Today, the patients with chronic disease are encouraged to take the responsibility of their own care and solve their problems [11]. In response to diagnosis of the chronic disease, the patients should change their usual habits, behaviors, and lifestyle [12,13]. Life style is important due to its effect on the QOL, health, and disease prevention [11,14].
According to the World Health Organisation (WHO), QOL is defined as “an individual’s perception of his position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns”. The QOL covers a wide range of economic, socio-cultural, and lifestyle factors [15]. There is a mutual relationship between the disease and the QOL, and the physical disorders directly affect all the aspects of QOL; however, the primary objective of treatment, especially in case of chronic diseases is to improve the QOL [11].
Since a large part of care activities, including low fat diets, increasing physical activity, and blood sugar and blood pressure self-control, occur outside the healthcare environments [16]. It might not be possible for all the patients to go to the hospital regularly; thus, it would be necessary to replace some alternative methods in order to increase the access to the secondary prevention and guide the patients. Some interventions such as the HELM intervention which is a brief intervention consisting of eight elements: refer to doctor, goal-setting with the client participation, an educational booklet, receiving risk-factor card based on patient’s risk factors, feed-back to patient, three phone calls, refrigerator magnet reminder and health diary program [17,18] and telephone calls, might be effective in getting access to the secondary prevention programs and guidance, which require active participation of the patients [19].
Given the increasing incidence of IHD, inappropriate lifestyle, necessity of health promotion behaviors, and lack of a specific self-management program after the patient’s discharge, the researcher was motivated to investigate and determine the effect of the HELM program on QOL of the patients with the IHDs.
Materials and Methods
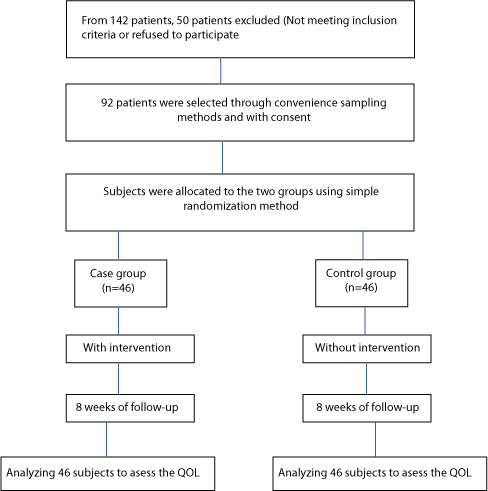
This was a single-blind, two-group quasi-experimental before-and-after study, the population of which included all the patients with IHD hospitalised in Farshchian Educational and Medical Centre Hamadan, Iran. The patients were selected using the convenience sampling method by researcher from July 2015 to October 2015. The sample size was calculated to 46 clients in each group (92 participants total) using 90% power with a two-sided significance level of α = 0.05 and the effect size of 0.70, based on the study conducted by Fernandez RS et al., [18].
The randomised allocation of the samples in the two interventions and control groups was performed by researcher and the patients did not know which group belongs to. The [Table/Fig-1] show the CONSORT of the study.
CONSORT flowchart of the study.
Inclusion criteria: living in Hamadan, the ability to read and write diagnosis of IHD and subsequent hospitalisation.
Exclusion criteria: incidence of underlying disease (renal, respiratory, endocrine, orthopaedic, movement diseases, cancer and stroke) during the study, moving to another city, and doctor’s prohibition for continuing participation in patient education program.
Data collection was performed using the demographic information questionnaire (age, gender, education, occupation, and marital status) and the MacNew QOL questionnaire (which is free-available). The MacNew QOL questionnaire is a questionnaire specifically designed for the patients with cardiac diseases, which includes 27 questions with a seven-grade Likert scale (ranging from always to never) and assesses three emotional (eleven items), physical (six items), and social (ten items) components [20]. In the component of emotional aspect, for example, client is asked about “How much of the time during the last 2 weeks have you felt frustrated, impatient or angry?” or “How often during the last two weeks have you felt worthless or inadequate?” In the component of physical aspect, the client is asked about “How often during the last two weeks have you felt worn out or low in energy?” or “How much shortness of breath have you experienced during the last two weeks while doing your day-to-day physical activities”. Some questions like: “How often during the last two weeks have you felt you were unable to do your usual social activities, or social activities with your family?” are questions example for assessing social components.
The range of scores for global QOL is 27-189. The range score for emotional, physical and social is 11-77, 6-42 and 10-70, respectively. Higher scores indicate better quality of life status.
It must be mentioned that Amirian Z et al., translated the questionnaire into Persian by Forward-backward method. They confirmed scientific validity of the questionnaire by content validity and reliability by test-retest (r=0.85) [21].
After obtaining and registration the necessary permissions from the Deputy of Research and Technology in the university (N: 9410015450 date: Jan, 2015), the researchers explained the research objectives, and by obtaining the written informed consent, sampling was started. The participants were allocated to the case and control groups through simple randomisation method. The case group underwent the HELM program and routine trainings, while the control group received only the routine trainings (which contain education on the control of disease without any special pattern like determining the patients’ goals, telephone follow up, completing the diaries).
In the case group, three 40-45 minutes sessions of individual training were held during hospitalisation (after establishing the patient’s clinical status), at the time of discharge, and one week after being discharged from the hospital. In the first session, the MacNew QOL questionnaire was completed by the patients; besides, the patients were educated about the IHD, prevalence and risk factors of disease, patient’s role in preventing the disease, necessity and methods of receiving information. In the second session, the emphasis was put on the disease control strategies and explanations were provided about the program, patients’ duties, and importance of controlling the disease; Then, the patients were given a booklet consisting of two parts: the first part included an introduction to the IHD as well as the relevant risk factors, and the second part focused on changing any of the risk factors, their positive role of self-care in controlling the disease. In this session, the patients were trained about the necessity of performing the activities such as completing their diaries and sticking the essential hints on the refrigerator magnets or anywhere that is in sight; furthermore, they were asked to record their daily activities such as the eating foods during a week or their physical activities; besides, the researcher helped determining the patients’ goals and also asked them to keep the record the goals in their diaries. In the third session, the researcher controlled the patients’ diaries and provided the patients with appropriate feedbacks. A general practitioner was also present in this session and, along with the researcher, answered the patients’ questions; besides, the physician helped writing the essential hints for refrigerator magnets. After finishing the three sessions, the researcher communicated the patients through three phone calls (the 2nd, 4th, and 6th weeks after being discharged) and, besides emphasizing on the importance of controlling the factors affecting the disease, provided the necessary explanations to remove the probable ambiguities. After eight weeks, the patients re-referred to the hospital and re-completed the QOL questionnaires.
In the control group, the patients received the usual cares commonly provided for the hospitalised patients; besides, they completed the QOL questionnaire during their hospitalisation and eight weeks later.
Statistical Analysis
Subsequent to data collection using questionnaires and data extraction, analysis of the obtained data was performed using SPSS (version 16.0) software. It should be noted that the significance level was considered as p<0.05.
Results
The mean age in the case and control groups was 49.67±11.02 and 49.96±10.36, respectively; furthermore, majority of the participants in the intervention and control groups were 55-64 and 45-54 years old, respectively. Majority of the patients in the both groups were male. The educational level of most of the participants in both groups was high school diploma [Table/Fig-2].
Demographic variables in two groups.
| Variables | Levels | Intervention(%) N | Control(%) N | Statistical test |
|---|
| Age (year) | ≤25 | 1 (2.2) | - | t=0.127df=90p=0.89 |
| 25-34 | 3 (6.5) | 2 (4.3) |
| 35-44 | 11 (23.9) | 10 (21.7) |
| 45-54 | 13 (28.3) | 20 (43.5) |
| 55-64 | 14 (30.4) | 9 (19.6) |
| ≥65 | 4 (8.7) | 5 (10.9) |
| SD±Mean | 49.67±11.02 | 49.96±10.36 |
| Gender | Male | 27 (58.7) | 31 (67.4) | χ2=1.49df=3p=0.68 |
| Female | 19 (41.3) | 15 (32.6) |
| Education | Elementary | 10 (21.7) | 7 (15.2) | Fisher=6.18p=0.92 |
| Middle school | 7 (15.2) | 8(17.4) |
| High school diploma | 24 (52.2) | 29 (63) |
| Associate degree | 2 (4.3) | - |
| Licentiate degree | 3 (6.5) | 2 (4.3) |
| Occupation | Unemployed | 21(45.7) | 17 (37) | Fisher=1.70p=0.51 |
| Self-employment | 20 (43.5) | 26 (56.5) |
| Employee | 5 (10.9) | 3 (6.5) |
| Marital status | Single | 1 (2.2) | 2 (4.3) | Fisher=1.35p=0.70 |
| Married | 42 (91.3) | 43 (93.5) |
| Divorced or widow | 3 (6.5) | 1 (2.2) |
Analysis of the data showed that, the mean global score of quality of life in case group was 94.93±19.94 and 94.89±13.06 in control group, before implementing the self-management program. There was no significant difference between the case and control groups in terms of the global mean score; That means that two group were the same in regard to global score of quality of life before intervention (p>0.05); however, after implementing the program, the mean global score of quality of life in case and control group was 118.70±11.61 and 90.28±12.67, respectively. There was a significant difference between the two groups in terms of the global mean score; it means that the self-management program had improved the quality of life of case group [Table/Fig-3].
Global score of quality of life in two groups before and after the intervention.
| Grouplevel intervention | Control(n=46) | Intervention(n=46) | Independent t-test |
|---|
| Before intervention | 94.89±13.06 | 94.93±19.94 | t=0.012p=0.991 |
| After intervention | 90.28±12.67 | 118.70±11.61 | t=11.21p<0.001 |
| Paired t-test | t=1.98p=0.053 | t=9.36p=0.001 | |
As shown in [Table/Fig-4] the mean score of the emotional, physical, and social aspects of quality of life in case and control group was the same before intervention (p>0.05), but after implementing the program, it was improved in case group comparing control group (p<0.05). It means that this program had improved the aspects of quality of life of case group.
Comparing the mean scores of quality of life in two groups before and after intervention.
| Aspects of QOL | Limit | Control | Intervention |
|---|
| Before(Mean±SD) | After(Mean±SD) | Paired t-test | Before(Mean±SD) | After(Mean±SD) | Paired t-test |
|---|
| p-value | t | p-value | t |
|---|
| Emotional aspect | 11-77 | 41.15±6.52 | 39.72±5.89 | 0.280 | 1.09 | 41.76±8.73 | 48.50±5.06 | <0.001 | 5.97 |
| Physical aspect | 6-42 | 17.93±4.62 | 16.70±4.64 | 0.150 | 1.64 | 17.83±5.72 | 23.52±3.78 | <0.001 | 6.93 |
| Social aspect | 10-70 | 35.80±8.25 | 33.87±8.98 | 0.160 | 1.42 | 35.17±8.75 | 46.67±6.99 | <0.001 | 8.77 |
Moreover, comparing the mean score of the emotional, physical, and social aspects of quality of life in the control group before and after the program indicated no significant difference (p>0.05); while, in the case group, the mean scores of emotional, physical, and social aspects were increased after implementing the self-management program (p<0.05). It means that the emotional, physical, and social aspects of quality of life of case group, whom were educated by self-management program, was higher than control group with routine education [Table/Fig-5].
Comparing the mean scores of quality of life in intervention and control group.
| Aspects of QOL | Limit | Before intervention | After intervention |
|---|
| Intervention(Mean±SD) | Control(Mean±SD) | Independent t-test | Intervention(Mean±SD) | Control(Mean±SD) | Independent t-test |
|---|
| p-value | t | p-value | t |
|---|
| Emotional aspect | 11-77 | 41.76±8.73 | 41.15±6.52 | 0.709. | 0.374 | 48.50±5.06 | 39.7±5.89 | <0.001 | 7.66 |
| Physical aspect | 6-42 | 17.83±5.72 | 17.93±4.62 | 0.920 | 0.100 | 23.52±3.78 | 16.70±4.64 | <0.001 | 7.72 |
| Social aspect | 10-70 | 35.17±8.75 | 35.80±8.25 | 0.723 | 0.355 | 46.67±6.99 | 33.87±8.98 | <0.001 | 7.62 |
Discussion
The present study was aimed to investigate the effect of a HELM program on the QOL of the patients with IHD. The obtained results showed that the use of such program would improve the QOL of these patients. This finding was consistent with the previous studies by Ataee E et al., Miri J et al., and Moattari M et al., indicating that self-management would improve the QOL of the patients [22-24].
According to the results of the statistical tests, comparing the total mean score of QOL and the scores of emotional, physical, and social aspects in the case and control groups indicated a significant increase after the intervention (p<0.001). Furthermore, The obtained results showed that this program affected the three emotional, physical, and social domains. These findings were consistent with findings of the previous studies conducted by Amirian Z et al., Cheraghi M et al., [21,25]. As for the physical domain, the study by Amirian Z et al., showed that regular physical activities at home would have considerable effects on the QOL of the patients undergoing the coronary artery bypass surgery; thus, it was recommended to train and encourage the patients to perform such activities after the surgery [21] Meanwhile, apropos of the social domain, the study by Cheraghi M et al., showed that an effective social and supportive care program is essential for improving the QOL of the patients [25]. In addition, the study of Alireza G et al., and Vahedian-azimi A et al., the study by Vahedian et al., showed that such programs could improve the QOL of the patients [4,5].
Furthermore, there was a significant difference before and after implementing the program in the intervention group (p<0.05). This result is confirmed by Seyam S and Heidarnia AR study [26]. They concluded that the QOL is related with factors such as education level, family life, and duration of disease; therefore, the QOL is not an unchangeable issue and can be improved by effective interventions. Ahn S et al., also showed that self-care health behaviors played important role in the QOL of the patients with CAD [27]. In another study, Gonzalez-Chica Da et al., concluded that insufficient information about health would lead to poor physical performance and increasing the health-related information would improve the QOL of the IHD patients [28].
Results of the present study indicated that the self-management intervention, including training, interview, and phone follow ups, affected the experimental group. Cramm J et al., confirmed that managing the heart diseases requires a multi-dimensional, patient-centered, and organized approach [10]. Furthermore, Leemrijse CJ et al., showed that the telephone programs had positive effects on managing the heart diseases [19]. Moreover, Free C et al., concluded that interventions such as text messages could increase the patients’ commitment to the treatment programs [29]. Besides, in an investigation on the motivations for self-management after an open heart surgery, Tayebi M et al., stated that it is necessary to apply some programs in order to achieve a successful self-management [30].
Limitation
The case and control group should complete the booklets every day. Furthermore, the written questionnaire should be answered before and after intervention; so it was possible clients did not complete the booklets or answering the questions with accuracy, because of their disease. The researcher explained the importance of answering to questions and helped the patients when necessary.
Conclusion
Results of the present research showed that the HELM program affected the QOL among the patients; furthermore, using this program was effective in all the three emotional, physical, and social dimensions. We can conclude that this program makes the clients feel more ability to exercise or physical activity, doing their day-to-day physical activities, and less dependency than before intervention. Besides, HELM might cause more relaxation, happiness, satisfaction or pleasure, and reduction the tension of the clients. It also increases the ability of clients to do social activities, and personal life. In general, this program would facilitate achieving the desirable health outcomes, performing the personal tasks, and having a useful and purposeful life; Finally, It can be concluded that by increasing the duration of such interventions, better results could be achieved for the patients.