Knot of Henry: Role in Tendon Transfer
Parul Kaushal1, Aritra Banerjee2, Pushpa Dhar3
1 Senior Resident, Department of Anatomy, AIIMS, New Delhi, India.
2 Junior Resident, Department of Anatomy, AIIMS, New Delhi, India.
3 Professor, Department of Anatomy, AIIMS, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pushpa Dhar, Room No 1003, Professor, Department of Anatomy, Teaching Block, AIIMS, New Delhi-110029, India.
E-mail: dharpushpa@hotmail.com
The term “Master knot of Henry” refers to the site of cross connections between long (extrinsic) tendons of foot namely Flexor Digitorum Longus Tendon (FDLT) and Flexor Hallucis Longus Tendon (FHLT). This chiasmatic structure in the second layer of sole, was first described by Henry in 1940. Over the years it has gained importance because of its close association with surgical procedures such as ‘Tendon Transfers’, whereby insertion of a muscle-tendon unit is relocated at another site for restoration of lost function. The demand for these surgical procedures is constantly increasing in parallel with increasing number of irreparable nerve injuries, spinal cord injuries and road traffic accidents etc.
Both FDLT and FHLT are identified as potential tendon transfer candidates and variations of cross connections between FDLT and FHLT at Henry’s knot have been reported. In the majority of cases, slips proceeding from FHLT to FDLT have been observed. However, we observed the presence of two variant tendinous slips extending from the FDLT to FHLT, one lying proximal and the other distal to the chiasmatic crossover, in left foot of a male cadaver. Awareness regarding possible variations with context to the cross pattern at the knot could be the determining factor in deciding about the preferential tendon transfer candidate with maximal preservation of functioning of hallux as well as other little digits.
Chiasma tendon, Flexor digitorum longus, Flexor hallucis longus
Case Report
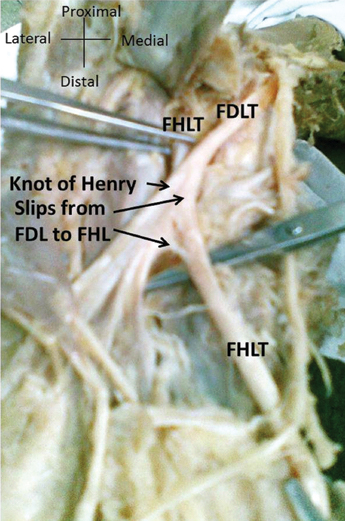
During routine dissection in the Department of Anatomy, AIIMS, New Delhi, India, a varied pattern of chiasmatic tendinous interconnection was observed in left sided sole of a 65-year-old male cadaver of Indian origin. Two anomalous tendinous slips extending from the FDLT to FHLT were noted, one slip lying proximal and the other distal to the crossover site (knot of Henry) [Table/Fig-1]. The neighbouring structures in the vicinity presented a conventional pattern. No such pattern was observed in the sole of the right side.
Photograph of the sole of the foot showing anomalous slips extending from the Flexor Digitorum Longus (FDLT) to Flexor Hallucis Longus Tendon (FHLT).
Discussion
Tendon transfers are surgical reconstructive procedures undertaken for restoration of injury induced functional loss in lower as well as upper limbs. In case of lower limbs, tendon transfer of FDLT/FHLT into tibialis posterior tendon is an accepted practice for treating patients with tibialis posterior dysfunction (considered as the most common cause of acquired flat foot) [1]. Though the success of such procedures is majorly determined by careful planning and preparation by the surgeon, yet the importance of varied architectural pattern in outcome of such situations cannot be undermined. Flexor Digitorum Longus (FDL) originates from the posterior surface of the tibia medial to tibialis posterior, just below the soleal line. Its tendon enters the sole by passing posterior to the medial malleolus. In the sole of foot, on the medial side of the tendon of Flexor Hallucis Longus (FHL), it splits into four separate tendinous slips (one each for the second to fifth toes) that get attached to bases of their distal phalanges. FHL after originating from the distal two-thirds of the posterior surface of the fibula and the adjacent interosseous membrane passes obliquely in the posterior compartment of the leg. This tendon grooves the posterior surface of the lower end of the tibia before passing forwards in the second layer like a bowstring and crossing FDLT from lateral to medial aspect. The final insertion of FHL is at the base of the distal phalanx of the hallux [2]. Majority of the studies have revealed variable slips going from FHLT to FDLT, thereby making FDLT as the tendon of choice for transfer [3].
Adoption of intricate and minimally invasive procedures such as tendon transfers especially in conditions like tibialis posterior insufficiency and Achilles tendon repair have rekindled the interest and inquisitiveness regarding knowledge of tendon arrangement. Variation observed in the present case vouched in favour of FDLT as the potential donor Muscle Tendon Unit (MTU). LaRue BG and Anctil EP, based on dissection of 24 cadavers, described three types of anatomic relationship between FHLT and FDLT at Henry’s Knot. Single connection between the two was described as type 1, double connection as type 2 and no connection as type 3 [4]. The variant encountered in the present case falls under type 2. Variation in the break-down of a common foetal tendon plate during formation could form the embryological basis of such variable interconnections between plantar tendons [5]. The tendons of FDL, FHL and peroneus brevis happen to be the most explored tendons among the autologous tendon transfers for Achilles tendon repairs. A retrospective study conducted by Qu JF et al., compared the success rates in repair of chronic rupture of Achilles tendon using different tendons. They observed an overall success rate of 80% in patients (5 cases) with FDLT transfers, while 100% success rate was demonstrated by patients (8 cases) with FHLT transfers after follow up of 24 months, thereby, proposing FHLT as the tendon of choice for such procedures [6]. On the other hand, O’Sullivan E et al., observed that transection of FDLT proximal to the region of the knot of Henry could prove helpful in maintenance of function of the hallux and lesser digits in cases of repair of tibialis posterior dysfunction [7]. Thus, thorough awareness regarding varied intertendinous connectivity between FHLT and FDLT could prove crucial in determining the specific donor tendon for correction of a specific deformity. Both, FHLT and FDLT, possess unique features as donor tendons. The anatomic location together with the strength and length of FHLT go in its favour as the preferred choice in tendon transaction. One of the biggest advantages of using FHLT is its anatomic location which minimises trauma to adjacent structures. Besides, Its strength, its length (10-12 cm) also aid in bridging large defects [8]. However, a recent study based on the gross dissection of 50 cadavers reported FHLT as a better candidate for tendon transfers intended to restore function of the foot but have speculated long term functional damage based on the harvesting procedure adopted and insertion of quadratus plantae [9].
Conclusion
These speculations lay emphasis on the fact that the choice of donor tendon should be based on the individual patient’s needs. Since, FHLT and FDLT are routinely used in reconstructive foot and ankle surgery; hence, awareness of their varied anatomy becomes imperative.
[1]. Sammer DM, Chung KC, Tendon Transfers Part I: Principles of transfer and transfers for radial nerve palsyPlast Reconstr Surg 2009 123(5):169e-77e. [Google Scholar]
[2]. Standring S, Gray’s anatomy: The anatomical Basis of Clinical Practice 2014 41st EditionEdinburg, LondonElsevier Churchill livingstone:1410-11. [Google Scholar]
[3]. Plaass C, Abuharbid G, Waizy H, Ochs M, Stukenborg-Colsman C, Schmiedl A, Anatomical variations of the flexor hallucis longus and flexor digitorum longus in the chiasma plantareFoot Ankle Int 2013 34(11):1580-87. [Google Scholar]
[4]. LaRue BG, Anctil EP, Distal anatomical relationship of the flexor hallucis longus and flexor digitorum longus tendonsFoot Ankle Int 2006 27(7):528-32. [Google Scholar]
[5]. Lewis OJ, Functional morphology of the evolving hand and foot 1989 OxfordClarendon Press:260-266. [Google Scholar]
[6]. Qu JF, Cao LH, Zhao HB, Gao JH, Li SG, Du XJ, Flexor digitorum (hallucis) longus muscle tendon transfer in the repair of old rupture of the Achilles tendonZhongguo Gu Shang 2008 21(4):297-99. [Google Scholar]
[7]. O’Sullivan E, Carare-Nnadi R, Greenslade J, Bowyer G, Clinical significance of variations in the interconnections between flexor digitorum longus and flexor halluces longus in the region of the knot of HenryClin Anat 2005 18(2):121-25. [Google Scholar]
[8]. Maffulli N, Ajis A, Management of chronic ruptures of the Achilles tendonJ Bone Joint Surg Am 2008 90(6):1348-60. [Google Scholar]
[9]. Pretterklieber B, The high variability of the chiasma plantare and the long flexor tendons: Anatomical aspects of tendon transfer in foot surgeryAnn Anat 2017 211:21-32. [Google Scholar]