Antimicrobial resistance in pathogens to most common antibiotics has become a major cause for concern. The O’Neill J review estimates that 10 million people will die every year as a result of antimicrobial resistance; more people than currently die from cancer [1]. Urinary Tract Infections (UTIs) are among the most common infections seen around the world, especially among women. They are also a common complication in catheterised patients. Moreover, they have become an important cause of morbidity with the rising incidence of antibiotic resistance in causative bacteria like E. coli and Klebsiella pneumoniae [2].
Therefore, there is a need to find alternate or adjuvant modalities to treat UTIs, particularly those caused by MDR isolates.
Vitamin C presents one such alternative. It is cheap, easily available and has few or no adverse effects [3]. It is widely prescribed as a nutritional supplement. It has established antioxidant effects and has been used as an adjuvant in cancer chemotherapy [4].
Several studies have shown that vitamin C, in the form of ascorbic acid exerts significant antibacterial effects on pathogenic organisms like Staphylococcus aureus, Enterococcus faecalis, Bacillus subtillis and Corynebacterium diphtheria [5,6]. Studies have demonstrated that vitamin C inhibits Helicobacter pylori, a well known risk factor for carcinoma and also Mycobacterium tuberculosis [7,8]. Furthermore, ascorbic acid has been shown to enhance the inhibitory effect of levofloxacin on biofilm formation on urethral catheters [9].
A study has demonstrated the inhibitory effect of vitamin C salts such as copper ascorbate on bacteria such as Serratia marcescens [10]. A previous study, also demonstrated that sodium ascorbate had some synergistic activity with ciprofloxacin against Pseudomonas aeruginosa biofilms [11].
Despite evidence in its support, vitamin C is still not considered in routine clinical practice for its antibacterial action, and need of more substantiated data. This study aims to determine the in vitro interaction between vitamin C (ascorbic acid and sodium ascorbate) and ciprofloxacin, an antibiotic commonly used to treat UTIs, against urinary isolates of E. coli and to determine if there is any synergistic activity between them. This could serve as the basis for future studies to evaluate the clinical use of vitamin C as an adjuvant to antibacterial therapy. The objectives of this study was to determine the growth of the urinary isolates of E. coli in the presence of vitamin C, ciprofloxacin and combination of vitamin C and ciprofloxacin respectively by spectrophotometry. And, to compare the absorbance values to determine whether there was a significant difference between growth inhibition by ciprofloxacin alone, and ciprofloxacin in combination with vitamin C.
Materials and Methods
The present laboratory based, prospective study was conducted at Department of Microbiology, Pondicherry Institute of Medical Sciences, Puducherry between August to September 2016. During this period, 72 isolates of E. coli were obtained from urine samples of suspected UTI patients, processed in the laboratory. Out of these, 50 isolates were selected by simple random sampling. As study focuses only on E. coli, all other urinary isolates were excluded. The study was cleared by the Institute Ethics Committee and a waiver of consent was obtained as the study did not involve human participants.
Urine samples from patients with suspected UTIs were processed by standard methods. All E. coli isolates were identified as per standard microbiological protocols [12]. Ciprofloxacin sensitivity of isolates was determined by Kirby-Bauer disk diffusion method [12].
Freshly prepared broths of E. coli in peptone water, incubated for two hours were used for the tests. Trypticase Soy Broth (TSB) (Himedia) was prepared following manufacturer’s instructions. Vitamin C-supplemented TSB was freshly prepared by adding Vitamin C to sterile TSB in two sets of sterile test tubes such that the final concentrations were 5 mg/mL and 10 mg/mL, respectively. These concentrations were used as per the study by Isela SN et al., [5]. Two forms of vitamin C were utilised for this study, L-ascorbic acid (Himedia) (Lot No. 0000204834) and sodium L-ascorbate (Sigma) (Lot No.SLBM1708V). Solubility and mean absorbance of ascorbic acid and sodium ascorbate differ; hence, two forms were used. Ciprofloxacin supplemented TSB was prepared by adding ciprofloxacin powder (HiMedia) (Lot No.0000000943) to TSB to a final concentration of 1 μg/mL (cut off for sensitive as per CLSI 2015 guidelines) [13]. Similarly, combinations of vitamin C and ciprofloxacin were prepared for the respective concentrations. A 250 μL of a two hour old bacterial broth (E. coli) was inoculated into each of these tubes and incubated at 37°C overnight, under aerobic conditions.
A 250 μL of bacterial broth (E. coli, clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control. Ciprofloxacin and vitamin C (ascorbic acid and sodium ascorbate) alone without bacterial culture were used as control for baseline absorbance values. E. coli ATCC® 25922™ was tested and absorbance value was noted for assessing vitamin C efficacy.
Absorbance of the inoculated broths and controls were measured by spectrophotometry at 450 nm as per Koch’s recommendations [14]. The absorbance values for the sensitive and resistant isolates were analysed. The mean absorbance for both ascorbic acid and sodium ascorbate at different concentrations was calculated.
Statistical Analysis
Statistical analysis was carried out using SPSS version 20.0. Unpaired t-test and multivariate analysis by ANOVA were used to compare the mean absorbance of the isolates. A p-value <0.05 was considered statistically significant.
Results
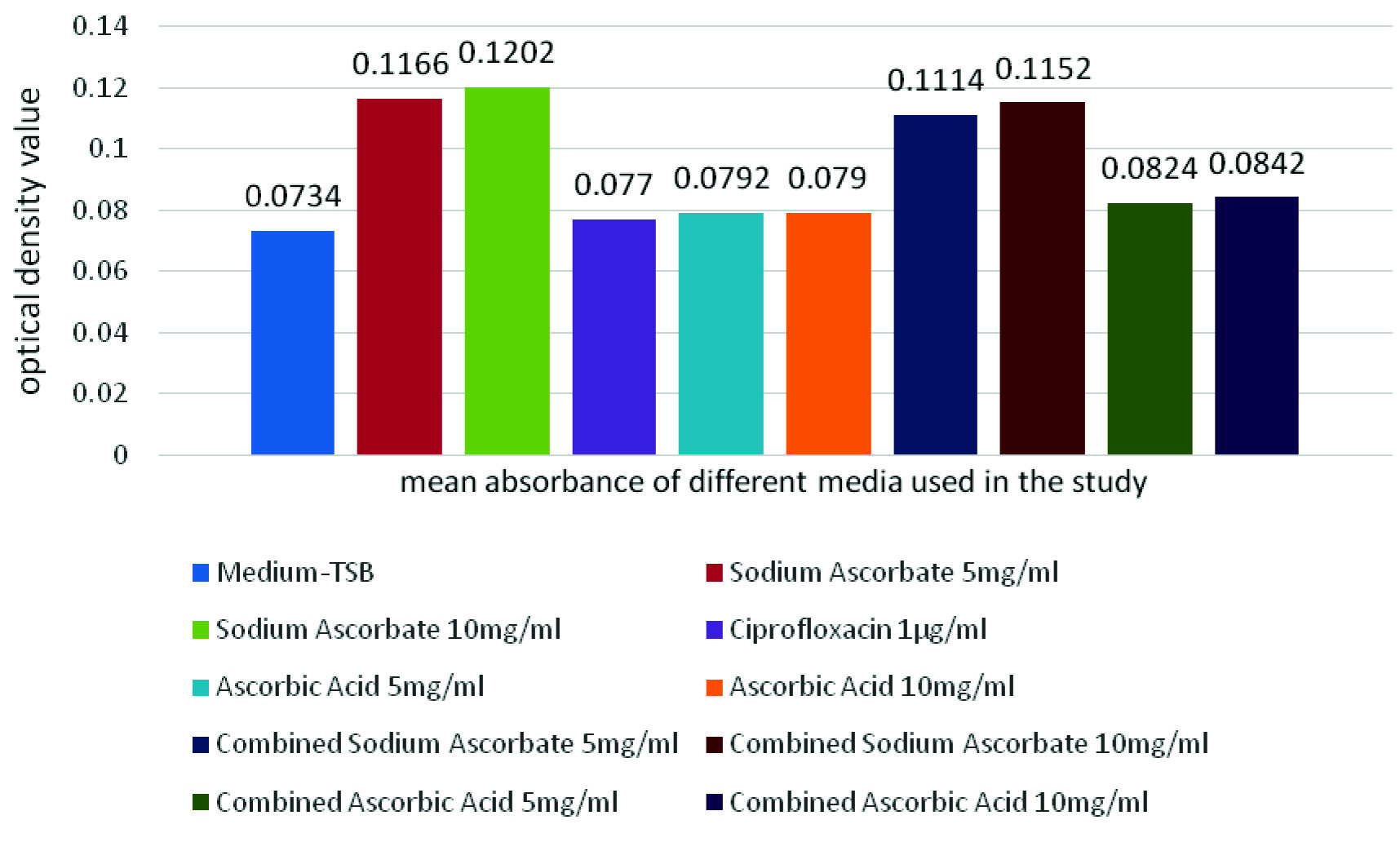
Out of the 50 isolates, 19 were sensitive to ciprofloxacin and 31 were resistant to ciprofloxacin [Table/Fig-1]. Sodium ascorbate significantly increased (p<0.001) the absorbance of the medium, at all concentrations and combinations. This increase was maximum in the tubes containing sodium ascorbate alone at 10 mg/mL. Ascorbic acid [Mean difference-0.0056, Standard error-0.0057 (p=0.992)] and ciprofloxacin (p=1.000) caused no significant change in the absorbance of the medium [Table/Fig-2].
Distribution of E. coli isolates, from urine samples, showing susceptibility to ciprofloxacin.
Comparison of mean absorbance of the media used as base in the study.
There was no significant difference in the absorbance between the two groups except for the ciprofloxacin (p<0.001) and the combinations of ciprofloxacin and sodium ascorbate (p<0.001) [Table/Fig-3].
Group comparison of various media on mean absorbance values.
| Group comparison | Mean | StandardDeviation | p-value (<0.05=significant) |
|---|
| Bacteria control* | Sensitive Isolates | 0.266211 | 0.0403424 | 0.357 |
| Resistant Isolates | 0.281613 | 0.0647928 |
| Sodium ascorbate 5 mg/mL | Sensitive Isolates | 0.275263 | 0.0508296 | 0.514 |
| Resistant Isolates | 0.287742 | 0.0723450 |
| Sodium ascorbate 10 mg/mL | Sensitive Isolates | 0.276105 | 0.0474785 | 0.644 |
| Resistant Isolates | 0.284000 | 0.0639380 |
| Ciprofloxacin 1 μg/mL | Sensitive Isolates | 0.157632 | 0.0938818 | <0.001 |
| Resistant Isolates | 0.280484 | 0.0648598 |
| Ascorbic acid 5 mg/mL | Sensitive Isolates | 0.087316 | 0.0136709 | 0.138 |
| Resistant Isolates | 0.081323 | 0.0136000 |
| Ascorbic acid 10 mg/mL | Sensitive Isolates | 0.075105 | 0.0071949 | 0.557 |
| Resistant Isolates | 0.076581 | 0.0092836 |
| Combined sodium ascorbate 5 mg/mL | Sensitive Isolates | 0.183000 | 0.0939876 | <0.001 |
| Resistant Isolates | 0.287645 | 0.0487391 |
| Combined sodium ascorbate 10 mg/mL | Sensitive Isolates | 0.190105 | 0.0885788 | <0.001 |
| Resistant Isolates | 0.292419 | 0.0589479 |
| Combined ascorbic acid 5 mg/mL | Sensitive Isolates | 0.080526 | 0.0114182 | 0.641 |
| Resistant Isolates | 0.083129 | 0.0223990 |
| Combined ascorbic acid 10 mg/mL | Sensitive Isolates | 0.082263 | 0.0102298 | 0.662 |
| Resistant Isolates | 0.085194 | 0.0277698 |
*E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
Unpaired t-test was used to compare the mean absorbance values of sensitive and resistant isolates, at different concentration of vitamin C, ciprofloxacin, and combinations of both (sensitive isolates-19, resistant isolates 31)
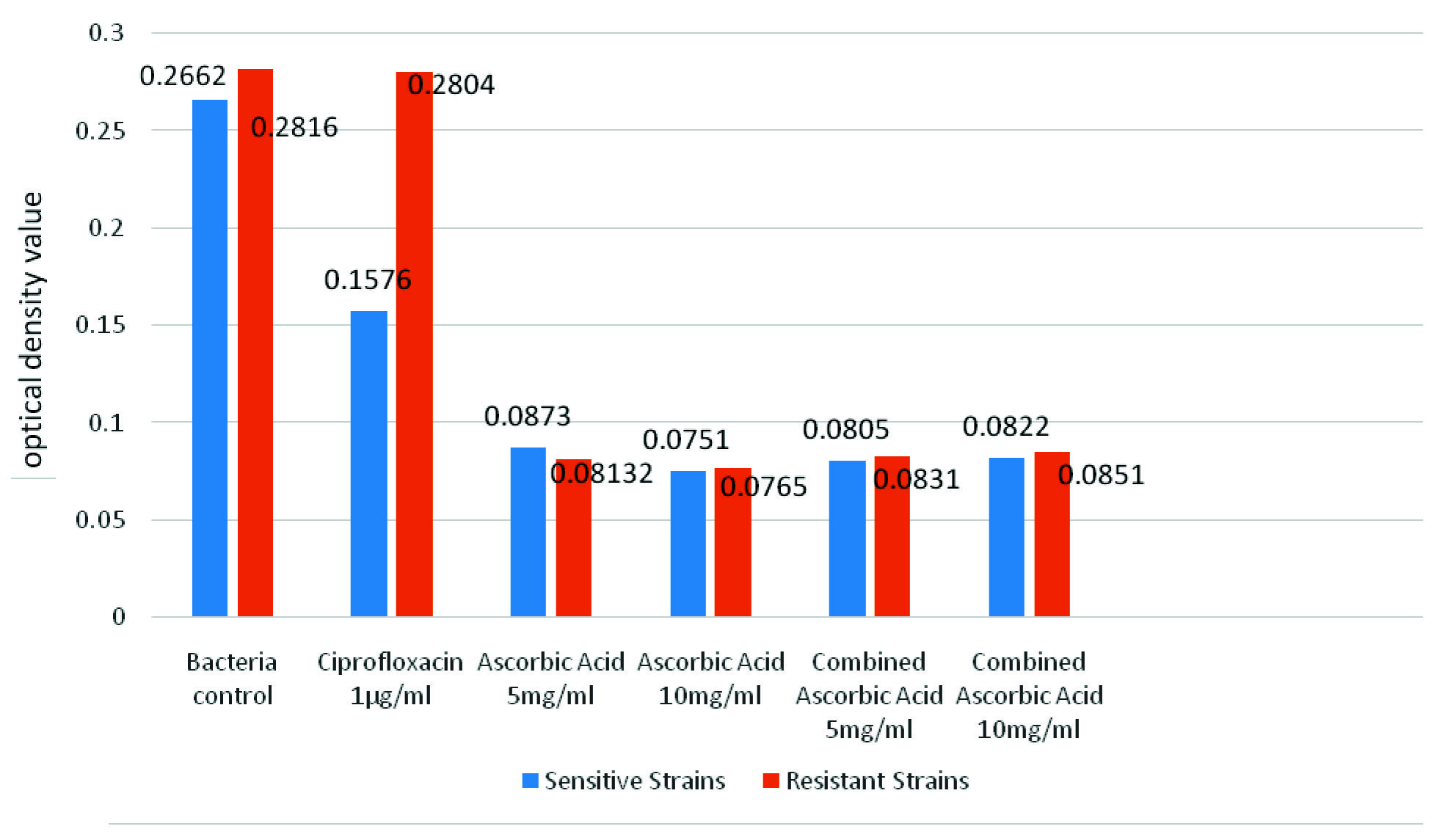
In ciprofloxacin sensitive isolates, there was a significant decrease in the absorbance in isolates with ciprofloxacin (p<0.001), ascorbic acid (5 mg/mL and 10 mg/mL) (p<0.001) and the combinations of ciprofloxacin with ascorbic acid (p<0.001), as compared to the bacteria control. These absorbance values of the isolates with ascorbic acid were significantly lower than the absorbance values for ciprofloxacin alone (p<0.001) [Table/Fig-4,5]. The lowest absorbance values were noted in the tubes containing ascorbic acid at a concentration of 10 mg/mL. However, there was no significant difference between the absorbance of ascorbic acid at 10 mg/mL, as compared to ascorbic acid at 5 mg/mL [Mean difference-0.0122, (p=0.950)] or the combinations of ciprofloxacin and ascorbic acid (5 mg/mL and 10 mg/mL) [Mean difference-0.0054, (p=0.999) and Mean difference-0.0071, (p=0.995) respectively]. E. coli ATCC® 25922™ was tested and absorbance values were same as sensitive isolates.
Mean absorbance of sensitive and resistant isolates measured at 450 nm.
Mean absorbance of sensitive isolates containing ascorbic acid at different concentrations and combinations.
| Variable 1 | Variable 2 | Mean difference(Variable 1-Variable 2) | p-value(<0.05=significant) |
|---|
| Bacteria control* | Ciprofloxacin 1 μg/mL | 0.1085789* | <0.001 |
| Ascorbic acid 5 mg/mL | 0.1788947* | <0.001 |
| Ascorbic acid 10 mg/mL | 0.1911053* | <0.001 |
| Combined ascorbic acid 5 mg/mL | 0.1856842* | <0.001 |
| Combined ascorbic acid 10 mg/mL | 0.1839474* | <0.001 |
ANOVA test was used to compare the mean absorbance values of bacterial control with variables for isolates sensitive to ciprofloxacin
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control
In the resistant isolates, only the isolates containing ascorbic acid (5 mg/mL, 10 mg/mL) showed a significant decrease (p<0.001, p<0.001) in absorbance as compared to the bacteria control [Table/Fig-4,6]. The lowest absorbance values were noted in the tubes containing ascorbic acid alone at 10 mg/mL. However, there was no significant difference between the absorbance of ascorbic acid at 10 mg/mL, as compared to ascorbic acid at 5 mg/mL (p=0.997) or the combinations of ciprofloxacin and ascorbic acid (5 mg/mL and 10 mg/mL) (p=0.988, p=0.961).
Mean absorbance of resistant isolates containing ascorbic acid at different concentrations and combinations.
| Variable 1 | Variable 2 | Mean Difference(Variable 1-Variable 2) | p-value(<0.05=significant) |
|---|
| Bacteria control* | Ciprofloxacin 1 μg/mL | 0.0011290 | 1.000 |
| Ascorbic acid 5 mg/mL | 0.2002903* | <0.001 |
| Ascorbic acid 10 mg/mL | 0.2050323* | <0.001 |
| Combined ascorbic acid 5 mg/mL | 0.1984839* | <0.001 |
| Combined ascorbic acid 10 mg/mL | 0.1964194* | <0.001 |
ANOVA test was used to compare the mean absorbance values of bacterial control with variables for isolates resistant to ciprofloxacin.
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
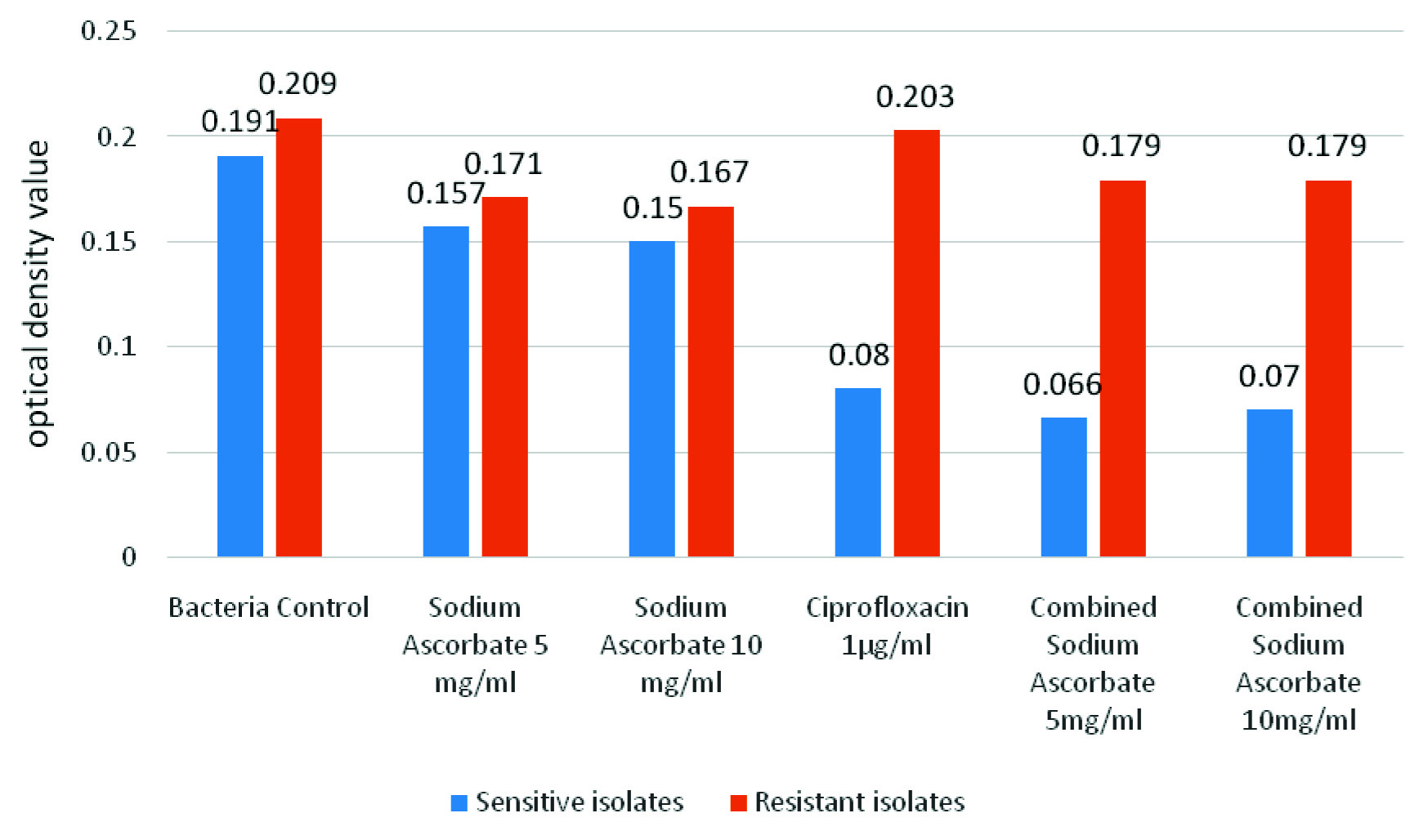
Sodium ascorbate significantly increased the absorbance of the medium, at all concentrations and combinations; hence, corrected absorbance was calculated. In the sensitive isolates, there is a slight decrease in the absorbance in the sodium ascorbate (5 mg/mL, 10 mg/mL) supplemented isolates. However, this decrease was not statistically significant (p=0.728 and p=0.529, respectively). There was a significant decrease in absorbance in the isolates containing combination of sodium ascorbate (5 mg/mL, 10 mg/mL) with ciprofloxacin, as compared to the bacteria control (p<0.001, for both) [Table/Fig-7,8]. In the resistant isolates, there was no significant difference between any of the isolates [Table/Fig-7,9]. There was no synergy between vitamin C and ciprofloxacin [Table/Fig-10].
Corrected mean absorbance of sensitive and resistant isolates measured at 450 nm.
Corrected mean absorbance of sensitive isolates containing sodium ascorbate at different concentrations and combinations.
| Variable 1 | Variable 2 | Mean difference(Variable 1 – Variable 2) | p-value(<0.05=significant) |
|---|
| Bacteria control* | Sodium ascorbate 5 mg/mL | 0.0332105 | 0.728 |
| Sodium ascorbate 10 mg/mL | 0.0405789 | 0.529 |
| Ciprofloxacin 1 μg/mL | 0.1105789* | <0.001 |
| Combined sodium ascorbate 5 mg/mL | 0.1241579* | <0.001 |
| Combined sodium ascorbate 10 mg/mL | 0.1203158* | <0.001 |
ANOVA test was used to compare the corrected mean absorbance of sensitive isolates containing sodium ascorbate at different concentrations and combination.
Corrected absorbance = absorbance of isolate – absorbance of respective control
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
Corrected mean absorbance of resistant isolates containing sodium ascorbate at different concentrations and combinations.
| Variable 1 | Variable 2 | Mean Difference(Variable 1- Variable 2) | p-value (<0.05=significant) |
|---|
| Bacteria control* | Sodium ascorbate 5 mg/mL | 0.0376452 | 0.197 |
| Sodium ascorbate 10 mg/mL | 0.0421613 | 0.107 |
| Ciprofloxacin 1 μg/mL | 0.0057097 | 0.999 |
| Combined sodium ascorbate 5 mg/mL | 0.0301613 | 0.438 |
| Combined sodium ascorbate 10 mg/mL | 0.0295161 | 0.463 |
ANOVA test was used to compare the corrected mean absorbance of resistant isolates containing sodium ascorbate at different concentrations and combination.
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
Study of synergistic action between ciprofloxacin and vitamin C.
| Variables | Mean | p-value(<0.05=significant) | 95% CI |
|---|
| Ascorbic acid | 0.0873 | 0.1053 | 0.01508 to 0.001498 |
| Ciprofloxacin + Ascorbic acid 5 mg/mL | 0.0805 |
Unpaired t-test was used to analyse the synergy between ciprofloxacin and vitamin C.
Discussion
Multidrug resistant bacteria have become a major cause for concern, and there has been limited success in the search for new antibiotics [1]. Therefore, there is need to find new adjuvant to treat bacterial infection. Earlier data which has been submitted for publication (in press) had shown that vitamin C is one such promising adjuvant. In this study, the inhibitory effect of two formulations of vitamin C on the growth of urinary isolates of E. coli was analysed.
Analysis of the absorbance of the controls revealed that ciprofloxacin and ascorbic acid did not significantly alter the absorbance of the medium, sodium ascorbate significantly increased it. This increase in the absorbance is probably due to the chemical properties of sodium ascorbate and requires further investigation. Due to this difference in the absorbance of the controls, the analysis for sodium ascorbate was done separately.
The results show that the absorbance at 450 nm of the bacterial broths containing ascorbic acid was less than the control broths, both in ciprofloxacin resistant and sensitive isolates and the difference was statistically significant. This fall in the absorbance values implies that bacterial dry weight decreased with the addition of ascorbic acid. This showed that ascorbic acid inhibited the growth of E. coli. Gupta GC and Guha BC demonstrated an inhibitory effect of vitamin C on Staphylococcus aureus and Corynebacterium diphtheriae at a concentration of 1/50,000; fungi such as Aspergillus niger and A. flavus were inhibited at a higher concentration of 1/10,000 [6].
In present study, a fall in the absorbance of the solutions as the vitamin C concentration was increased from 5 mg/mL to 10 mg/mL was observed. However, this fall was not statistically significant. When the absorbance was compared to the controls containing ascorbic acid, there was no significant difference. This implies that the dry weight of the bacteria in the broths containing vitamin C was almost zero. It was inferred that the antibacterial action of ascorbic acid on E. coli is maximal at a concentration of 5 mg/mL. Isela SN et al., studied the effect of vitamin C on oral bacteria such as Streptococcus mutans, Staphylococcus aureus and Enterococcus faecalis [5]. They observed a concentration-dependant fall in the absorbance for all bacterial solutions, with a maximal effect at 20 mg/mL vitamin C. They also observed a reduction in the number of bacterial cells by as much as 90% at 20 mg/mL vitamin C, as compared to the controls [5].
It must also be mentioned that the inhibitory effect of Ascorbic acid was independent of the ciprofloxacin susceptibility pattern of the organisms, as ascorbic acid inhibited both sensitive and resistant isolates.
On the other hand, sodium ascorbate did not cause significant decrease in the absorbance of the broths as compared to the bacteria control. Combination of sodium ascorbate with ciprofloxacin caused a significant decrease in the absorbance for the sensitive isolates but not for the resistant isolates. Furthermore, there was no significant difference between the absorbance for the broths with ciprofloxacin alone and the combination with sodium ascorbate. These two points indicate that the inhibitory effect on bacterial growth in the combination of sodium ascorbate with ciprofloxacin is probably due to the sole action of ciprofloxacin and sodium ascorbate caused no significant inhibition on its own. Future studies, can use other methodology such as quantitative culture to study the antibacterial activity of sodium ascorbate.
Studies by El-Gebaly E et al., and Biswas S et al., have demonstrated a synergistic activity between vitamin C and antibiotics such as azithromycin and levofloxacin, respectively [9,15]. This synergistic action has been attributed to presence of antioxidants, flavonoids and phenolics in vitamin C. El-Gebaly E et al., demonstrated that vitamin C inhibited bacterial biofilm formation on the surface of urethral catheters [9]. In our study, we noted that there was no significant decrease in absorbance in the combinations of ascorbic acid as compared to ascorbic acid alone. This could be due to the fact that ascorbic acid alone inhibited all bacteria at a concentration of 5 mg/mL. Future studies can use lower concentrations of ascorbic acid, to study synergistic activity with ciprofloxacin.
Further studies need to be carried out to determine the optimal concentration of vitamin C needed for its inhibitory activity. Moreover, it needs to be determined whether these concentrations can be achieved and sustained in vivo. Stein HB et al., observed that vitamin C at a dose of 8 gm/day orally precipitated uricosuria in one of the volunteers [16]. A few case reports suggest that unusually high intake of vitamin C, especially when administered intravenously may be associated with the development of oxalate kidney stones [17]. However, Creagan ET et al., observed that vitamin C in doses of up to 10 gm/day orally can be given in most patients with no toxicity [18]. A prospective study could not find any association between a high daily intake of vitamin C and the risk of renal stone formation [19].
Limitation
Sample size was small to support the hypothesis due to short study duration of the Indian Council of Medical Research (ICMR), Short Term Student (STS) fellowship study period. The other parameters like Extended-Spectrum Beta-Lactamase (ESBL) production and Minimum Inhibitory Concentration (MIC) of ciprofloxacin was not possible.
Conclusion
This study demonstrates that combination of ciprofloxacin with sodium ascorbate, showed significant inhibition against sensitive isolates, but no such inhibition against resistant isolates. Vitamin C in the form of sodium ascorbate, showed no significant inhibitory effect on the growth of E. coli. Ascorbic acid on the other hand, showed significant inhibition. This study highlights a possible role of ascorbic acid as an adjuvant to antibiotic therapy in UTI. However, further time kill studies are required with various concentrations to determine the bacteriostatic, bactericidal activity, as well as pharmacokinetic and pharmacodynamics studies to understand the role of vitamin C as an antibacterial substance alone or in conjunction with other antibiotics.
Financial support: This ICMR STS [Reference ID-2016-00922] fellowship project was funded by the council.
*E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
Unpaired t-test was used to compare the mean absorbance values of sensitive and resistant isolates, at different concentration of vitamin C, ciprofloxacin, and combinations of both (sensitive isolates-19, resistant isolates 31)
ANOVA test was used to compare the mean absorbance values of bacterial control with variables for isolates sensitive to ciprofloxacin
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control
ANOVA test was used to compare the mean absorbance values of bacterial control with variables for isolates resistant to ciprofloxacin.
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
ANOVA test was used to compare the corrected mean absorbance of sensitive isolates containing sodium ascorbate at different concentrations and combination.
Corrected absorbance = absorbance of isolate – absorbance of respective control
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
ANOVA test was used to compare the corrected mean absorbance of resistant isolates containing sodium ascorbate at different concentrations and combination.
* E. coli (clinical isolates) in TSB without any form of vitamin C or ciprofloxacin was used as a bacterial control.
Unpaired t-test was used to analyse the synergy between ciprofloxacin and vitamin C.