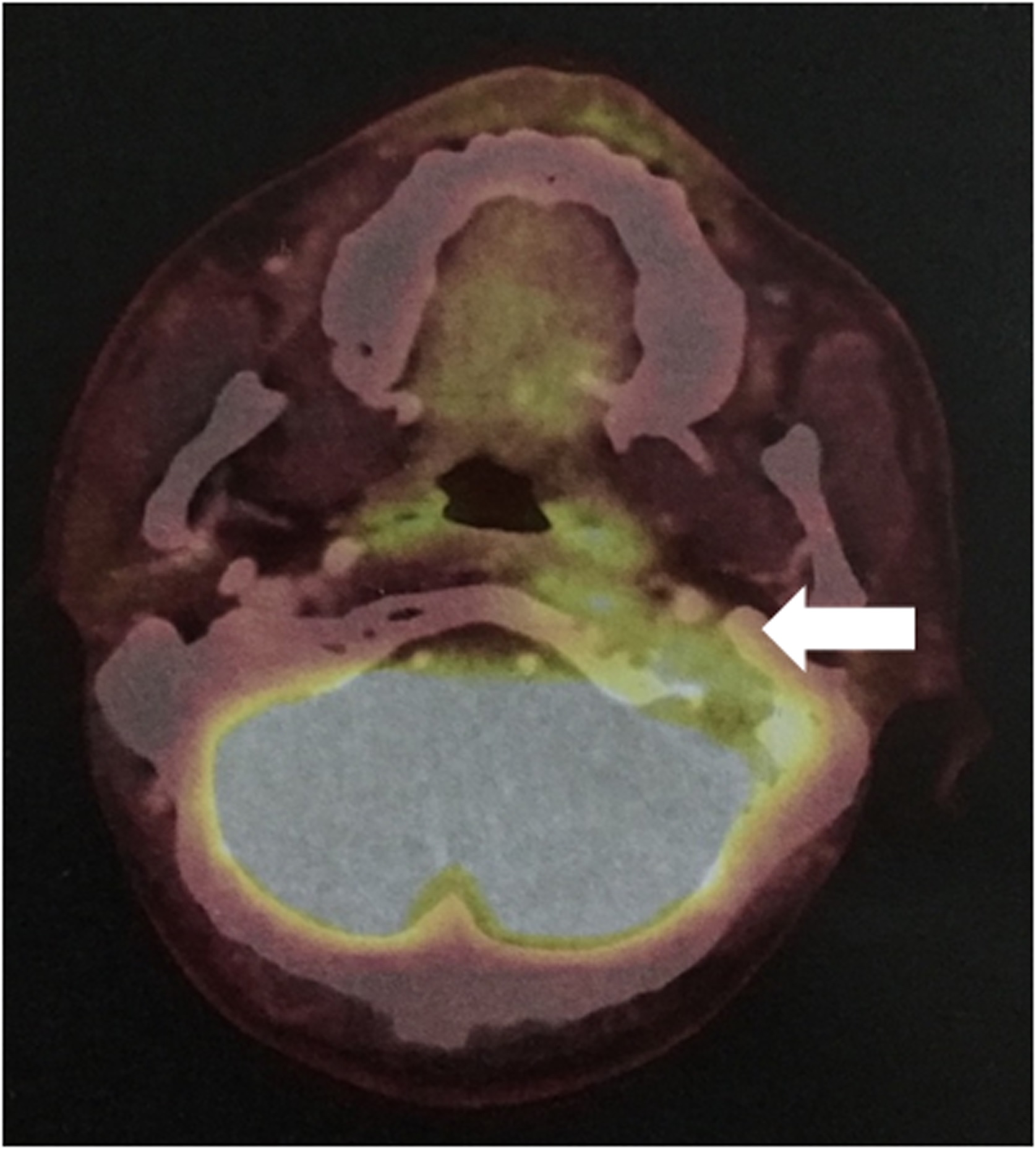
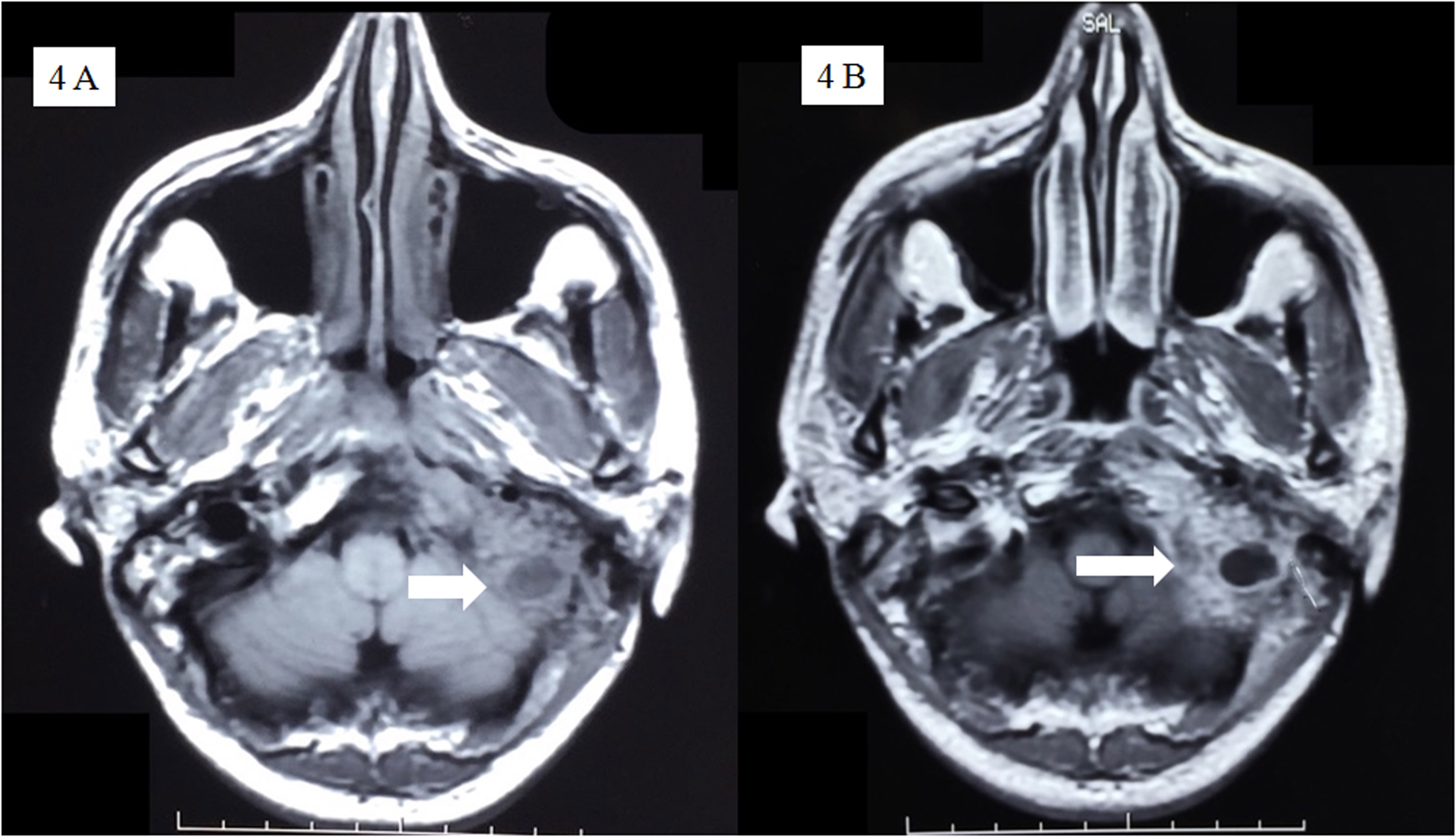
The Histopathology (HPE) showed a moderately differentiated SCC. The patient had symptoms of nasal intonation, difficulty in swallowing with voice and cough after one month of the surgery. On evaluation, patient had left side facial nerve palsy with hoarseness of voice. MRI Brain showed enhancing soft tissue lesion involving left facial canal, jugular fossa and carotid sheath with left parapharyngeal wall thickening. Considering the lesions as residual disease, he was given two cycles of chemotherapy elsewhere and was referred to us. He received radiotherapy 66 Gy in 33 fractions along with one cycle concurrent cisplatin 50 mg. Patient was clinically normal on follow up for one year and a Positron Emission Tomography (PET) scan also confirmed the same. Patient again had complaint of pain in left temporal area and in left ear one year after completing the treatment. After discussion in tumour board, a repeat PET scan was done [Table/Fig-3]. It showed avid (SUVmax: 8.95) lytic destructive lesions with soft tissue component involving petrous and mastoid part of left temporal bone, occipital and sphenoid bones [Table/Fig-4]. It was also involving left jugular foramen with an extracranial soft tissue component. MRI brain [Table/Fig-4a,b] showed heterogeneously enhancing mixed intensity solid-cystic lesion with erosion of clivus, left half of occipital bone and anterior arch of atlas on left side with infiltration into adjacent sigmoid sinus and left internal jugular vein. The mass was also encasing internal carotid artery in carotid canal and eroding the left semicircular canal. Surgical opinion was taken but surgery was denied. Since, the option of radiotherapy had already been exhausted, he was started on oral gefitinib 250 mg. The symptoms improved after administration of two months of gefitinib. A MRI [Table/Fig-5] repeated after that showed smaller lesions. Subsequently, he was put on methotrexate and gefitinib combination, and is clinically normal after six months of follow-up.
PET Scan showing increased uptake in petrous and mastoid part of left temporal bone.
MRI T1 plain and contrast images showing solid-cystic lesion eroding the left semi-circular canal.
MRI T1 image showing decreased size of lesion as compared to the previous imaging.
Discussion
Squamous cell carcinoma of the middle ear and external auditory canal is very rare, with a reported prevalence of one in ten lakh persons [1]. These tumours are generally associated with symptoms of ear pain and discharge, bleeding and hearing loss and hence, diagnosis is delayed as it is often confused with other common benign diseases with similar presentation [2]. The temporal bone, ear canal and middle ear are rare sites of malignancy and their anatomical location and invasive nature pose a challenge for treating physicians.
Optimum treatment guidelines have been difficult to formulate because of the rarity of occurrence of the tumours and lack of uniform staging system [3]. Staging system for middle ear carcinomas was proposed by Arriaga M et al., based on clinical and radiological findings [4]. The five year actuarial rates as mentioned by Arriaga [4] ranged from 83% for T1 lesions to 27% for T4 lesions. Several single institutional studies have reported prognostic factors and treatment option in these tumours and optimal role of surgery, chemotherapy and radiotherapy (RT) remains controversial. One study by Ogawa K et al., [5]. revealed that treatment with surgery plus RT was associated with better local control and overall survival. Similar results were also shown by Pemberton LS et al., [6]. and Yin M et al., [7]. While some authors suggest RT for recurrent cases, doubtful free margins and/or presence of lymph node invasion [8], other investigators recommend surgery followed by RT as the standard of care in general for all advanced disease (T2-3) [5]. Another study by Moffat DA et al., concluded that radical RT doses of at least 70 Gy may be necessary for local control in case of advanced disease [9]. The role of technique of delivery of RT has also evolved over the years and has increased importance in the management of middle ear carcinomas with RT being the choice for definitive therapy for early stage cancers. However, there are no defined treatment guidelines for recurrent SCC of middle and external ear. A wide variety of treatment options has been tried for head and neck squamous cell cancers, which include palliative RT and chemotherapeutic agents. The most important decision being the choice of agents to be used depends on the condition of the patient and the form of palliation intended by the physician. The agents include methotrexate, platins, taxanes, gefitinib, cetuximab and combination of these agents. Gefitinib has previously been addressed by authors for recurrent head and neck SCC. It has been used as a metronomic therapy as a single agent or in combination with methotrexate and/or celecoxib with good results [10]. The results of these can be extrapolated to recurrent and middle ear carcinomas as they share the same histology as other SCC of head and neck.
Conclusion
In conclusion, in this report, we describe a case of a rare tumor type with recurrence for which the most beneficial therapeutic approach was unsure. Gefitinib resulted in an unusually better response compared to other expected treatment modalities for palliation. Like in other SCC, gefitinib also can give good results in recurrent SCC. It should be considered as a viable treatment option in recurrent middle ear and external ear carcinomas.
[1]. Lobo D, Llorente JL, Suarez C, Squamous cell carcinoma of the external auditory canalSkull Base 2008 18(3):167-72. [Google Scholar]
[2]. Lim L H, Goh Y H, Chan Y M, Chong VF, Low WK, Malignancy of the temporal bone and external auditory canalOtolaryngol Head Neck Surg 2000 122(6):882-86. [Google Scholar]
[3]. Nakagawa T, Kumamoto Y, Natori Y, Shiratsuchi H, Toh S, Kakazu Y, Squamous cell carcinoma of the external auditory canal and middle ear: An operation combined with preoperative chemoradiotherapy and a free surgical marginOtol Neurotol 2006 27:242-48. [Google Scholar]
[4]. Arriaga M, Curtin H, Takahashi H, Hirsch BE, Kamerer DB, Staging proposal for external auditory meatus carcinoma based on preoperative clinical examination and computed tomography findingsAnn Otol Rhinol Laryngol 1990 99:714-21. [Google Scholar]
[5]. Ogawa K, Nakamura K, Hatano K, Uno T, Fuwa N, Treatment and prognosis of squamous cell carcinoma of the external auditory canal and middle ear: a multi-institutional retrospective review of 87 patientsInt J Radiat Oncol Biol Phys 2007 68(5):1326-34. [Google Scholar]
[6]. Pemberton LS, Swindell R, Sykes AJ, Primary radical radiotherapy for squamous cell carcinoma of the middle ear and external auditory canal—an historical seriesClin Oncol (R Coll Radiol) 2006 18(5):390-94. [Google Scholar]
[7]. Yin M, Ishikawa K, Honda K, Arakawa T, Harabuchi Y, Nagabashi T, Analysis of 95 cases of squamous cell carcinoma of the external and middle earAuris Nasus Larynx 2006 33(3):251-57. [Google Scholar]
[8]. Kollert M, Draf W, Minovi A, Hofmann E, Bockmühl U, [Carcinoma of the external auditory canal and middle ear: therapeutic strategy and follow up]Laryngorhinootologie 2004 83(12):818-23. [Google Scholar]
[9]. Moffat DA, Wagstaff SA, Squamous cell carcinoma of the temporal boneCurr Opin Otolaryngol Head Neck Surg 2003 11(2):107-11. [Google Scholar]
[10]. Colevas AD, Chemotherapy options for patients with metastatic or recurrent squamous cell carcinoma of the head and neckJ Clin Oncol 2006 24(17):2644-52. [Google Scholar]