Colloid Cyst – A Small Third Ventricle Cyst with Unusual Psammomatous Calcifications
Sadaf Khan1, Manna Valiathan2
1 Postgraduate Student, Department of Pathology, Kasturba Medical College, Manipal, Karnataka, India.
2 Professor and Head, Department of Pathology, Kasturba Medical College, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sadaf Khan, Postgraduate Student, Department of Pathology, Centre for Basic Sciences, Kasturba Medical College, Manipal-576104, Karnataka, India.
E-mail: sadaf519@gmail.com
We report a case of a colloid cyst in the foramen of Monro, with an unusual finding of psammomatous calcifications. Colloid cysts of the third ventricle with calcifications in the wall are very rare. Colloid cysts are benign, slowly progressing lesions that most often arise from the roof of the anterior third of the ventricle along the foramen of Monro, account for almost 0.5-2% of all intracranial neoplasms, ranging from 1 to 3 cm in diameter and contain intraluminal homogenous mucoid or semi-solid colloid like material. Few cases have also been reported in septum pellucidum and fourth ventricle. They are usually incidentally discovered or can cause repeated attacks of worsening headache, syncope, memory loss and visual disturbances.
Benign cyst, Foramen of Monro, Rare
Case Report
A 48-year-old male patient, a known diabetic, presented with complaints of holocranial headache, associated with blurring of vision, diplopia and episodes of vomiting at the peak of headache since 15 days. The patient also had imbalance while walking and urinary incontinence. There was no history of loss of consciousness, black-outs, motor weakness or cranial weakness.
On neurological examination, all higher mental functions were normal. There was papilledema in the second cranial nerve with no evidence of any motor or sensory deficit.
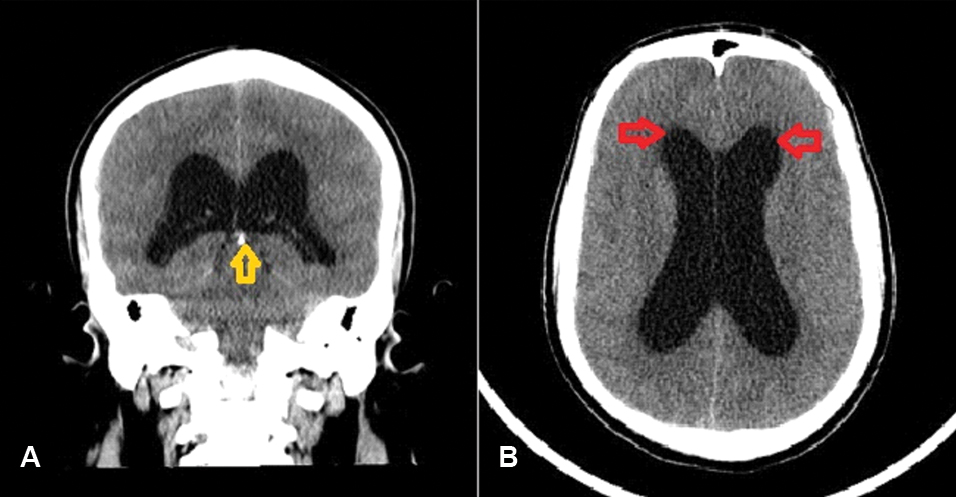
On radiological investigations, CT scan showed a well-defined hyperdense lesion with peripheral hypodensity noted in the region of foramen of Monro causing dilation of bilateral ventricles with periventricular Cerebrospinal Fluid (CSF) seepage along with tiny calcifications along falx cerebri [Table/Fig-1a,b].
a) Plain CT Brain (coronal section) showing calcification in the falx cerebri; b) and the periventricular luscency along bilateral frontal horns.
MRI revealed a non-enhancing cystic lesion, measuring (2.1 cm × 1.7 cm × 1.7 cm) in the region of anterior third ventricle along foramen of Monro, appearing hypointense on T1 Weighted Image (T1wi) and hyperintense on T2 Weighted Image (T2wi), with mild signal suppression on FLAIR without diffusion restriction and having a dependent central T1 hyperintense/ T2 hypointense area blooming in Susceptibility Weighted Image (SWi) (suggestive of subacute haemorrhage) along with mild dilation of lateral ventricles and periventricular seepage.
The patient was admitted with the above complaints and taken up for cyst excision via right interhemispheric approach.
Histopathology
Grossly, the cyst was received in four irregular bits, largest bit measuring (0.5 cm × 0.5 cm × 0.5 cm) and showed grey white areas on cut section.
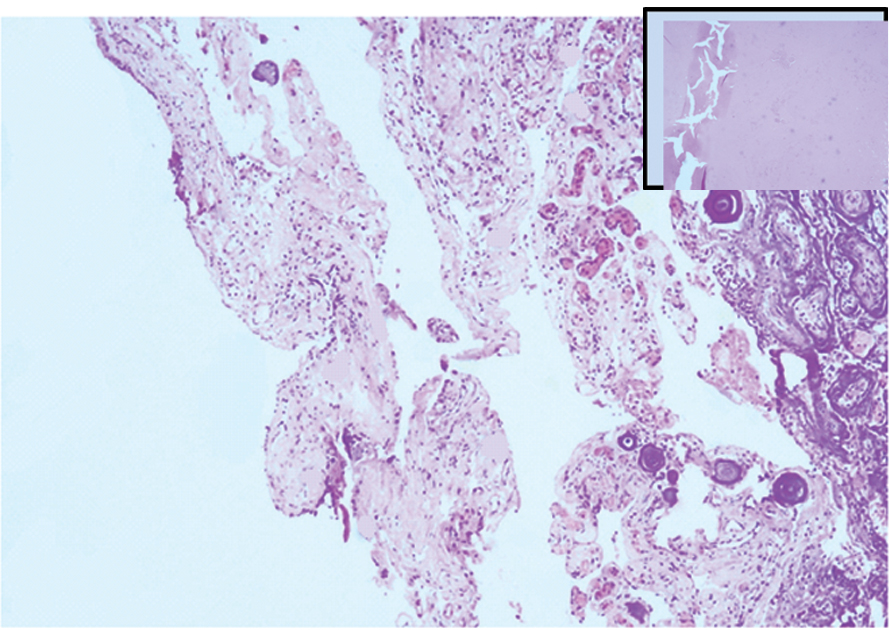
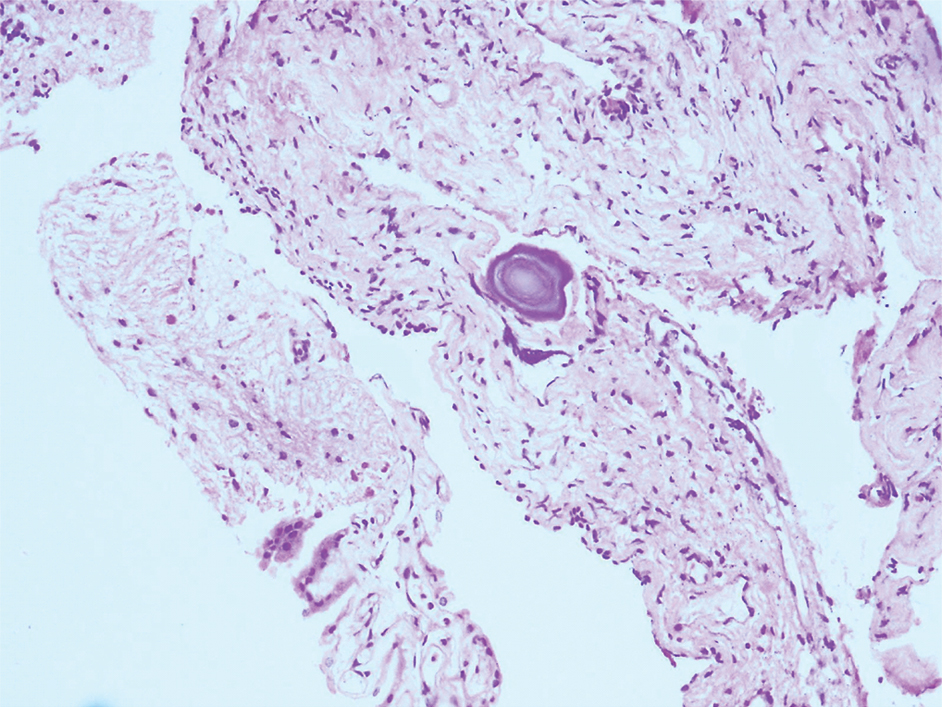
Microscopically, sections showed a cyst wall focally lined by ciliated pseudostratified columnar epithelium enclosing intraluminal acellular mucinous eosinophilic material and cystic macrophages [Table/Fig-2,3]. The cyst wall was composed of fibrocollagenous stroma showing proliferating congested blood vessels, numerous micro and macro dystrophic calcifications resembling psammoma bodies and occasional cystic macrophages [Table/Fig-4,5].
Cyst wall composed of fibrocollagenous stroma showing psammomatous calcifications and congested blood vessels. Inset showing intraluminal acellular mucinous material. (H&E 10X).
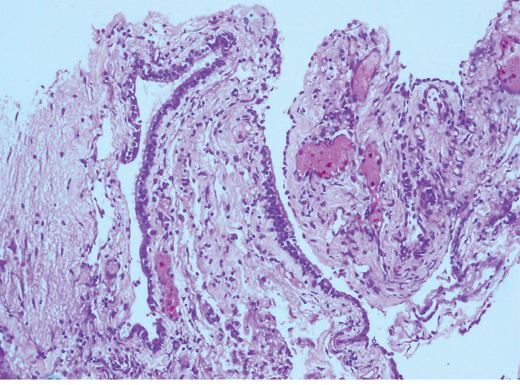
Cyst wall focally lined by pseudostratified ciliated epithelium (H&E 20X).
Cyst wall showing psammomatous calcification and cyst macrophages (H&E 20X).
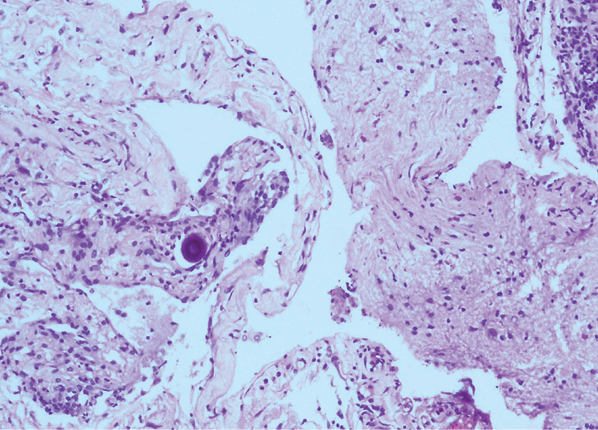
Cyst wall with focal ciliated columnar epithelium overlying fibrocollagenous stroma showing psammomatous calcification (H&E 20X).
Following the cyst excision, patient made a good post-operative recovery and was discharged. At a follow up interval of four months, he continued to be neurologically intact.
Discussion
Colloid cysts are rare developmental cysts, benign in nature, constituting 0.5-2% of all intracranial neoplasms and ranging from 1 to 3 cm in diameter [1,2]. Their typical location is on the roof of the anterior third ventricle along the foramen of Monro. The frequent clinical presentation is with features of increased intracranial pressure by virtue of their site of occurrence. Rare examples of colloid cysts have also been seen in the fourth ventricle, lateral ventricles, and outside the ventricular system [3-6]. They can be distinguished from other similar benign cysts such as enterogenous cyst, ependymal cyst and Rathke cleft cyst on the basis of their respective locations.
The term colloid is derived from the Greek word ‘kollodes’ which means resembling glue and grossly it varies in consistency based on the contents of the cyst which range from semi-solid to viscous with gelatinous appearance and are thought to be derivatives of the secretory fluid and breakdown products of the cyst wall [7].
On histological examination, colloid cysts are characteristically lined by a simple to pseudostratified epithelium along with scattered ciliated cells, interspersed mucous goblet cells overlying connective tissue. The cyst encloses amorphous material which is Periodic acid-Schiff (PAS) positive, sometimes showing cholesterol clefts or necrotic leukocytes or both. Occasionally, the cyst wall can undergo secondary xanthogranulomatous reaction resulting from a chemical irritation from cholesterol, hemorrhage, or the colloid material itself [8].
Ultrastructural analysis by Ho KL and Garcia JH have shown ciliated cells and non-ciliated cells showing microvilli, goblet cells with secretory granules, basal cells and undifferentiated cells having scanty organelles [9]. The mucus producing ciliated cells are thought to have an endodermal origin while the topographical distribution of the ciliated epithelial cells suggests respiratory origin and the distally tapering cilia are theorized to have an olfactory origin [10].
Spectroscopic studies have shown the cyst to vary from hypointense and isointense to hyperintense. The existence of numerous ions such as calcium, sodium and magnesium intermixed with the mucinous amorphous contents of the cyst wall have been thought to impart the high density of these lesions compared to brain parenchyma on CT scan [3].
On MRI, the appearance of the cyst varies, most commonly being hyperintense as compared to the brain parenchyma on T1wi and hypointense to the brain parenchyma on T2wi [7]. Despite the fact that calcium ions are found routinely within the contents of the cyst wall, calcification of the cyst wall has been observed very rarely. Previously, only 13 such cases with calcific nodules in the cyst wall have been reported in the literature, out of which four were giant (>3 cm in diameter) in size [2,11,12]. The present case report calcifications were seen in the form of concentric basophilic lamellated psammoma bodies which is a unique finding; previously documented in only a single case [11].
It becomes extremely important to diagnose colloid cyst preoperatively and intraoperatively and distinguish it from other neoplastic conditions, since, its benign nature imparts a good prognosis, low risk of recurrence [2] and the mode of treatment varies based on the size and consistency of the cyst varying from cyst drainage, wide fenestration, and subtotal capsular resection to complete cyst excision.
Conclusion
This is a rare case of colloid cyst wall with psammomatous calcifications, in a 48-year-old diabetic male patient which at times may present with acute hydrocephalus and prove fatal. Previously, only 13 cases of colloid cyst with calcific nodules in the cyst wall have been reported in the literature; out of which only a single case had lamellated concentric psammomatous calcifications, which makes this case interesting. It is imperative to make a preoperative and intraoperative diagnosis and distinguish this entity from other neoplasms because it carries an excellent prognosis on total excision.
[1]. Türe U, Hiçdönmez T, Elmaci I, Peker S, Solid-calcified colloid cyst of the third ventricleClin Neurol Neurosurg 2001 103(1):51-55. [Google Scholar]
[2]. Yüceer N, Başkaya M, Gökalp HZ, Huge colloid cyst of the third ventricle associated with calcification in the cyst wallNeurosurg Rev 1996 19(2):131-33. [Google Scholar]
[3]. Two A, Christian E, Mathew A, Giannotta S, Zada G, Giant, calcified colloid cyst of the lateral ventricleJ Clin Neurosci 2016 24:06-09. [Google Scholar]
[4]. Bertalanffy H, Kretzschmar H, Gilsbach JM, Ott D, Mohadjer M, Large colloid cyst in lateral ventricle simulating brain tumour. Case reportActa Neurochir (Wien) 1990 104(3-4):151-55. [Google Scholar]
[5]. Jan M, Ba Zeze V, Velut S, Colloid cyst of the fourth ventricle: diagnostic problems and pathogenic considerationsNeurosurgery 1989 24(6):939-42. [Google Scholar]
[6]. Campbell DA, Varma TR, An extraventricular colloid cyst; case reportBr J Neurosurg 1991 5(5):519-22. [Google Scholar]
[7]. Armao D, Castillo M, Chen H, Kwock L, Colloid cyst of the third ventricle: imaging-pathologic correlationAJNR Am J Neuroradiol 2000 21(8):1470-77. [Google Scholar]
[8]. Hadfield MG, Ghatak NR, Wanger GP, Xanthogranulomatous colloid cyst of the third ventricleActa Neuropathol (Berl) 1985 66(4):343-46. [Google Scholar]
[9]. Ho KL, Garcia JH, Colloid cysts of the third ventricle: ultrastructural features are compatible with endodermal derivationActa Neuropathol 1992 83(6):605-12. [Google Scholar]
[10]. Navatha V, Veena KL, Colloid cyst in third ventricle- a rare caseMRIMS J Health sciences 2014 2(2):113-15. [Google Scholar]
[11]. Michels LG, Rutz D, Colloid cysts of the third ventricle. A radiologic-pathologic correlationArch Neurol 1982 Oct 39(10):640-43. [Google Scholar]
[12]. Sambasivan M, Padmanabhan S, Sambasivan M, Large colloid cyst of the anterior third ventricle associated with calcification in the cyst wallNeurol India 2010 58(2):330-31. [Google Scholar]