The reproductive system, its function, dysfunction and disease plays a central role in women’s health [1]. Globally, World Health Organization (WHO) estimates that the reproductive ill health accounts for 33% of the total disease burden in women and also reports the global prevalence of UP as 2–20% among women younger than 45 years of age [2].
Uterine Prolapse is the main contributor to reproductive health problem that influences the women’s quality of life [3]. In the process of pregnancy and labour women are subjected to a lot of stress and strain, where in their pelvic floor muscles and the structure of perineum loses its tone and may result in Utero-vaginal Prolapse [4]. It is one of the most frequent causes of gynaecological morbidities among women in India and one of the main indications for hysterectomy [5]. So, care is essential, both in the prevention and detection of prolapse. The preventive measures of UP include adequate antenatal, intranatal and postnatal care (Kegal exercises, rest, early ambulation after delivery, personal hygiene, birth spacing, maintenance of balanced diet etc) and general measures such as avoid strenuous activities, avoid weight gain, quit smoking. The nurse can assist in preventing uterine prolapse by (a) encouraging pregnant to seek qualified obstetric care, (b) teaching patients after delivery to alternatively tense and relax their gluteal muscles and the muscles of the pelvic floor. Conservative management approaches such as giving lifestyle advice and delivering pelvic floor muscle training are often used in cases of mild prolapse. However, if UP disrupts the normal life then it might got benefit from treatment options which include using a supportive device (pessary) or surgery to repair the prolapse [6-8], An extensive information about preventive measures of UP during pregnancy and delivery should be the first step to reduce this significant social and public health problem or issue.
Uterine Prolapse has not received sufficient attention despite its high prevalence. So, the reproductive health of a women has to be taken care at right time, thus the impending complications can be prevented. It is one’s responsibility to maintain reproductive health by increasing knowledge on mothers regarding UP and its prevention by giving proper health education, especially during the beginning of motherhood. Therefore, the present study was conducted with an aim to evaluate the effectiveness of STP on knowledge regarding preventive measures of UP among mothers and to find out the association between knowledge of mothers regarding preventive measures of UP and selected demographic variables.
Materials and Methods
A quantitative research approach with pre-experimental one group pre-test post-test design was used for the study [9]. The setting of the study was Gynaecology Out Patients Department (OPD) at AIMS, Kochi. By using non-probability convenience sampling technique, 40 antenatal mothers were selected. The inclusion criteria for the study were antenatal mothers on 36-38 completed gestational weeks and above, mothers with the age group of 18-35 years. Mothers who are mentally ill were excluded from the study.
Sample Size
Considering 95% Confidence Interval (CI), and 20% allowable error, the required sample size was calculated to include 27 respondents. However, researcher decided to include 40 mothers.
Sample size = (Z1-α/22 SD2)÷d2
Z1-α/2- Standard normal variate (at 5% type 1 error (p<0.05) it is 1.96 and at 1% type 1 error (p<0.01) it is 2.58). As in majority of the studies p-values are considered significant below 0.05 hence, 1.96 is used in formula.
SD=Standard deviation of variable. Value of Standard deviation can be taken from previously done study.
d=absolute error or precision.
The research proposal was presented in the Research Committee of Amrita College of Nursing and Thesis Review Committee of Amrita Institute of Medical Sciences and Ethical Committee clearance was obtained. Permission was obtained from HOD of Obstetrics and Gynaecology Department, AIMS, before data collection. The data was collected from December 2016 to January 2017. The antenatal mothers were identified from the OPD during their consultation (Six days per week) and allocated by convenience sampling method as per inclusion criteria. A detailed explanation of the nature and purpose of the study has been given and informed consent was obtained from the participants and explained about post-test on the 14th day to find out the effectiveness of STP and freedom was provided to withdraw from the study at anytime if they want. Since it was an educational intervention study minimum two weeks (14th days) interval must be needed between pre-test and post-test. To follow this formality, the researcher conducted Post-test after 14th day.
Data Collection Instrument and Technique
Tool for socio-demographic and clinical variables including age, age at marriage, educational status, occupation, place of residence, source of information, parity, number of children, age at first childbirth, mode of previous delivery, comorbidities, family history of pelvic organ prolapse and contraceptive use. The semi-structured questionnaire has 26 multiple choice questions on areas like causes (four questions), signs and symptoms (two questions) and preventive measures of uterine prolapse (20 questions). Each correct answer carries one mark and the total score is 26. The knowledge level has been arbitrarily divided into three categories based on the scores in the structured questionnaire which includes Poor knowledge: (scores 1–8), Average knowledge: (scores 9–18) and Good knowledge: (scores 19–26).
The tool prepared was validated by nine experts, including three gynaecologists. The reliability of the tool was done using split-half method on ten antenatal mothers and it was found to be reliable, r=0.743.
Intervention: The STP on preventive measures of UP was prepared for 45 minutes session (six days in a week and seven sessions per day) which comprises of teaching about causes and risk factors, signs and symptoms, diagnostic investigations, management and preventive measures of UP. Lecture cum discussion classes was planned using AV aids such as LCD and charts.
Statistical Analysis
The data collected for the study were analysed by appropriate descriptive statistics and inferential statistics. Frequency and percentage was used to analyse the socio-demographic and clinical data and knowledge regarding preventive measures of UP. Paired t-test was used to compare pre and post test knowledge scores. Chi-square test was used to find out the association between selected variable with knowledge scores.
Results
Demographic Data
The data shows that 20 (50%) of the mothers were in the age group of 23-26 years and majority 19 (47.5%) were graduates and above and 27 (67.5%) of them residing in rural area; whereas only four (10%) of the subjects have received previous information regarding preventive measures of UP [Table/Fig-1].
Distribution of subjects based on the socio-demographic variables (n=40).
| Demographic variables | Frequency (f) | Percentage (%) |
| Age in years |
| 18–22 years | 10 | 25 |
| 23–26 years | 20 | 50 |
| 27–30 years | 7 | 17.5 |
| 31-35 years | 3 | 7.5 |
| Age at Marriage |
| 18-22 years | 27 | 67.5 |
| 23-26 years | 8 | 20 |
| 27-30 years | 4 | 10 |
| 31–35 years | 1 | 2.5 |
| Education |
| Primary | 1 | 2.5 |
| High school | 4 | 10 |
| Higher Secondary | 16 | 40 |
| Graduate and above | 19 | 47.5 |
| Occupation |
| Employed | 6 | 15 |
| Unemployed | 34 | 85 |
| Area of residence |
| Rural | 27 | 67.5 |
| Urban | 13 | 32.5 |
| Previous knowledge about preventive measures of UP |
| Yes | 4 | 10 |
| No | 36 | 90 |
Clinical Characteristics
Majority 62.5% of the mothers were primigravida. Among the multigravida mothers, 73% had single child and 53.3% had undergone vaginal delivery with episiotomy. Only four (10%) of the mothers had previous history of any surgery and 5% of them had history of contraceptive use. There were 15 (37.5%) of the mothers having presence of comorbidity during present pregnancy and none of them have family history of pelvic organ prolapse, which was an important data [Table/Fig-2].
Distribution of subjects based on the clinical variables (n=40).
| Clinical Variable | Frequency (f) | Percentage (%) |
|---|
| Parity |
| Primigravida | 25 | 62.5 |
| Multigravida | 15 | 37.5 |
| Number of children |
| No child | 1 | 7 |
| One | 11 | 73 |
| Two | 3 | 20 |
| 1.2 Age at first childbirth |
| 20-25 years | 11 | 74 |
| 26-30 years | 2 | 13 |
| 31–35 years | 2 | 13 |
| 1.3 Mode of delivery |
| Vaginal delivery with episiotomy | 8 | 53.3 |
| Vaginal delivery without episiotomy | 1 | 6.7 |
| Caesarean section | 6 | 40 |
| 1.4 Gap between first and second pregnancy |
| ≤1 year | 1 | 7 |
| 1-2 years | 7 | 46.5 |
| ≥3 years | 7 | 46.5 |
| Previous history of any surgery |
| Yes | 4 | 10 |
| No | 36 | 90 |
| History of contraceptive Use |
| Yes | 2 | 5 |
| No | 38 | 95 |
| Presence of Comorbidity at present pregnancy |
| No | 25 | 62.5 |
| Yes | 15 | 37.5 |
| History of Pelvic Organ Prolapse |
| No | 40 | 100 |
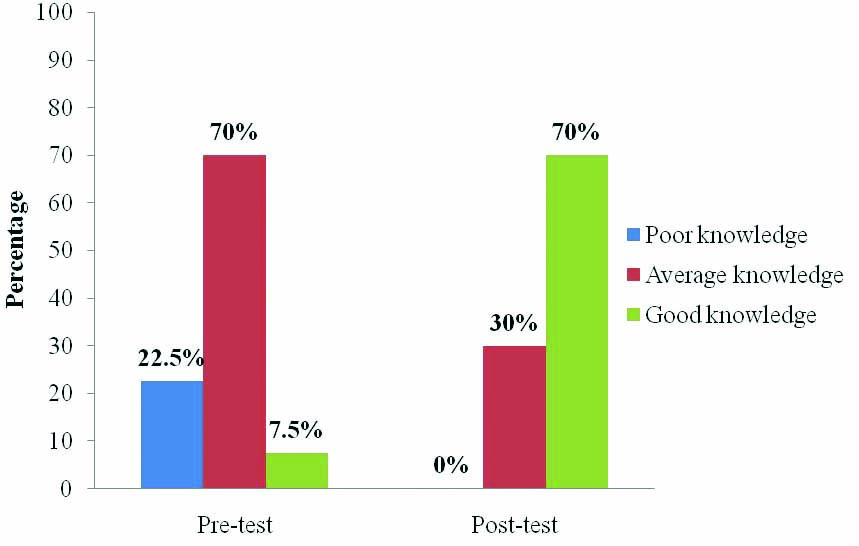
Comparison of the pre-test and post-test knowledge level of the mothers regarding preventive measures of UP: [Table/Fig-3] shows that, in pre-test 28 (70%) subjects had an average knowledge and nine (22.5%) of them had poor knowledge. Only three (7.5%) of the subjects had good level of knowledge regarding preventive measures of Uterine Prolapse. In the Post- test, 28 (70%) of the subjects had good knowledge and 12 (30%) had average knowledge. No one had poor level of knowledge in the post-test.
Comparison of the pre-test and post-test level of knowledge.
Comparison of the pre-test and post-test knowledge score level of the mothers: The mean post-test knowledge score (19.75) was significantly (p<0.001) higher than the mean pre-test score (11.85) [Table/Fig-4]. This shows that the STP was effective in improving the knowledge of mothers regarding preventive measures of UP.
Comparison of the pre-test and post-test knowledge score level of the mothers (n=40).
| Groups | Scores of Knowledge | Df | Paired t-test value | p-value |
|---|
| Mean | SD (±) |
|---|
| Pre-test | 11.85 | 4.36 | 39 | 16.01 | <0.001 |
| Post-test | 19.75 | 2.98 |
t (at α=0.001 at 39 df) =3.55; t (at α=0.05 at 39 df) =2.02
Df=Degrees of Freedom
Association between knowledge of mothers regarding preventive measures of uterine prolapse and selected demographic variables: There was no statistically significant association between pre-test level of knowledge and selected demographic and clinical variables including education, occupation, place of residence, previous information about UP, parity, presence of comorbidity, history of any surgery and contraceptive use except age of the mothers. There was a significant association found between pre-test level of knowledge and age of mothers (χ2=6.307, p=0.043) [Table/Fig-5].
Association between pre-test knowledge level and selected socio-demographic and clinical variables (n=40).
| Variables | Knowledge level | χ2 Value | p-value |
|---|
| Poor | Average | Good |
|---|
| F | % | F | % | F | % |
|---|
| Age |
| ≤ 27 years | 4 | 13.3 | 24 | 80 | 2 | 6.7 | 6.3 | 0.04* |
| > 27 years | 5 | 50 | 4 | 40 | 1 | 10 |
Discussion
The present data illustrates that all the respondents were married after the age of 18 years and had first child birth after the age of 19 years. This result is inconsistent with the national data presented in Nepal Demographic and Health Survey 2011 [10,11].
The results of the present study indicated that the mean pre-test knowledge level of mothers was 11.85±4.36 and the mean post-test knowledge level was 19.75±2.98. Paired t-test was used to compare the mean pre-test and post-test score and t-value was 16.01 and p-value was <0.001 which was statistically significant. Divya et al., conducted a similar study to evaluate the effectiveness of Educational Intervention Package on Utero-Vaginal Prolapse and its prevention among women in chennai. In the pre-test, 50 (83.3%) of women had inadequate knowledge, eight (13.3%) of women had moderately adequate knowledge and two (3.3%) of women had adequate knowledge. In post-test, majority 46 (76.7%) of mothers had adequate knowledge, 14 (23.3%) mothers had moderately adequate knowledge and none of them have inadequate knowledge. The mean pre-test knowledge score was 7.2±2.9 and the mean post-test knowledge score was 9.5±2.8. The paired t-value was 26.3, which was statistically significant at p<0.001 [12].
The results of the present study and supporting study highlighted the positive role of education on preventive measures of UP and interpreted that STP was effective.
In the present study, there was a significant association found between pre-test level of knowledge and age of mothers (χ2=6.307, p=0.043). Study conducted by Shrestha BO et al., also demonstrated that women’s age group was associated with UP knowledge. Satisfactory knowledge about UP was associated with administrative region, ecological zones, caste/ethnic group, and age group of women. Compared with women age <20 years, the odds of having knowledge regarding UP were 0.4 and 0.3 times higher in women aged 20–35 years and >35 years, respectively [13]. The study results are consistent with the similar comparable studies from Nepal, India, Moscow and Vienna [12-16].
Similarly, another study conducted by Lyatoshinskaya P et al., to evaluate the level of knowledge of pelvic organ prolapse and analyse health information-seeking preferences in patients presenting at tertiary referral centres in Vienna and in Moscow. The result shows that, the mean total knowledge scores in patients in Vienna and in Moscow were not significantly different: 9.7±3.5 vs. 9.8±2.9 (p=0.92) and could not find any association between knowledge scores and parameters including age, parity and household income in both groups [17]. However, there was significant association found between pre-test knowledge scores and age of mothers in the present study and this may be due to influence of confounding variables like previous pelvic organ prolapse treatment, pelvic organ prolapse symptom duration.
Limitation
Limitations were randomization was not possible due to time constraints and pre-test was conducted in antenatal period and post-test was in postnatal period.
Strength of the Study
The finding of the study have implications in nursing practice, nursing education, nursing administration and nursing research are the strengths of the study.
Conclusion
The study findings showed that there was a significant improvement in knowledge regarding preventive measures of UP in post-test. The STP was effective and it also suggested that the programme should be continued in order to uplift the overall health and practices of mothers. Hence, it will help to reduce the incidence of UP and enhance the quality of life in future.