Osteochondrolipoma – A Rare Entity at a Rare Site
Manjula Jain1, Shivali Sehgal2
1 Director Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
2 Assistant Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shivali Sehgal, Assistant Professor, Department of Pathology, Lady Hardinge Medical College, New Delhi-110001, India.
E-mail: shivalisehgal@gmail.com
Osteochondrolipoma is an extremely rare histological variant of lipoma with most reported cases in the head and neck area and the upper half of the body. We report a case of osteochondrolipoma occurring in the right distal fibula of an 11-year-old female. The physical examination revealed a painless, firm swelling over the right ankle joint with no history of trauma preceding it. Histologically, the tumour showed the presence of sheets of mature adipose tissue admixed with mature bony trabeculae. Also, seen in between were the foci of cartilage, proliferating fibroblasts, numerous blood vessels with the evidence of endochondral ossification favouring the diagnosis of osteochondrolipoma. Considering its rare site, the clinicians and pathologists should regard osteochondrolipoma as a possible diagnosis for a well-defined, calcified/ossified mass in the lower half of the body.
Endochondral, Fibula, Lipoma, Variant
Case Report
An 11-year-old female presented with swelling in the distal part of the right leg of six months duration. There was a history of gradual increase in size of the swelling and no history of any preceding trauma. Clinical examination revealed a painless, firm, non-fluctuant swelling measuring 8 cm × 6 cm. Computed tomography showed a bony mass along the lateral aspect of the distal fibula. Excision was planned and per operatively the mass was seen in the soft tissue with no communication with the fibula.
A well circumscribed mass measuring 7 cm × 5 cm × 3 cm was received. The cut surface was predominantly yellow and soft to firm with focal grey white areas which were hard [Table/Fig-1].
Gross photograph showing cut section of a well circumscribed mass which is yellow with focal grey white areas.

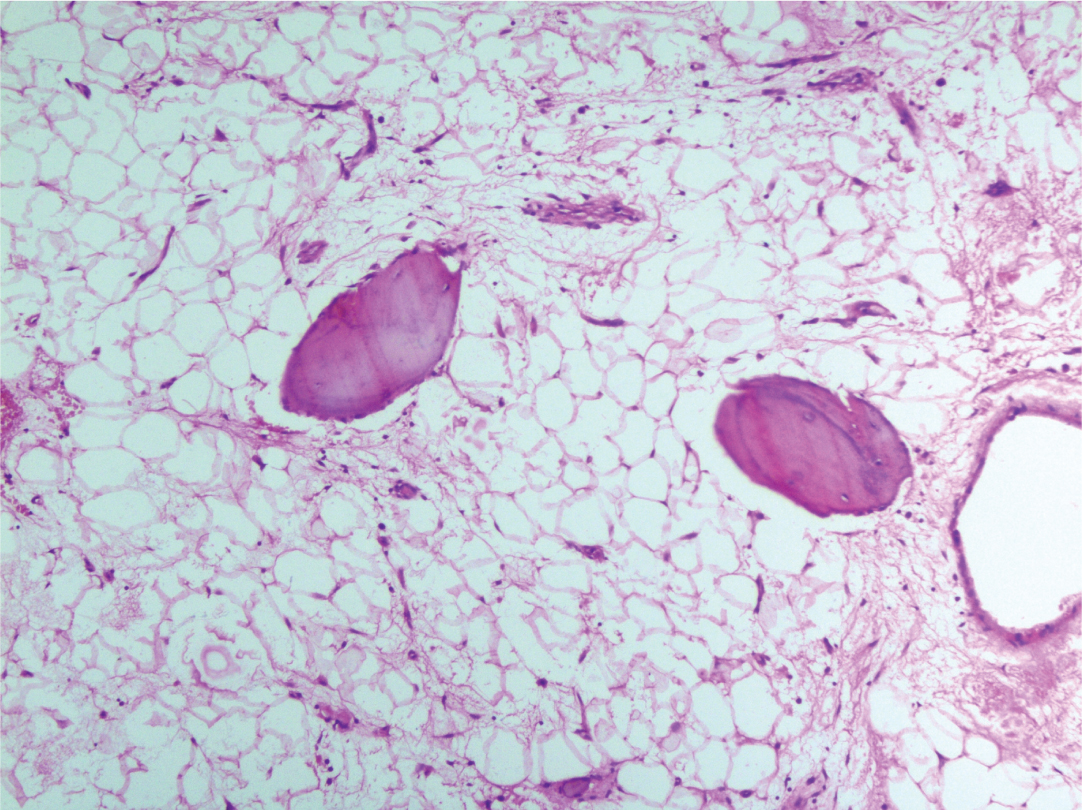
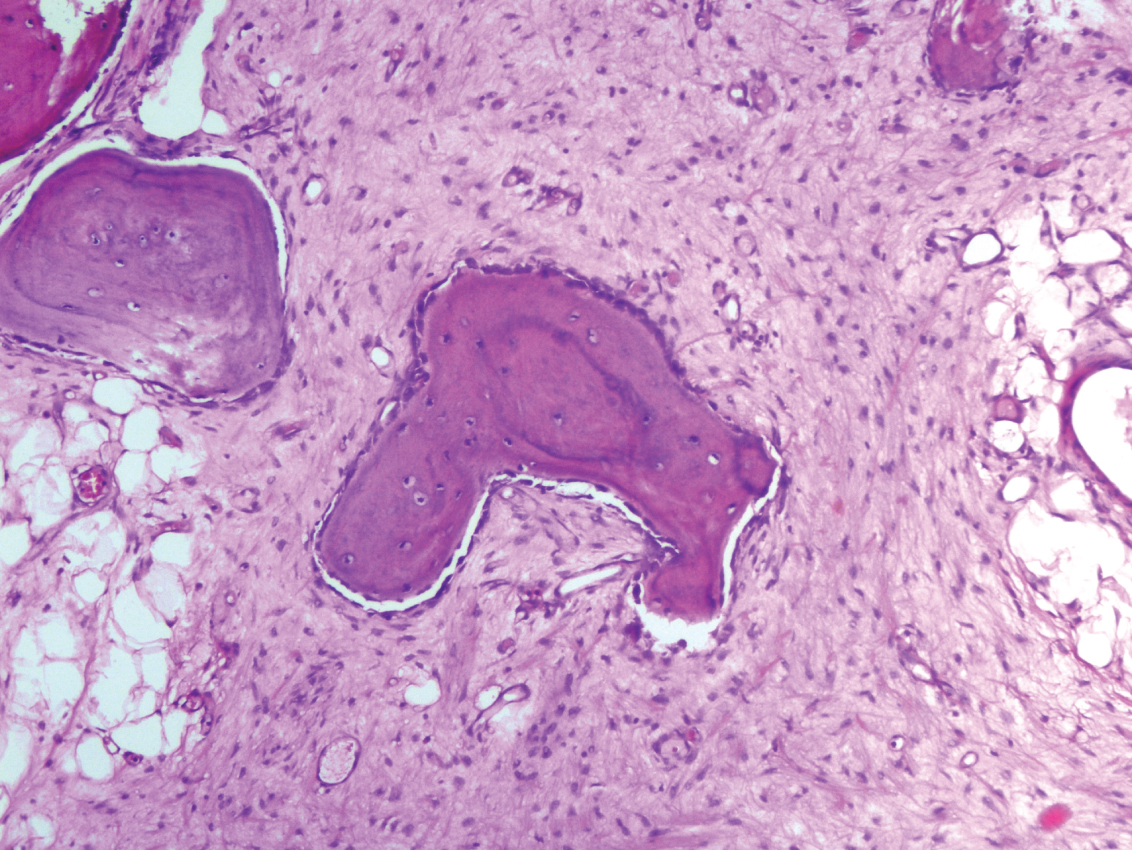
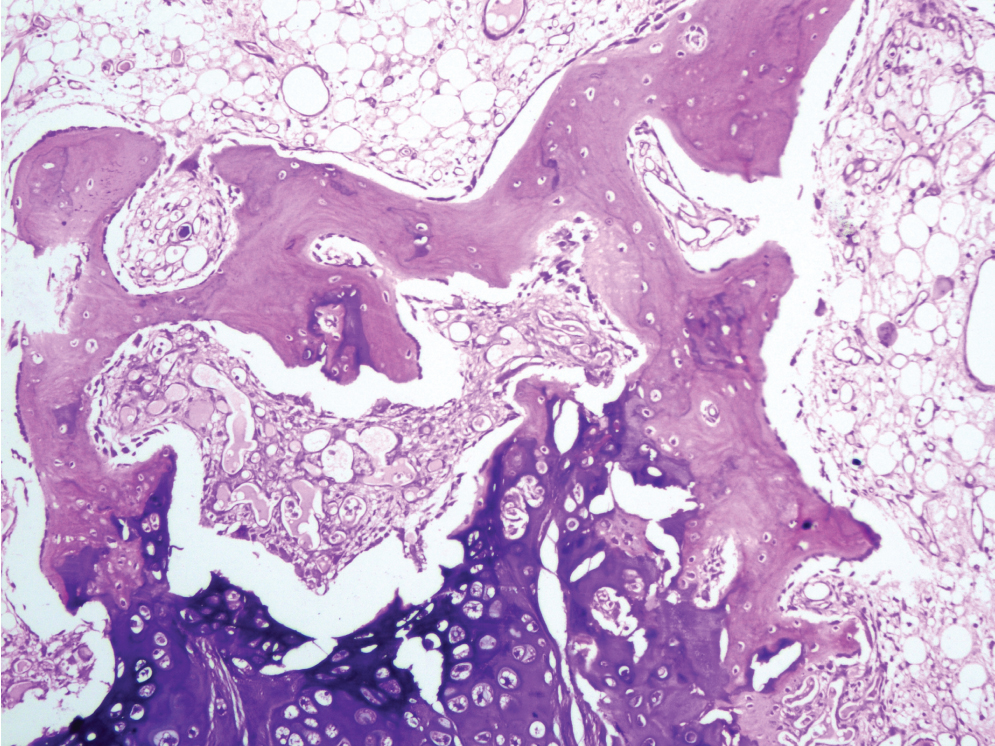
Histopathological examination revealed an encapsulated lesion comprising of lobules of mature adipose tissue with interspersed bony trabeculae [Table/Fig-2]. The bony trabeculae showed osteoblastic rimming [Table/Fig-3]. Also, seen in between were foci of mature hyaline cartilage and enchondral ossification [Table/Fig-4]. There was no haematopoietic tissue, cartilaginous cap, evidence of zonation, cellular atypia or mitotic figures, fibromyxoid areas ruling out mesenchymal hamartoma, osteochondroma, myositis ossificans, well differentiated liposarcoma and ossifying fibromyxoid tumour respectively. A final diagnosis of osteochondrolipoma was made.
Sheets of mature adipose tissue with interspersed bony trabeculae. (H&E, 10X)
Bony trabeculae showing osteoblastic rimming. (H&E, 40X)
Foci of mature hyaline cartilage and endochondral ossification. (H&E, 40x)
The postoperative course was uneventful and subsequently the patient was lost to follow up.
Discussion
Osteochondrolipoma is a variant of lipoma which shows an osseous and cartilaginous differentiation. It is a benign lesion; therefore, there is absence of atypia, increased mitotic activity and lipoblasts. Most of the cases have been reported in the head and neck region and the upper half of the body [1]. Its occurrence in lower half of the body is extremely rare. Very few cases of osteochondrolipoma have been reported, with none described in the distal leg region.
The term “osteochondrolipoma” was coined by Rau T et al., [2]. It is a lipoma with osseous and cartilaginous component and is extremely rare. The adipose, cartilage and osseous tissue components of the tumour may originate from multipotent undifferentiated mesenchymal cells. Secondary cartilaginous and osseous metaplasia in a preexisting lipoma is also a probable cause [3].
Most of the cases have been described in upper part of the body. Soulard R et al., reported a case in the submandibular region which also showed presence of bone marrow elements [1]. A rare case of lipoma with osseous and cartilaginous metaplasia has been reported in the tongue [4]. Gru AA et al., reported an osteochondrolipoma in the subcutaneous region of the chest wall in a young individual [5]. Nishio J et al., reported a case in the scapular region in a 49-year-old male [3].
Osteochondrolipoma has been rarely reported in the lower half of the body. Rau T et al., reported a case located in the thigh in the parosteal area [2]. To the best of our knowledge, osteochondrolipoma has never been reported in the distal leg region. We report this case due to its rare occurrence and at a rare site.
Osteochondrolipoma has the same prognosis as a simple lipoma [3]. Treatment of choice for an osteochondrolipoma is complete surgical excision. Recurrences have not been reported [4].
Conclusion
Considering its a rare site, the clinicians and pathologists should regard osteochondrolipoma as a possible diagnosis for a well-defined mass with ossification, in the lower half of the body.
[1]. Soulard R, Nguyen AT, Souraud JB, Oddon PA, Fouet B, Cathelinaud O, Osteochondrolipoma of the submandibular region: a case report and review of literatureHead and Neck Pathology 2012 6(4):486-91. [Google Scholar]
[2]. Rau T, Soeder S, Olk A, Aigner T, Parosteal lipoma of the thigh with cartilaginous and osseous differentiation: an osteochondrolipomaAnn Diagn Pathol 2006 10(5):279-82. [Google Scholar]
[3]. Nishio J, Ideta S, Iwasaki H, Naito M, Scapular osteochondrolipoma: Imaging features with pathological correlationOncol Lett 2013 6(3):817-20. [Google Scholar]
[4]. Tasie D, Pavlovic M, Stankovie D, Dimov I, Stanojevie G, Dimov D, Ossifying chondrolipoma of the tongueVojnosanit Pregl 2012 69(11):1009-12. [Google Scholar]
[5]. Gru AA, Santa-Cruz DJ, Osteochondrolipoma: a subcutaneous lipoma with chondroid and bone differentiation of the chest wallJ Cutan Pathol 2012 39(4):461-63. [Google Scholar]