The tissue defect has always been a challenge for the reconstructive surgeon, most involving reconstruction of lower third leg and foot defects. There has been a great deal of interest in the use of local tissue to cover lower extremity defects. Skin resurfacing of the exposed soft tissue is essential in preventing complications. The management of lower-extremity trauma has evolved over the last two decades to the point that many extremities that would have required amputation are now routinely salvaged. The goal in lower extremity salvage is to preserve a limb that will be more functional than if it is amputated. An ideal solution for soft tissue coverage should shorten wound healing time, reduce wound complications, provide satisfactory function, minimize morbidity, and, if possible, provide better cosmesis. Closure by secondary intention or by skin grafting may not give good functional results. For deep defects best results are obtained from muscle flaps for dead-space obliteration or a fasciocutaneous flap. A simple method for reconstruction of the lower leg, heel, and foot is the islanded reverse sural artery fasciocutaneous flap supplied by perforators from the medial superficial sural artery [1-7]. It has become popular since, introduced by Donski and Fogdestam [8], followed by the detailed anatomical description by Masquelet AC et al., [2]. Multiple case series reported the reverse sural island fasciocutaneous flap as a reliable solution to a myriad of reconstructive needs, with low complication rate [3-7,9-14]. The reverse sural neurocutaneous flap and lateral supramalleolar flaps were compared in a series by Touam C et al., [15] which inferred sural flap was superior to the lateral supramalleolar flap in reliability: 4.8% failure for the reverse sural flap versus 18.5% for the lateral supramalleolar flap. Both flaps are more useful in non-traumatic wounds, such as after resection of skin cancers or ulcers. The ultimate result of the reconstruction will be to fit into a proper footwear and ambulation.
This study was done to assess the versatility of islanded reverse sural artery flap cover for distal third leg, heel and foot defects since, it is a one stage operation, which does not require microsurgical techniques. Subsequently, however, it was discovered that there existed a vascular axis along the path of the cutaneous nerves of the body [2,4], which allows for elevating an axial flap supplied by the neurovascular axis for coverage of leg wounds. The possibilities of coverage of such defects are few, the flap chosen should be easy to execute quickly with minimal discomfort to the patient, and should provide durable coverage for the defects of the distal third leg, heel and foot.
Materials and Methods
This was a prospective study done between October 2007 and March 2010 at Government Chengalpattu Medical College and Hospital, Tamil Nadu, India. There were a total of 26 patients with moderate sized skin and soft tissue defects in the distal third of leg and foot who were treated in our institute with islanded reverse sural artery flap. The average age of these patients was 37.8 years ranging between 12 to 65 years and all were males. The inclusion criteria were moderate size defects (raw area whose any one dimension was more than 4 cm considered to be moderate defect), defects with exposed or ruptured tendoachilles, diabetics, smokers, hypertensives and fracture lower third leg with intact fibula.
The exclusion criteria were large defects (raw area whose any one dimension is more than 15 cm was considered to be a large defect), major trauma with associated head injury, mangled extremity, fracture of both bones distal third of leg and varicose veins.
In 22 cases, the indication for flap surgery was traumatic defects, of which eight were due to wheel spoke injuries and 14 were due to Road Traffic Accident (RTA). There were three post-burn unstable scar and one post-infective ulcer. Four of the patients had ruptured tendo achilles tendon which was repaired primarily. Closure of the defects was achieved by islanded reverse sural artery flap alone in 21 patients and in combination with an additional skin graft in five patients. The success rate of the flap in our study is 80.7%.
The average dimension of the defect was 5.8x5.1 cm ranging from 4x3 cm to 11x9 cm. The average dimension of skin paddle ranged from 7.1x6.3 cm ranging from 5x4 cm to 12x10 cm. The recipient sites of the defect were over the heel tendo achilles region (18 cases), heel weight bearing area (two cases), medial and dorsal aspect of the ankle joint (four cases), Lateral malleolar region (two cases) with defects that were exposing the bones and tendons in the region.
Of the 26 cases, where the defects were present six had concomitant fracture tibia without fracture fibula. These associated fractures were treated either with external fixator and interlocking nailing. All the flaps in post traumatic cases have been undertaken as delayed primary procedure and the average time gap between injury and flap procedure was 7.5 days (one to 21 days).
Of the 26 patients,14 patients had comorbidities of which six patients had isolated diabetes, three patients with only history of smoking and five cases of combined diabetes and smoking history. Smoking alone was noted in three patients. All comorbid conditions were present for more than five years duration.
After obtaining fitness for surgery, an informed consent for surgery was obtained. Under anaesthesia patient was positioned in lateral decubitus position or prone position. A line was then marked from a point halfway between the achilles tendon and the lateral malleolus at the ankle extending to the midline between the two heads of the gastrocnemius muscle [Table/Fig-1].

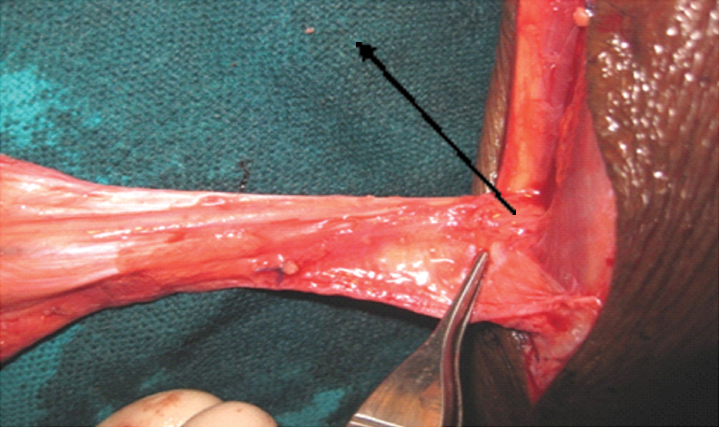
This roughly describes the course of the medial sural cutaneous nerve [5,6]. Following marking the course of the nerve, the peroneal perforators that course through the posterior crural septum were identified. The foot was dorsiflexed, demonstrating the interface between the musculature, lateral compartment, and soleus muscle. The Doppler probe was then used to identify and mark the peroneal perforators. Typically, three to five of these occupy a zone 4 to 13 cm above the tip of the lateral malleolus [9-11]. The pivot point of the pedicle was marked including minimum two perforators marked around 6-7 cm above the lateral mallelous to allow anastomosis with the peroneal artery with the aid of hand held doppler. [Table/Fig-2,3]. The flap was outlined at or below the posterior aspect of junction of upper and middle 1/3rd leg according to the prepared defect pattern of the recipient defect. The defect was excised and perforators were marked. Flap was planned basing the pivot point on the second perforator from lateral malleolus with upper end of flap not extending into proximal third. The required skin island was marked and raised on an adipofascial pedicle to transport the flap to defect. Flap outcome based on pedicle width and arc of rotation was studied.
Perforators from peroneal artery to median sural artery.

Picture showing the intact 7 cm perforator.
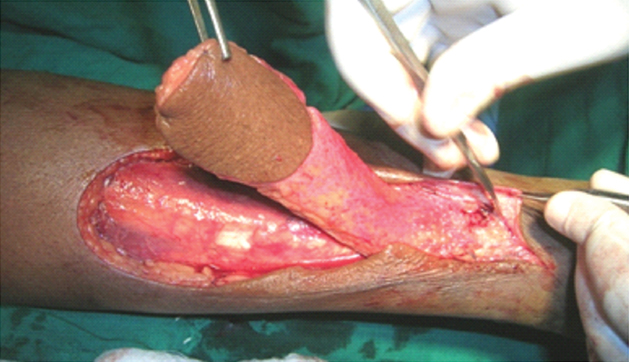
Pedicle width of the flap was kept at 3 cm in first 12 cases and 4 cm in next 14 cases to study the effect of pedicle width [Table/Fig-4].
Skin island raised on a wide adipofacial pedicle.
Flap was elevated up to pivot point and thenrotated from 900-1100 for ankle and lateral malleolar defects, and to 1950 rotation for heel defects. Flap was inset to the defect and donor area and pedicle were resurfaced with Split Skin Graft (SSG) [Table/Fig-5].
Donor area and pedicle resurfaced with SSG.

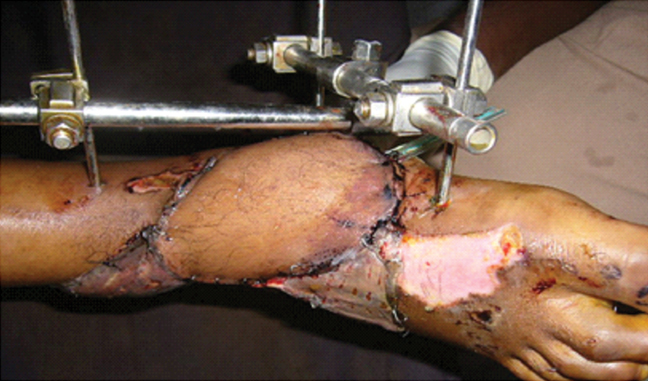
Postoperatively, patients were immobilized with a Plaster of Paris (POP) cast avoiding pressure over heel in 19 patients or utilizing external fixators as in seven patients. Patients were ambulated after six weeks with full weight bearing. A proforma was filled out for each patient to collect data on patient’s demographics, wound and defect properties including its cause, size, site, bone, tendon, or joint exposure, and associated problems such as diabetes, varicose veins, and smoking. Then, in the operating room and during two to 28 months of follow up in the ward and outpatient clinic, the second part of the proforma was completed to record flap characteristics, including the size of the skin paddle, pedicle length and width, site of any previous scar at the donor site, pivot point distance from the lateral malleolus, and complications of donor site.
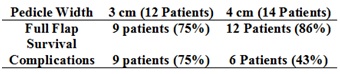
Observations with 3 cm wide adipofacial pedicle: In 12 of the 26 sural artery flaps, the pedicle width was 3 cm. There were four cases of marginal necrosis but survived ultimately. Two flaps had partial necrosis of 2.5 cm which were salvaged secondarily by split skin graft after 7–10 days. Hence, nine out of 12 flaps survived completely with success rate of 75%.
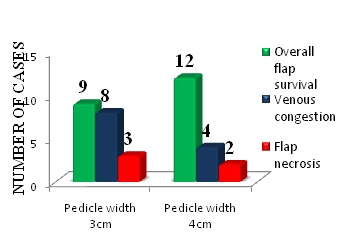
Arc of rotation: In our study, eight (66.6%) of the 3 cm pedicle flaps with arc of rotation of 180° showed venous congestion and three had flap necrosis. Those with venous congestion survived [Table/Fig-6].
Pedicle width and outcome.
Observations with 4 cm wide adipofacial pedicle: In 14 of 26 flaps, the pedicle width was 4 cm. The necrosis rate in this patient group was 14%. Two patients had marginal superficial necrosis which healed by secondary intention. There were two cases of partial necrosis with raw area which was resurfaced with split skin graft. Hence, 12 out of 14 flaps survived completely with success rate of 85.7%.
Arc of rotation: In this group with 4 cm pedicle, the flaps undergoing 180° rotation showed venous congestionin six cases and flap necrosis in two cases. Venous congestion was noted in seven of the flaps in total which resolved on its own with conservative management in five to seven days time. The incidence was eight patients (67%) in 3 cm pedicle width flaps and four patients (22%) with 4 cm pedicle width flaps. Further flaps undergoing 180° rotation used to cover posterior aspect of heel and weight bearing area of heel showed increased incidence of venous congestion. The incidence of venous congestion was less in wider pedicled flaps [Table/Fig-7].
Flap showing venous congestion and marginal necrosis.

Complications: Flap complications were recorded in 10 of 26 cases (38.5%). Marginal superficial necrosis was noted in six cases and partial necrosis occurred in four cases [Table/Fig-8].
Flap showing partial necrosis.

Superficial necrosis was treated conservatively and flap survived completely. In the five cases of necrosis of skin leading to raw area at the flap margins and in two cases of raw area at the pedicle, the same were resurfaced with split skin grafting. All wounds healed completely. Other complications seen were infection in six cases, hematoma in two cases. This occurred more in patients with associated comorbidities.
In patients with diabetes alone there was 50% flap necrosis of which 33% was marginal. Complications were noted even in patients with good glycaemic control. The isolated smokers showed 66% flap necrosis and in patients with combined diabetic and smoking history there were 60% flap necrosis of which 40% were partial flap necrosis needing secondary salvage.
Long term complications: 20 of the 26 patients on long-term follow up for a maximum of 24 months had no complaints. Six of the patients on long-term follow up complained of hyperkeratosis in the flap to heel junction. One patient had ulceration at junction of flap with the sole skin which was managed conservatively with foot care and proper foot wear [Table/Fig-9].
Ulceration at junction of flap.

This was mainly noted in flap used for reconstruction of weight bearing area of heel.
Donor site morbidity: Donor-site grafted areas showed good graft take except in three cases. All patients were advised graft care, kneading and compression garments to avoid adherence of graft to underlying posterior gastrocnemius soleus muscle complex. All patients had good tendo achilles function at the end of three months irrespective of tendo achilles injury. Patients complained of initial impaired sensation in the territory of sural nerve over lateral border of foot which improved over three months time, due to other intact cutaneous nerves of the lower limb. However, no patient in this study developed painful neuroma.
Functional outcome: All the patients had full weight bearing walk at the end of six weeks with normal tendo achilles action. Due to bulkiness of the flap nine of the 26 patients were not comfortable in wearing their usual footwear. They opted for customized footwear. All the patients returned to their previous job after surgery in three months time and carried out activities of daily living.
Results
The results were analyzed based on the hypothesis that certain factors could be identified that influences the complication rate which were age, comorbidity, pedicle width and arc of rotation and tendo achilles action.
Age
The average age of the entire group was 37.8 years (age range, 12 to 65 years). The necrosis rate in each decade of age showed more necrosis in fifth and sixth decade. The necrosis rate was very minimal in second to fourth decade irrespective of comorbid state. Full survival of the flap was seen in 100% of second to fourth decade patients while fifth to seventh decade showed only 50% full flap survival. Since, this study mainly had younger patients success rate was better.
Pedicle Width and Arc of Rotation
An islanded flap with a wider subcutaneous pedicle including additional superficial veins over the pedicle was used in 14 cases. The result was better with pedicle width of 4 cm compared to 3 cm as shown above with better flap survival and less venous congestion. Venous congestion was more in flaps requiring more degree of rotation as for dorsum of foot and heel in both groups but more in 3 cm pedicle flaps [Table/Fig-10,11].
Flap with wider arc of rotation.
Flap survival and complications in the two different pedicle widths tendo achilles.
Of the 26 patients, four patients had ruptured tendo achilles tendon which was primarily repaired and wound was covered with islanded reverse sural artery flap. All the patients recovered well and had normal weight bearing walk at end of six to eight weeks. There was no restriction of movement of tendo achilles due to the graft adherence to the gastrocnemius-soleus muscle complex.
Discussion
Nakajima H et al., [16] proposed three types of pedicledfasciocutaneous flap in the extremities which were veno-adipo-fascial, neuro-adipo-fascial and veno-neuro-adipo-fascial. These flaps were all based on type II vessels. They were arteries accompanying cutaneous nerves and veins that run long in the deep adipofascial layer. The median superficial sural artery, which runs in conjunction with the medial sural cutaneous nerve, and a series of two arteries accompanying the lesser saphenous vein provide the axial pattern blood flow to the suprafascial plexus, subcutaneous vascular plexus, and subdermal plexus, which allows elevation of this flap [4-7]. The median superficial sural artery is located lateral to the medial cutaneous sural nerve and sural nerve, whereas, the lesser saphenous vein is located medially. These axial pattern vessels make a series of interconnections with perforating vessels in the region of the lateral malleolus [9-12].
The sural artery anastomosis with the lateral tarsal artery, which takes origin from the anterior tibial artery. Generally, four to five fasciocutaneous perforators from the peroneal artery travel in the crural septum to supply the skin of the lateral leg. These fasciocutaneous perforators are the vascular supply of the fibula osteocutaneous flap skin island. They also communicate with the axial vessels that accompany the medial sural cutaneous nerve. These vessels typically are located in the posterior crural septum; starting at a point 5 cm above the tip of the lateral malleolus and extending proximally to a distance of approximately 13 cm above the lateral malleolus [9-11]. This anastomoses with peroneal artery are constant. A huge anastamosis is located in the lower part of the tibio fibular space. It gives off the lateral calcaneal artery based on which many types of flaps have been designed for smaller defects. Therefore, a rich plexus of fasciocutaneous and musculocutaneous perforators localized to the lateral aspect of the distal third of the leg that communicate with a series of axial patterned vessels accompanying the sural artery and lesser saphenous vein provide the principal blood supply to the suprafascial plexus, subcutaneous plexus, and subdermal plexus along the posterior calf [13-14]. The vascular axis of the nerve anastomosis with the perforators issued from the deep vessels can be considered as a superficial subcutaneous relay. The islanded reverse sural fasciocutaneous flap should therefore, be designed to incorporate these structures in an effort to maximize local blood flow. The prerequisites for good venous drainage in a reverse-flow arterial flap are the elevation en bloc of the pedicle with its surrounding areolar tissue and the release of the pedicle as far as the superficial vein of return.
The age of the patients ranged in present study was 12–65 years with a mean of 37.8 years. In comparison to previous studies, the present patient population was relatively of younger age. The average age in other studies was 40 [17], 38.9 [18], and 54.1 years [19]. In this study the complications were more seen in older age supported by a larger series done by Baumeister SP et al., [19] [Table/Fig-12].
Association between age and flap necrosis.
| Age group(years) | Flap necrosis rate (in percentage) |
|---|
| Present study | Baumeister SP et al., [19] |
|---|
| <20 | 0 | 50 |
| 21-30 | 0 | 0 |
| 31-40 | 0 | 0 |
| 41-50 | 25 | 45 |
| 51-60 | 40 | 57 |
| 61-70 | 100 | 44 |
In the present study, trauma was the major cause of the defects in 22 (84.6%) patients. Among these 14 patients met with road traffic accidents and eight patients had wheel spoke injuries. This is comparable to other studies in which trauma was described as major etiological factor by 84% by Almeida MF et al., [20], 88% by Fraccalvieri M et al., [21], 64.7% Yilmaz M et al., [7], 71.4% by Rajacic N et al., [22] and 65% by Jeng SF et al., [12]. This is in contrast to the study described by Baumeister SP et al., [19] in which unstable or chronic ulcers were the dominant causative factor in 75% of patients, and pressure sores in 45% cases as described by Touam C et al., [15] [Table/Fig-13].
Comparison of aetiological factors in different studies.
| Aetiological factor | Present study (%) | Almeida MF et al., [20] (%) | Fraccalvieri M et al., [21] (%) | Yilmaz M et al., [7] (%) |
|---|
| RTA | 84.6 | 84 | 88 | 65 |
| Post burn/Unstable scar | 11.5 | 6 | - | - |
| Post infective | 3.9 | 10 | 12 | 12 |
| Others | - | - | - | 24 |
Masquelet AC et al., [2] reported the concept of a neuroskin flap in 1992 and later Yilmaz M et al., [7] modified the technique, but were uncertain as to how large a flap could be elevated successfully. However, Yilmaz M et al., [7] reported that the largest flap used in their series measured 12 cm in width and 15 cm in length. The maximum dimension of the flap in present study was 12x10 cm, which is similar to above and is comparable to other studies reported by Rashid M et al., [17] and Ayyappan T et al., [23] the largest flap was used to cover an extensive heel defect.
The success rate of the islanded reverse sural artery flap in present study was 80.7% with 21 of 26 flaps healed fully without secondary salvage with SSG and five of 26 (19.3%) of the flaps showed marginal or partial necrosis requiring salvage SSG. It is comparable to study described by Rashid M et al., [17] (80.4%) and Akthar S et al., [24] (79%). This rate is higher than the rates reported in larger series by Baumeister SP et al., [19] (64%), Almeida MF et al., [20] (73.6%) and Fraccalvieri M et al., [21] (78%). However, this rate is lower than the rates previously reported by Yilmaz M et al., [7] (88%), Rajacic N et al., [22] (86%), Touam C et al., [15] (94%) [Table/Fig-14].
Success rate compared with various other studies.
| Study | Number of cases | Success rate (%) |
|---|
| Present study | 26 | 80.7 |
| Yilmaz M et al., [7] | 17 | 88 |
| Touam C et al., [15] | 36 | 94 |
| Rashid M et al., [17] | 12 | 81 |
| Baumeister SP et al., [19] | 70 | 64 |
| Almeida MF et al., [20] | 71 | 73.6 |
| Fraccalvieri M et al., [21] | 18 | 78 |
| Rajacic N et al., [22] | 21 | 86 |
| Akhtar S et al., [24] | 84 | 79 |
The higher success rate of the flap in present study is due to the fact that the islanded reverse sural artery flap is used in younger patients with post-traumatic defects who have very less comorbidity.
Having the pedicle width wider at 4 cm in later patients has also reduced the complications like venous congestion and flap necrosis encountered in previous patients with pedicle width of 3 cm. This is supported by the study done by Hollier L et al., [18] and Ajmal S et al., [25] providing wider inferolateral pedicle avoids flap necrosis. With regard to the arc of rotation flap undergoing wider arc of rotation to reach the defects show higher incidence of venous congestion and superficial necrosis irrespective of pedicle width, probably due to the kink in pedicle.
The complication rate was associated with co-morbidity as described in other studies [12,19,22]. A study conducted by Baumeister SP et al., [19] described venous insufficiency, arteriosclerosis and diabetes as an ‘unhappy triad’. Statistically two of three flaps are prone to necrosis if at least one of these risk factors is present and every flap will be necrotic if all three factors are present [12,19,22].
The advantage of this islanded reverse sural artery flap is that it can reach the ankle and the calcaneal areas due to long pedicle and is easy and relatively quicker to elevate. Furthermore, there is no sacrifice of major arteries; it can be created in single stage with no need of microsurgical technique [25]. There is no significant morbidity at the donor site. It may be compromised by venous congestion and peripheral arterial insufficiency when the flap is transferred with its pedicle tunneled subcutaneously. In this study, the sural nerve along with lesser saphenous vein and deep fascia was taken with the flap without extending into proximal third of leg. This ensured the safety of the flap. Further, when the pedicle was kept wide, raised as an adipofascial unit and was not tunnelled the success rate of flap was better. This is attributed to the less kinking of the pedicle and improved venous return compared to skin pedicled flaps. This is supported in the study by Hollier L et al., [18]. The exposed adipofascial pedicle was resurfaced with a skin graft. However, these are insensate flaps and sacrifice of sural nerve leads to hypoesthesia at the lateral part of the foot. The sensitivity improves if other nerves in the lower limb are intact [17]. In this study, none of the patients after six months of follow up complained about sensory disturbance over lateral border of foot.
Donor site shows minimal depression deformity in the early postoperative period. With time contour deformity becomes less prominent. In few cases, the donor site may have unacceptable scarring especially in women was reported [7,17]. In the present study, since all the patients were male they had no major complaints on donor site scarring. Donor area of the flap is generally not involved in the zone of injury even in polytrauma and hence, the graft take is better due to the presence of well vascularised muscle underneath. The modifications of these flaps like including the cuff of gastrocnemius muscle as by Al Qattan MM et al., [26], delaying the flap [27] and supercharging [28] will help to take larger flaps beyond angiosomal territory that have been experimented and studied in literature which has not been attempted in the present study as flaps were planned within the angiosmal territory.
Limitation
As per the study, obese individuals have a large amount of subcutaneous fat which causes post-operative fat necrosis and hence increases the healing time.
Conclusion
Reconstruction of the moderate sized defects over the lower third leg, heel and foot defects is always a challenge to every reconstructive surgeon with limited options available like conventional cross leg flap, perforator flaps and microvascular free tissue transfer.
From this study, we are able to conclude that islanded reverse sural artery flap with its wide arc of rotation can provide cover to lower third of leg, heel and foot defects, thereby reducing the need for staged cross leg flap and other flaps. Keeping the adipofascial pedicle wide (4 cm) and not tunnelling it subcutaneously helps to reduce venous congestion, oedema and necrosis. Thus, the islanded reverse sural artery flap is a good option to provide coverage for defects over lower third of leg, heel and foot with minimal donor site morbidity.