Postpartum period is the first six weeks after giving birth. It is a period in which the maternal retrograde changes i.e., the reshaping of uterus and vagina, progressive changes i.e., having milk in the breasts, the return of normal menstrual periods and parental phase occur [1]. Due to various factors like hormonal imbalance after delivery, responsibility of taking care of the infant, adoption of the new maternal role and taking care of the family etc., most of the mothers, especially primiparous mothers experience many challenges during this period [2]. Postpartum period is a transition period for the mother and her family. Therefore, physical, psychological and social adaptation of mother and her family are essential in this period [3].
In the postpartum period, mothers do not have sufficient preparation, awareness and support so they usually undergo struggle with physical and psychological problems and lifestyle changes [4]. The first two weeks after giving birth is the most stressful period for primiparous women. Primiparous women in comparison to multiparous mothers need more support of family, friends and health care providers in the postpartum period [5]. Approximately 40% of women experience postpartum consequences and about 15% of women face potential problems that threaten their lives and suffer from the long-lasting consequences [6]. During this period some problems such as back pain, perinatal and haemorrhoids pain, are rarely considered and the mother must adapt herself to these problems [7]. On the other hand, the mother’s experiences of postpartum problems affect mothers physical and mental health as well as the health of her family members [8].
Health promoting behaviour is an activity that a person does in order to protect the health and prevent the disease. These behaviours include proper nutrition, regular exercise, avoiding destructive behaviours, timely detection of symptoms of physical disease, emotional control, stress management, independence, adaptability and improvement of interpersonal relationships in a social dimension [9]. Some factors such as demographic factors including gender, age, marital status, financial status, social norms, culture, mass media, national health policies, advertising practices and physical environment are associated with health promoting behaviours [10].
In the postpartum period, mothers often leave health promoting behaviours that were performed during pregnancy such as continuing healthcare, healthy eating, exercise and protection of their health and their babies, because of time confines and accessibility to resources. However, limiting the consumption of fruits and vegetables lead to decrease of essential vitamins in the body and risk of constipation and haemorrhoids. On the other hand, reduce physical activities and long rest in the bed may increase the risk of thrombosis [11,12]. Health promotion counselling can improve the health status of the mothers in the first year after the baby was born, and also increase the mother’s ability to maintain her performance when faced with a challenge [13].
Many primiparous mothers do not feel healthy and may encounter different problems such as change of lifestyle and lack of health promoting behaviours [14-16]. Therefore, taking into account the potential long-term effects that postpartum period may have on the physical, mental and social health of mothers and their family and with regard to the fact that midwives are the first health care persons who can help primiparous mothers and can recommend the health promoting behaviours to those women during postpartum period. The present study aimed to determine the effect of group consulting on health promotion behaviours during postpartum period on primiparous mothers.
Materials and Methods
This randomised clinical trial study (ID: IRCT2016030510426N10]) was conducted, on 112 primiparous mothers from March to September, 2016. Before conducting the study, permission was obtained from Deputy Dean of Health affairs of Hamadan University of Medical Sciences. The sampling strategy for selection of the participants was two-stage cluster sampling. In the first stage, Hamadan city was divided into five geographic districts (North, South, Center, East and West) and from each district, two health centers were randomly selected based on the list received from the health center in Hamadan city. Afterwards, the selected centers from each district were randomly assigned into two groups-experimental and control. Out of 20 health centers in Hamadan city, 10 health centers were selected (five in experimental group and five in control group).
In order to determine the number of samples, the study conducted by Ghodsbin F et al., was used [17]. By considering the Type I error 5% and power of 80% and taking 10% attrition into account, the required sample size for each group was 56. In order to extract the samples in each center, the cases of those mothers who were in the 38-40 weeks of pregnancy.
Inclusion criteria: Primiparous mothers, ability to read and write the Persian language, healthy baby weighing 2500 to 4000 g, no physical and mental illness, the absence of obstetric problems during the current pregnancy, lack of participating in the other educational programs and vaginal delivery.
Exclusion criteria: The exclusion criteria was immigration, hospitalisation of mother or baby in hospital for more than 48 hours after delivery, absence of the participants for more than one session in the counselling sessions, occurrence of stressful events like divorce, death of relatives or neonatal death during the study, lack of breastfeeding to infant, postpartum complications such as intense infection or bleeding were collected based on their household ID. Afterwards, the samples were randomly selected from extracted cases. The selected mothers were invited through phone calls for a briefing session wherein written consent to participate in the study were taken. Then in the three to five days after giving birth, when they visit the center for routine check-up, the demonstration was given to mothers for two groups. The study obtained Ethics Committee approval from Hamadan University of Medical and Health Sciences (IR.UMSHA.REC.1394.343).
The participants in both groups were interviewed to complete the questionnaires and if the mothers had caesarean, they were excluded from the study and another person was replaced according to the method described. In this study, the experimental group received 3 to 60 minutes counselling sessions in small groups of five to 10, which were held at the health center.
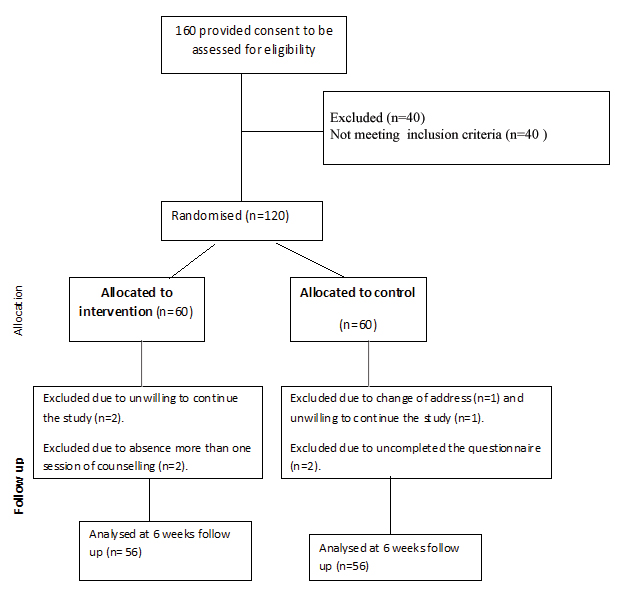
The women were selected randomly to receive either consultation and routine cares or only routine care. They were selected based on a convenient sampling method and were randomly allocated into experimental and control groups. So, that postpartum women who met the study’s criteria were assigned to either experimental or control group using permuted-block randomisation design. The allocation sequence was determined by one of the members of the research team, not involved in the sample selection, using a four-block randomised design. The participants were randomly assigned to the intervention and control group with a ratio of 1:1. The codes related to each woman were specified in envelopes in order not to expose the assignment procedure. Thus, the subjects were in A and B group according to the specified sequence. The CONSORT 2010 flow diagram for the study is given in [Table/Fig-1] which shows that 160 women were enrolled and filled the consent forms to be assessed for eligibility. Among them 40 women were excluded due to lack of eligibility of inclusion criteria. So, sixty women allocated to each group. In the experimental group, four women were excluded due to absence of more than one session of counselling (n=2) and unwillingness to continue the study (n=2). Therefore, information of 56 women were analysed in the experimental group. In the control group also four women were excluded due to change of address (n=1) unwillingness to continue the study (n=1), and uncompleted the post-test questionnaire (n=2). Finally, 56 postpartum women were analysed in the experimental group and 56 to the control group.
CONSORT diagram of recruitment to the study.
Therefore, if A was the experimental group and B was the control group, the participants would be divided by using randomised blocks (ABBA). The data analyser was not aware of the interventions provided to the groups.
Totally, 10 small groups with five to 10 peoples in each group performed in experimental group. The first, second and third consultation sessions were held three to five, 10-15 and 17-20 days after giving birth, respectively. The contents of health promotion counselling sessions have shown in the [Table/Fig-2].
Consulting sessions of the study during postpartum.
| Counselling sessions | Contents | Duration of sessions |
|---|
| First | Physiological changes during the postpartum, signs of danger, sexual health, lactation, nutrition of mother. Training on lactation. | 45-60 minutes |
| Second | Recognition of stress and its symptoms, strategies for coping with stress and relaxation, factors affecting interpersonal relations. Training on lactation and copying with stress. | 45-60 minutes |
| Third | Physical activity after giving birth, appropriate exercises for this period, self-actualisation and importance of spiritual issues in the health body and positive effects of relying on health. Training on lactation, copying with stress and physical activity. | 45-60 minutes |
After counselling sessions, in order to remind and follow up, the researcher once a week for three weeks called the participants in the experimental group. It is noteworthy that the researcher’s phone number was given to the participants in the experimental group to reply to the possible questions of the participants. In addition, a booklet was provided for the experimental group, based on accredited scientific books and sources, which consisted of the topics of advice. Then, 42 days after giving birth, when the participants of both groups visited the health centers to receive routine care of mother and baby, using interview, the questionnaires were completed by mothers in the two groups. At the end of the study, the control group also received the booklet.
In this study, two questionnaires were used to collect the data. The first questionnaire included sociodemographic characteristics of the participants of the study which contained questions concerning mother’s age, employment status, education, housing, average monthly income of households, planned or unplanned pregnancy, sex of the newborn, and the abortion experience. The second questionnaire was Health-Promoting Lifestyle Profile II (HPLPII) which measured health promoting behaviours as outcome of this study [18]. This questionnaire assesses the health promoting behaviours in the six dimensions of responsibility for health, spiritual growth and self-actualisation, supporting interpersonal, physical activity, nutrition and stress management, which includes 52 four-point likert scaled items ranging from never (1), sometimes (2) often (3), to always (4). The total score of health promoting behaviours ranged from 52 to 208 and for each dimension, the score can separately be calculated. The higher the scores, the better the level of health promoting behaviours and the lower the scores, the worse the level of health promoting behaviours. Mohamadian H et al., confirmed the validity and reliability of the test for Iranian context. Cronbach’s α coefficient was 0.86 for the HPLP II and for the subscales ranged from 0.70 to 0.77 [19]. In the present study, using Cronbach’s alpha, the reliability obtained for the total lifestyle was 0.83, indicating that the aforementioned questionnaire enjoyed acceptable reliability rate to be used in the present study.
Statistical Analysis
Data analysis was carried out using SPSS software version 20.0. Using Kolmogorov-Smirnov, the normality of quantitative variables was checked. The findings revealed that all of them were normally distributed. After collecting the required data, using Independent samples t-test, Fisher’s exact and Chi-square test, sociodemographic characteristics of the participants in both were examined. In order to investigate the difference between the two groups before and after the intervention, Independent Samples t-test was used. Moreover, in order to compare the mean difference within both groups before and after the intervention, Paired samples t-test was used. Analysis of covariance was used to control the effect of the score before intervention in the field of nutrition and physical activity. The significance level for all the tests was considered to be p<0.05.
Results
According to [Table/Fig-3], the mean of mother’s age in the experimental group was 23.46±4.75 and the mean of mothers age in the control group was 23.77±4.98 (p>0.050). To test the equality of variables in the experimental and control groups in the variables of job and education, Fisher’s exact test was used and Chi-square test was used for the other variables. The two groups were homogenous in terms of all relevant variables.
Mean of overall lifestyle’s score and its dimensions between and within the experimental and control Groups before and after the intervention is evident in [Table/Fig-4].
Comparing the socio-demographic characteristics of the mothers in both experimental and control groups.
| Variables | Experimental Group (N=56) | Control Group (N=56) |
|---|
| Mother’s age (years) | Mean | 23.46 | 23.77 |
| Standard Deviation | 4.75 | 4.98 |
| Frequency | Percent (%) | Frequency | Percent (%) |
| Mother’s job | Housewife | 52 | 92.9 | 52 | 92.9 |
| Employee | 4 | 7.1 | 4 | 7.1 |
| Mother’s education | High school | 22 | 39.3 | 23 | 41.1 |
| Diploma | 18 | 32.1 | 17 | 30.4 |
| Associate degree | 6 | 10.7 | 6 | 10.7 |
| Bachelor | 10 | 17.9 | 10 | 17.9 |
| Abortion experience | Yes | 8 | 14.3 | 6 | 10.7 |
| No | 48 | 85.7 | 50 | 89.2 |
| Planned pregnancy | Yes | 46 | 82.1 | 43 | 76.8 |
| No | 10 | 17.9 | 13 | 23.2 |
| Newborn gender | Male | 35 | 62.5 | 31 | 55.4 |
| Female | 21 | 37.5 | 25 | 44.6 |
| Vaginal delivery | With episiotomy | 36 | 64.3 | 39 | 69.6 |
| Without episiotomy | 10 | 17.9 | 9 | 16.1 |
| With tear | 10 | 17.9 | 8 | 14.3 |
| Household income (Toman* per month) | Less than one million | 27 | 48.2 | 26 | 46.4 |
| One-two million | 23 | 41.1 | 24 | 42.9 |
| More than two millions | 6 | 10.7 | 6 | 10.7 |
*Toman is Iranian currency; U.S. $ 1=Toman 3800
Comparing the mean of overall lifestyle’s score and its dimensions between and within the experimental and control groups before and after the intervention.
| Dimensions | Experimental GroupMean±SD | Control GroupMean±SD | Independent Samples t-test Before | p-valueAfter |
|---|
| Before | After | Before | After |
|---|
| Health responsibility | 37.89 (7.07) | 45.29 (4.48) | 37.66 (7.01) | 37.00 (7.31) | p=0.862t=0.17 | p<0.001t=7.23†† |
| p-value (paired samples t-test) | p<0.001t=13.06 | p=0.070t=1.85 |
| Self- actualisation | 23.66 (3.70) | 24.93 (3.18) | 23.45 (3.77) | 23.26 (5.29) | p=0.762t=0.30 | p=0.047t=2.01†† |
| p-value (paired samples t-test) | p<0.001t=10.27 | p=0.732t=0.34 |
| Interpersonal support | 21.77 (3.73) | 23.73 (3.20) | 21.54 (3.75) | 21.32 (3.61) | p=0.743t=0.33 | p<0.001t=3.74†† |
| p-value (paired samples t-test) | p<0.001t=10.91 | p=0.627t=0.49 |
| Stress management | 14.89 (2.98) | 20.87 (4.49) | 14.79 (2.88) | 14.63 (2.81) | p=0.847t=0.19 | p<0.001t=8.83†† |
| p-value (paired samples t-test) | p<0.001t=9.66 | p=0.258t=0.55 |
| Physical activity | 11.95 (3.26) | 17.91 (3.00) | 13.77 (2.82) | 13.88 (2.71) | p=0.002t=3.17 | p<0.001F=222.69§ |
| p-value (paired samples t-test) | p<0.001t=15.27 | p=0.515t=0.65 |
| Nutrition | 20.82 (3.74) | 26.70 (6.48) | 18.07 (3.59) | 17.80 (3.45) | p<0.001t=3.97 | p<0.001F=54.99§ |
| p-value (paired samples t-test) | p<0.001t=7.52 | p=0.249t=1.16 |
| Lifestyle (overall) | 130.98 (17.30) | 159.43 (15.12) | 129.34 (16.82) | 127.90 (16.27) | p=0.611t=0.51 | p<0.001t=11.10†† |
| p-value (paired samples t-test) | p<0.001t=17.57 | p=0.126t=1.55 |
††Independent Samples t-test; §Analysis of Covariance
Discussion
The findings of the study revealed that overall and dimensions of lifestyle’s scores of the experimental group increased significantly after the intervention, while no significant difference was found in the mean scores of the control group. In other words, health promoting behaviours counselling had a significant positive effect during postpartum period. The findings of the present study are in line with other studies. For instance, the findings of Kamalifard M et al., showed that training during postpartum period increased mothers’ knowledge and belief with regard to their lifestyle [12]. Furthermore, Ghodsbin F et al., found the significant difference between the mean score of quality of life pre-intervention and post-intervention between the two groups (p<0.001) [17]. Study conducted by Ahmadi SH et al., says that, breastfeeding consultation of mothers based on the Belief, Attitudes, Subjective Norm and Enabling Factors (BASNEF) model and using Great Ask, Tell Help, Explain and Return (GATHER) counselling steps increased the rate of exclusive breastfeeding, lactation performance and weight gain of premature infants [20]. However, the findings of the present study are in odds to those of some other studies. For example, Mendelson SG et al., showed that intervention program on women with gestational diabetes made no significant difference between the mean scores of health promoting lifestyle of the experimental and control groups [21]. One possible justification for the difference between the findings might be the different population and diabetes disease of the mothers.
In the present study, nutrition was investigated as one of the dimensions of health promoting behaviours and the findings of analysis of covariance revealed that after counselling, there was a significant difference between two groups on nutrition. In the experimental group, feeding behaviours improved significantly after the intervention, while no significant difference was found in the control group. The findings of the present study are in accordance with previous studies found that lifestyle education improved healthy nutritional behaviours during pregnancy and after giving birth [22,23].
With regard to women physical activity, the results of present study showed a significant difference between two groups after intervention. The finding is in accordance with McIntyre HD et al., study which reported early postpartum intervention increased physical activity in women with previous gestational diabetes [24]. After delivery in some mothers, lack of exercises and inappropriate nutritional behaviours have been observed. Therefore, adopting regular physical activity and healthy eating behaviours deemed necessary to maintain health and reduce the risk of weight gain during this period.
In the present study, after counselling a significant positive improvement on social support was found in the experimental group. The findings are in line with those of several studies. Chen CM et al., showed that social support was a predictor of all subscales of lifestyle in the postpartum period [25]. Likewise, Keller C et al., that investigated social support intervention in physical activity and losing weight after delivery, revealed that social support was necessary to improve physical activity and weight management in women [26]. Thornton P et al., also showed that social support was important to promote women lifestyle, improve eating behaviours and physical activity during pregnancy and after delivery [27]. Additionally, social support had a very important role in reducing the mothers vulnerability and stress [28].
The present study revealed that stress management score in the experimental group increased significantly after intervention. In order to handle stressful situations in postpartum mothers, stress management and relaxation techniques can be used. Perhaps, muscular relaxation program and focusing on breathing were effective in reducing the perceived stress [28]. During postpartum period, mothers are simultaneously forced to learn how to take care themselves and their infants. Failure to pay attention to mental and emotional conditions of the mother during postpartum leads to psychological problems for her and increase the rate of family conflicts. Family conflicts can lead to psychological problems in children and adolescents [29]. Therefore, health promotion counselling effectively can help mothers to manage their stress.
The present study results showed the positive effects of health promoting behaviours in promoting a sense of health responsibility, spiritual growth and self-actualisation during postpartum periods. Also, Chen CM et al., found that counselling improved health responsibility, spiritual growth and self-actualisation in Taiwanese postpartum women [25].
Limitation
It can be noted that the intervention program could not be continued for longer period of time due to the condition of the mothers during postpartum period, while programs for changing behaviour need more time and continuous trainings. In addition, this study was conducted only on urban populations. Further research is suggested to use other approaches of counselling to improve health behaviours and lifestyle. Moreover, further research is deemed essential to replicate this study in the rural communities and ethnic groups.
Conclusion
The results of this study showed that health promoting behaviours utilisation counselling had an effective role in improving the mothers’ lifestyle during postpartum period. Counselling process leads to change of perceptions, beliefs, attitudes, behaviours, and finally results in changing lifestyle. Considering the fact that a midwife is the first health care person through which mother can receive her counselling after giving birth, and with regard to the importance of mothers’ health in this critical period. It is recommended that the health promoting behaviours counselling should be done by midwives for all mothers during postpartum period as it is easy and has no consequences, it is affordable and promotes mothers and neonates health status.
*Toman is Iranian currency; U.S. $ 1=Toman 3800
††Independent Samples t-test; §Analysis of Covariance