Asthma is a chronic airway disease affecting approximately 235 million people worldwide [1]. Inhaled medication in asthma has revolutionized the treatment with better outcomes and lesser side effects. Despite tremendous progress in the field, adequate control of asthma is still a major challenge faced by physicians worldwide. Among all risk factors, suboptimal adherence to the inhaled controller medication is an important reason for poor asthma control [2].
From asthma perspective, adherence is the degree to which patients takes their inhalers as prescribed by their health care providers. Unfortunately, research on adherence to controller medication has demonstrated a wide range of non-adherence ranging from 9-80% across varied settings [3-6]. A wide variety of different patients, disease and therapy related factors have been identified as determinants of medication non-adherence in asthma [7,8]. However, due to lack of uniformity in the study design and/or adherence measuring methods, there is a wide variation in the results among different studies.
Poor adherence with the prescribed therapy leads to increased morbidity and health expenditure in asthma [9]. As per INSEARCH study, estimated prevalence of asthma in India accounts to be 2.05% among those aged >15 years, with an estimated national burden of 18 million asthmatics [10]. Despite a heavy burden of disease, adherence to treatment has been rarely evaluated in Indian patients [11-13]. Moreover, these available studies have utilized subjective adherence measurement which is accompanied by inherent flaws. A good number of studies on this topic have been conducted outside India but, due to differences in culture and lifestyle as well as healthcare practices, the results may not be applicable to Indian patients. Hence, the study was planned to synthesize the current observational data on the prevalence of adherence to ICS and its determinants in patients of bronchial asthma using an objective adherence measurement tool.
Materials and Methods
This was a prospective observational study conducted at the Department of Pulmonary medicine, Government Medical College and Hospital (GMCH), Chandigarh over a period of one year (Febuary 2016 to January 2017). One hundred and three patients with physician diagnosed bronchial asthma, in their stable phase and on regular controllers medicines (ICS with/without long acting beta agonists) for more than six months were enrolled. Sample size was calculated on the basis of a prevalence of 70% adherence to ICS as per previous studies [4,14], assuring 90% confidence interval at 5% level of significance and 80% power. After adjusting for 20% non-response rate, a sample size of 100 patients was decided. Patients with acute exacerbation of asthma or other pulmonary comorbidities like pneumonia, lower respiratory tract infections etc in the preceding six weeks, uncontrolled cardiac comorbidities like unstable angina, recent myocardial infarction (in last six weeks) were excluded from the study. The study was approved by the Institutional Ethics Committee of GMCH.
After obtaining written informed consent, necessary information on patient demographics and medical history, particularly the type and duration of symptoms, occupational history, and their literacy status was retrieved from the patients as well as by scrutinizing the records. Patients were said to be literate if they had done their primary level of education or above. Asthma symptom control level was assessed by recording self-reported asthma attacks and/or emergency visits in the preceding one year. Asthma was said to be controlled if there were no attacks or emergency visits [15]. Information on the total duration of inhaler use, type of inhaler was collected and correctness of inhaler technique checked. Asthma knowledge on medical adherence was checked from the patients by a single question, asking whether they were given information on adherence education by their treating physician. The information generated was recorded in a dichotomous (yes/no) way. All patients underwent routine spirometry as per therecent American Thoracic Society (ATS) guidelines using RMS Helios 401 PC-based spirometer and post-bronchodilator forced expiratory volume in one second (FEV1), Forced Vital Capacity (FVC), and FEV1/FVC values were recorded [16].
Adherence Calculation
Adherence to inhaled medication (only controllers) was determined objectively by checking the dose counters on Metered Dose Inhalers (MDI) or counting the DPI capsules and calculating the proportion of prescribed medication doses which were taken, averaged over the final four weeks. It was calculated as number of actuations or capsules taken/number of puffs or capsules prescribed in four weeks ×100. The adherence was capped at 100% to prevent overuse or dose dumping [14]. Self reported adherence was also measured by asking the patients about the number of days they have not taken their inhaler (containing ICS) in the prescribed dose in the preceding four weeks [11]. Using both the methodologies, the patient was said to be adherent if he has taken ≥80% of the prescribed doses [11,17]. Adherence rates derived from both methods were used separately to evaluate factors determining medication adherence.
Determinants of Medication Adherence
Different disease related factors (duration, symptom control, lung function test), patient (age, gender, literacy, employment etc) and therapy related (type of inhaler, duration of therapy etc) factors were selected by scrutinizing the existing literature [7,8,18] as well as utilizing current knowledge and experience. These variables were analyzed for their possible association with medication adherence using appropriate statistical tests (detailed below). Information on the drug as well as non-drug related reasons for non-adherence like apprehension about side effects and/or addiction, feeling of well being, forget fulness, non-availability of inhalers, social stigma, high inhaler cost, etc., was also collected from all patients. The data obtained was compared between the two adherence groups [11,19] for any possible association.
Statistical Analysis
Data were statistically described in terms of mean±standard deviation, median with range or frequencies, wherever appropriate. We used binary logistic regression analysis with forward inclusion approach to find association between potential determinants of inhaler adherence. Univariate and multivariate models were used to measure crude and adjusted OR respectively, with their 95% Confidence Intervals (CI), for different factors predicting adherence. Chi-square test was used to compare the reasons for non-adherence among to the two adherence groups. p-value was considered significant at <0.05.
Results
Total 103 patients of stable bronchial asthma were enrolled. Mean age was 41.9±16 years with 18 patients (17%) in the elderly age group. The median duration of asthma symptoms was four years [Inter Quartile Range (IQR): 2.5-10 years], however, median duration of use of inhaler was two years (IQR: 0.7-4 years) [Table/Fig-1]. On checking the inhaler technique, 72 (69%) patients were able to take their ICS inhaler correctly.
Baseline characteristics of asthma patients.
| S. No. | Parameters | Value |
|---|
| 1 | Age (mean±SD) | 41.9±16 |
| 2 | Gender |
| Male | 43 |
| Female | 60 |
| 3 | Literate (%) | 55 (53) |
| 4 | Employed (%) | 35 (34) |
| 5 | Smokers (%) | 31 (31) |
| 6 | Total duration of asthma in years (IQR) | 4 (2.5-10) |
| 7 | Duration of inhaler* use in years (IQR) | 2 (0.7-4) |
| 8 | Asthma symptom control (%) | 58 (56) |
| 9 | ICS adherence (%) | 73 (70.8) |
Determinants of Adherence
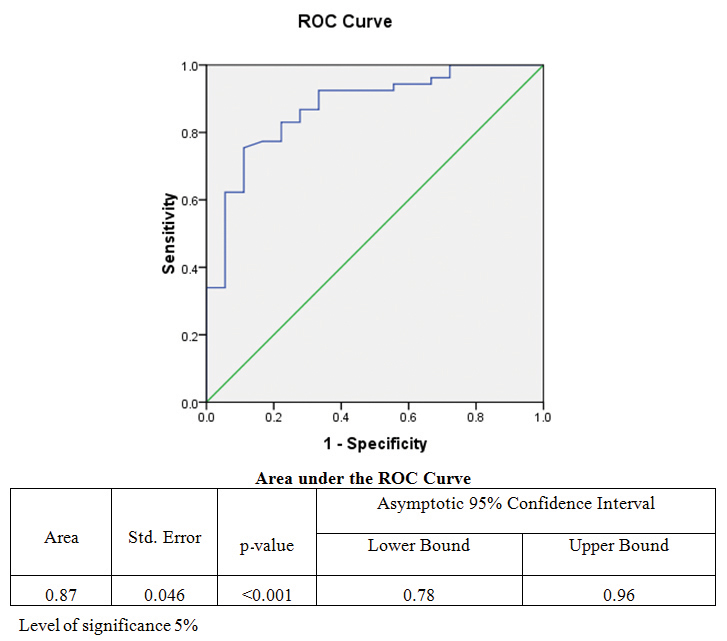
There was no significant difference in the medication adherence rates as determined by subjective and objective adherence tools (75.7% v/s 72.7%; p=0.77) [Table/Fig-2]. Different pre-defined variables as mentioned were evaluated for their possible association with adherence using univariate and multivariate logistic regression analysis using forward Lloyd’s Register’s (LR) approach [Table/Fig-3]. In the multivariate model, being literate, low FEV1 and asthma knowledge were found to be independent predictors of adherence to ICS using both subjective and objective adherence rates, whereas, use of DPI was significant factor in subjective adherence assessment only [Table/Fig-3]. The validity of correct classification of adherence using forward stepwise (likelihood) method was reported to close to 80%. Based on the four predictors, Receiver Operating Characteristic (ROC) curve [Table/Fig-4] was drawn which offers an excellent visual performance of the model, and the area under the curve (87%) suggests that the modelworks very well with minimum standard error of 0.038 and close to 95% confidence intervals for area.
Apprehension about side effects, feeling of well being and forget fulness (p=0.01 and 0.04 respectively) were found as the most common reasons for non-adherence given by the patients and found significant when compared between the two adherence groups [Table/Fig-5].
Distribution of patients between objective and subjective adherence measurements.
| Number of patients | Objective adherence (n=77) | Subjective adherence (n=103) | p-value |
|---|
| Adherent | 56 | 78 | 0.77 |
| Non-adherent | 21 | 25 |
Logistic regression analysis of predicted variables with adherence to inhaled corticosteroids.
| S. No. | Parameter | Univariate analysis(Objective adherence) | Multivariate analysis(Objective adherence) | Multivariate analysis(Subjective adherence) |
|---|
| Exp (B) (CI) | p-value | Exp (B) (CI) | p-value | Exp (B) (CI) | p-value |
|---|
| Patient related factors |
| 1 | Age <40 years | 1.72 (0.62-4.7) | 0.29 | | | | |
| 2 | Female | 0.82 (0.29-2.3) | 0.70 | | | | |
| 3 | Smoking | 0.92 (0.60-1.15) | 0.25 | | | | |
| 4 | Literate | 2.9 (1.04- 8.3) | 0.04 | 4.4 (1.1-20) | 0.04 | 4.2 (1.11-18.3) | 0.02 |
| 5 | Employed | 1.31 (0.43-4.0) | 0.63 | | | | |
| 6 | Asthma knowledge | 6.1 (1.9-19.7) | 0.003 | 7.3 (1.6-32.2) | 0.008 | 8.1 (2.2-31.5) | 0.001 |
| Disease related factors |
| 7 | Duration of symptoms | 0.95 (0.89-1.02) | 0.14 | | | | |
| 8 | FEV1 | 0.91 (0.87-0.96) | 0.001 | 0.91 (0.86- 0.97) | 0.003 | 0.9 (0.84-0.99) | 0.03 |
| 9 | Symptom control | 0.37 (0.12-1.06) | 0.06 | | | | |
| Therapy related factors |
| 10 | Duration of inhaler therapy | 0.99 (0.91-1.07) | 0.82 | | | | |
| 11 | Use of DPI | 4.5 (0.94-21.4) | 0.06 | | | 5.6 (1.2-26.1) | 0.03 |
CI: Confidence interval; FEV1: forced expiratory volume in one second; DPI: Dry Powder Inhaler
Receiver operating characteristic (ROC) curve for the binary logistic regression model generated for significant determinants of medication adherence.
Reasons for non-adherence to ICS among asthma patients.
| S. No | Reasons for non-adherence to ICS | Adherent group (n=78) | Non-adherent group (n=25) | p-value |
|---|
| 1 | Apprehension about side effects | 26 | 17 | 0.04 |
| 2 | Apprehension about addiction | 27 | 16 | 0.12 |
| 3 | Well being feeling | 19 | 16 | 0.01 |
| 4 | forgetfulness | 23 | 16 | 0.04 |
| 5 | Ill attitude towards medicines | 2 | 4 | 0.08 |
| 6 | High Cost | 17 | 12 | 0.09 |
| 7 | Social stigma | 27 | 15 | 0.26 |
| 8 | Non-availability of inhalers | 16 | 12 | 0.15 |
Discussion
The study evaluated the prevalence of medication adherence (to ICS) in bronchial asthma as well as the factors determining it in a subset of North Indian patients. The results showed a high non-adherence rate of 27.2% among asthma patients. Factors such as low FEV1, asthma knowledge and being literate were independently associated with adherence to inhaled corticosteroids.
In the present study, a total of 21 (27.2%) and 25 (24.2%) patients were found to be non-adherent to ICS by objective and subjective assessments respectively. There has been a wide variation in the adherence rates ranging from 9-80% reported in different studies across the globe [3-6]. A major reason behind this variability is the difference in adherence measurement tool employed in these studies. The present study compared both objective and subjective method for adherence measurement and found no significant difference in the adherence rates calculated using the two methods (p=0.77). In contrast, previous Indian studies [11,13,19] used only subjective method for adherence calculation which has limitations of poor recall bias and propensity to overestimate adherence [20]. Many western studies [5,8,14] have used electronic monitoring or medical refill records for measuring adherence which is not feasible in India in the current scenario.
The present study evaluated different patient, disease and therapy related factors that might determine adherence to asthma therapy. The results showed that being ‘literate’ increased 4.2 times the odds of adherence to ICS in asthma patients [Table/Fig-3]. The results are coherent with those from previous studies [11,15,21] as well as with a recent Cochrane analysis [22]. It is likely that education decreases communication gap between doctor and patient, as a result there is better patient understanding about the disease as well as motivation to take inhalers [23]. Also, literate patients are likely to be more efficient in self management of their asthma symptoms. Apart from the literacy status, knowledge about medication adherence in asthma was also a significant predictor of adherence to ICS in the present study using both subjective and objective adherence measures. The finding is supported by published data [3,15,18] and highlights the need for timely and periodic counselling of patients regarding the basic concepts of inhaler therapy.
Forced expiratory volume in one second, a measure of airflow limitation, is an objective marker of disease severity in asthma patients. It has been previously evaluated as potential determinant of adherence in asthma with inconsistent results [21,24,25]. The results from the present study showed that a decrease in FEV1 in patients with ongoing treatment was associated with increased adherence to ICS [Table/Fig-3]. This may be due to the fact that a low FEV1 represents a severer disease that might necessitate/ensure regular ICS use by the patients. In contrast to FEV1, asthma symptom control was found to be a poor predictor of adherence in the present study which indicates a poor correlation between perceived symptoms and lung function [26]. The results prove the superiority of objective parameter i.e. FEV1 over symptom control as a predictor of medication adherence. Lastly, the use of dry powder inhalers was also associated with medication adherence using self-reported adherence only, in the present study. Eventhough there is some previous evidence in favour of its association [27], the scientific reason behind it remains to be elucidated.
Older age has been related to better adherence in many previous studies [8,21]. It might be due to better motivation and discipline seen in the elderly towards their disease management. However, we could not find any such association in our study probably due to lesser number of elderly patients (n=18) in our study cohort [Table/Fig-3]. Duration of asthma is an important disease related factor that, similar to previous results [15,21,28] it could not qualify as a significant determinant of adherence. Poor motivation counteracted by increased severity due to prolonged disease might be reason for the insignificant association. Among socioeconomic factors, employment status has yielded mix results in previous studies [8]. The association between the two was found insignificant in our study (p= 0.63). In contrast, higher income has been found to be associated with adherence to ICS [25,29], however, this variable could not be analyzed in the present study due to difficulty in retrieving financial information from the patients.
The present study also extracted possible drug and non-drug related reasons for non-adherence from among the patients who defaulted to ICS [Table/Fig-5]. Forget fulness was the most important reason for non-drug related non-adherence. Apprehension about side effects and feeling of well-being were the predominant reasons for intentional non-adherence. These results are consistent with a previously conducted Indian study [11].
The present study evaluated a wide range of patient, disease and therapy related factors determining medication adherence in bronchial asthma patients using both objective and subjective adherence tools that probably has not been done previously in any Indian study. Comparative analysis of two different adherence measures increased the power of the study. Both adherence measures yielded similar predicting factors which increased the reliability of the results. The results have clearly demonstrated a high prevalence of non-adherence to ICS among Indian patients and have highlighted areas which need attention of the caregivers.
Limitation
The study employed objective method for adherence measurement in our study but that same could not be utilized in 26 patients where self-reported adherence was relied upon adherence estimation. Electronic monitoring of the inhaler use is considered gold standard tool for adherence measurement but its use is limited by the cost and feasibility in Indian settings. In light of this, the objective method used in the study seemed to be a reasonable option available. However, this method of dose counting is also associated with flaws which need to be considered while interpreting the results. Certain variables like income status and belief and behaviours about asthma that have been proved previously as adherence determinants could not be evaluated in our study [29,30]. The evaluations of disease relate beliefs and behaviours require questionnaires that have not yet been validated for Indian patients. Nevertheless, possible reasons for non-adherence as asked from patients gave a reasonable insight into this psychological part of medication adherence.
Conclusion
Ensuring adherence to inhaled controllers is vital for adequate control of asthma. The study yielded constructive data on medication adherence among asthma that is pertinent to Indian settings. Measures like imparting knowledge about asthma therapy particularly the importance of medication adherence, checking the technique for inhaler use and regular counselling of patients to remove their fears/doubts are simple, cost effective yet important management strategies that can go long way in ensuring adherence. Longitudinal studies evaluating the response of these educations interventions on medication adherence might further help to strengthen the evidence generated in the study.