Rapid globalisation, technological advancements, multicultural work environments, work-life conflict, recessions and subsequent changes in the work nature had caused high stress with everyone at the workplace [1]. Meeting and beating deadlines, unnatural life style, materialistic relationships, no time for self, over indulgence, odd and long work hours, multi-tasking, bullying, poor pay scale, job insecurity, work-life conflict, role mismatch, role conflict, role overlapping and role overload are some of the prevalent potential stressors of the corporate world [2]. Prevalence of distress and its somatic and emotional indicators among corporate personnel are highly responsible for deterioration of their health and performance. The American Institute of Stress (AIS) states that stress related illness costs economy more than $ 100 billion per year and as estimated in 2001 stress costs organisations $300 billion in healthcare, workers compensation, absenteeism and turnover; and annual productivity losses hover around $17 billion [3]. Distress is a state of physical and emotional suffering produced by excessive demands for adaption [4]. At individual level, persistent stress causes PD and ED in the form of cardiac diseases, stroke, cancer, respiratory disease, arthritis, gastrointestinal disorders, genitourinary problems, musculoskeletal disorders, insomnia, psychological disorders (depression, suicide, anger, inadequacy, anxiety, sensitivity etc.,), psychosomatic illness, dermatological disorders, chronic aches, and pain [5,6]. The PD, ED and TD stand for the indicators of distress on somatic, emotional and general health of an individual.
There are number of interventions developed to cope with and manage stress and its adverse effects at individual level. According to the transactional theory of coping proposed by Lazarus and Folkman, “coping is an active and purposeful process by which an individual responds to stimuli appraised as taxing or exceeding his or her resources” [7]. Coping includes behavioural, emotional and cognitive attempts to manage the demands imposed by stressor [8]. Stress Management Interventions (SMIs) and alternative options employed for the prevention, moderation and cure of distress and its possible adverse consequences at individual and organisational level have been widely reported but found insufficient [2].
Yoga has been accepted as an optimal way of living for time immemorial and has emerged as one of the inexpensive alternatives and common means for holistic health management. Substantial research evidences support that certain yoga techniques may improve physical and mental health through down-regulation of the Hypothalamic–Pituitary–Adrenal (HPA) axis [9], elevation of immunoglobulin-A and natural killer cells [10] and decrease in inflammatory markers such as C-reactive protein, interleukin-6 and lymphocyte-1B [11] and reduction of anxiety [12] and increase in Heart Rate Variability (HRV), emotional, social, and spiritual well-being [13].
Some of the Mind-Body Interventions (MBIs) employed for stress management have focussed on the particular aspect of mind-body practice such as postures, breathing exercises, and meditations rather than employing integrated intervention of pertinent yogic practices that can positively impact body, mind and spirit for stress prevention, moderation and healing of stress born somatic or emotional problems. Hence, the researcher was aspired to assess the efficacy of an IYI comprised of selected yogic practices (cleansing techniques, postures, breathing exercises, gestures, psychic locks, concentration, meditation, attmabodha and tattwabodha, devotional chants and songs, spiritual assertions for cognitive and emotional restructuring) derived from hatha yoga, raj yoga, jyan yoga and bhakti yoga; on PD-somatic health, ED-Emotional Health and TD- overall health; of the subjects from corporate sectors. Moreover, the study was also aimed at ascertaining the nature and strength of relationship between after ED and PD in EG to assess the fact- general health is the function of mind-body interplays. The expected implication of the study was to highlight efficacy and significance of yoga to prevent and moderate PD, ED and TD for empowering general health and work performance of corporate workforce in contemporary organisations.
Materials and Methods
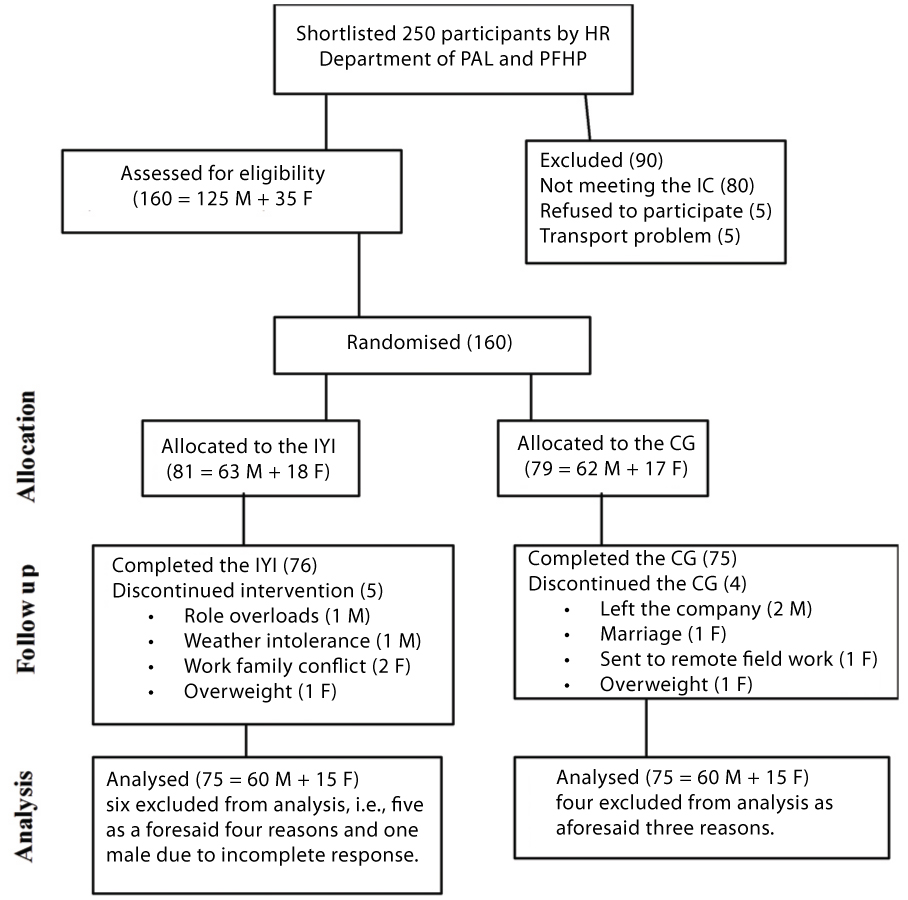
Study Design: Randomised control group design was employed to assess whether 45-day administration of the IYI among the subjects of EG cause significant reduction in distress level of the participants as compared to the controls. For this, 250 members were sampled from two corporate companies and measured in terms of PD and ED to shortlist the subjects as per Inclusion Criteria (IC). Then 160 subjects were shortlisted systematically after taking signed informed consent and subsequently assigned to EG and CG as depicted below in the CONSORT diagram [Table/Fig-1].
CONSORT Diagram.
Human Resource (HR), Patanjali Ayurved Limited (PAL), Patanjali Food and Herbal Park (PFHP), Integrated Yogic Intervention (IYI), Control Group (CG), Male (M), Female (F).
Inclusion and exclusion criteria: The age range and average age of the sampled participants were (20-65) years and 33.72 (31.44 for males and 36.0 for females) years respectively. The subjects with TD and ED greater or equal to 10 and 3 as specified in the CMIHQs [14], keen and capable for practicing the IYI were included for the sampling. The subjects with age out of the aforesaid range, operation preceding six months, contradictory medical problems with the proposed IYI, disinterest and poor commitment for the practice of yoga were excluded from the study.
Participants: Prior to the IYI, an orientation workshop was conducted among all the members of EG and CEOs of the both companies to instill the objectives, expected benefits, structure and mode of the IYI. Informed consent was signed by each participant to be included voluntarily as participants of EG and CG. One hundred sixty participants under study were randomly selected from two corporate companies namely Patanjali Food and Herbal Park (PFHP) and Patanjali Ayurved Limited (PAL), Haridwar, Uttarakhand, India, in the month of October 2011 by considering α = 0.05 (two-sided), β = 0.2 and standard effect size = 0.5 as estimated from previous studies. The IYI was administered from November to December 2011 at PFHP, Haridwar after taking prior approval from its top management and informed consent from all participants. The baseline measurements of the participants are displayed below in [Table/Fig-2]. The sample consisted of the participants with distinct roles selected from different departments such as Human Resource (HR), quality control, administration, tetra pack, Patanjali Biogas Research Institute, engineering, cosmetics, juice plant, accounts, supply and marketing. Firstly, 259 subjects meeting IC and with ranks from supervisor to chief general manager were shortlisted from the employee rosters provided by HR departments of both companies.
Baseline Measurements of Physical Distress (PD), Emotional Distress (ED) and Total Distress (TD) in EG and CG; N=number of individuals.
| Variables | Control Group (CG) | Experimental Group (EG) |
|---|
| Mean±SD(Males) | Mean±SD(Females) | Mean±SD(Males) | Mean±SD(Females) |
|---|
| Pre PD | 11.35±3.89 | 28.47±14.67 | 12.05±4.35 | 28.47±12.07 |
| Pre ED | 06.27±4.01 | 14.20±09.39 | 06.88±4.91 | 13.60±06.93 |
| Pre TD | 17.62±6.40 | 43.30±20.93 | 18.98±7.83 | 40.87±17.27 |
| Age (years) | 32.92±7.80 | 28.67±05.52 | 30.15±8.64 | 27.00±03.23 |
| N | 60 | 15 | 60 | 15 |
Measuring tool: The somatic, emotional and general health indicators of distress were categorised in terms of PD, ED and TD in the CMIHQ. The overall health contains 18 factors (12 for PD- 144 items from sections A-L and six for ED- 51 items from section M-R). The total number of dichotomous items having response yes or no in the CMIHQ is 195. PD was factorised into 12 health indicators of the distress namely A- Eyes and Ears- nine items, B- Respiratory system- 18 items, C- Cardiovascular system- 13 items, D- Digestive tract- 23 items, E- Musculoskeletal system- 8 items, F- Skin- seven items, G- Nervous system- 18 items, H- Genitourinary system- 11 items, I- Fatigability- seven items, J- Frequency of illness- nine items, K- Miscellaneous diseases- 15 items, and L- Habits- six items. Additionally, ED was measured by other six factors of the CMIHQ viz., M- Inadequacy- 12 items, N- Depression- six items, O- Anxiety- nine items, P- Sensitivity- six items, Q- Anger- nine items and R- Tension- nine items. The Hindi versions of the CMIHQ for male and female differed especially in the items of genitourinary section. The correlation coefficients between original English version and Hindi version of the CMIHQ were 0.77 and 0.87 for PD and ED respectively [15].
Data Generation: Male and female versions of CMIHQs were administered before introducing the IYI to generate baseline data and shortlist 160 participants as per IC and signed informed consent [14]. After 45 days, the same CMIHQs were administered among all the participants of the EG and CG under direct observation and instruction of the researcher. No time bar was imposed to the subjects for self-completion of the given CMIHQs. However, most of the participants completed the questionnaire in 20-30 minutes. Later IYI was administered to each participant [Table/Fig-3].
Protocol of the Integrated Yogic Intervention (IYI).
| Duration | 45 days (5 November-25 December 2011) |
|---|
| Timing | 09-10 am |
| Session hour | 45-60 minutes |
| Session days/week | Monday to Friday, rest two days were left for the self-practice |
| Activities | Description | Practice Interval |
| Cleansing Practice | Jal Neti [15] once per week | 45 minutes |
| Postures | Loosening series, Tadasana-Triyak Tadasan-Kati Chakra asana [15], spinal series or alligator twisting [16], Marjari asana, Shashanka- Bhujanga asana, Parvatasana, Tiger pose, Vakrasana, Gomukhasana, Pashimuttanasana, Shalbhasana, Vipreetkarani, Supta Vajraasana [15], spinal pose, Naukasana, Uttanpadasana, Pragya Yoga Vyayam [17] and Makarasana [15]. | 20 minutes |
| Pranayam | Nadi Shodhan, Bhastrika, Pranakarshan [18] and Bhramari [15]. | 15 minutes |
| Gestures and Meditation | Mixed Meditation with Dhyan Mudra [19]. | 15 minutes |
| Spiritual Inputs | Atmabodha, Tattvabodha and the charter of righteousness [18,20]. | five minutes |
Statistical Analysis
The design was treated as 2 X 2 mixed factorial ANOVA to check whether the mean difference among four data sets is significant or not. The four observed data sets were analysed as per the concept of 2X2 Mixed ANOVA (GLM 5) by using Predictive Analytic Software (PAS) (SPSS Inc. 18.0) The two time points of measurements- pre/before/ baseline (1) and post/after (2) were treated as within-subjects factor; and the two groups- EG (1) and CG (2) as between-subjects factor for data analyses. The level of significance was set less or equal to 0.05 (two-tailed). Simple regression analysis was used by treating post ED as the predictor and post PD as explained variable for each male and female participants.
Results
In [Table/Fig-4], the post mean PD of male practitioners is significantly smaller (p<0.001) than the post mean PD of their controls. The post mean PD seems significantly smaller (p<0.001, 37.76%) compared to pre mean PD in EG whereas, there is no significant difference between pre and post means of CG. The post mean ED of the male practitioners is significantly smaller (p<0.001) than post mean ED of their controls. On the other hand, post mean ED is significantly smaller (p<0.001, 45.2%) than pre mean ED. The post mean TD of the male practitioners is significantly smaller (p<0.00) compared to post mean TD of the controls. Post mean TD in EG is significantly smaller (p<0.001, 40.6%) than pre mean TD whereas, there is no statistically significant difference between pre and post mean TD of CG.
Summary of results regarding male participants.
| Variables | Pre-CG | Post-CG | Change (%) | Pre-EG | Post-EG | Change (%) |
|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD |
|---|
| PD | 11.35±3.89 | 10.95±3.59 | 03.5↓ | 12.05±4.35 | 07.50±3.80***,### | 37.76↓ |
| ED | 06.27±4.01 | 07.87±4.40### | 25.5← | 06.88±4.91 | 03.77±4.02***,### | 45.20↓ |
| TD | 17.62±6.40 | 18.82±6.67 | 06.8← | 18.98±7.83 | 11.27±6.59***,### | 40.60↓ |
| N | 60 | 60 | | 60 | 60 | |
Physical Distress (PD), Emotional Distress (ED), Total Distress (TD), N=number of participants, *depicts between-groups after comparison, #depicts before compared with respective after state (within group), ###stands for p<0.001, ***stands for p<0.001
In [Table/Fig-5], the post mean PD of female practitioners in EG is significantly smaller (p<0.01) than the post mean PD of their controls. On the other hand, post mean PD is significantly smaller (p<0.001, 44.26%) compared to pre mean PD (28.47) whereas there is significant increase (p<0.05, 7.23%) in post PD compared to pre PD of CG. The post mean ED (6.0) of the female practitioners EG is significantly smaller (p<0.001) compared to post mean ED of their controls. The post mean TD of the female practitioners is significantly smaller (p<0.01) compared to the post mean TD of their controls. In EG, post mean TD is significantly smaller (p<0.001, 44.87%) than pre mean TD.
Summary of results regarding female participants.
| Variables | Pre-CG | Post-CG | Change (%) | Pre-EG | Post-EG | Change (%) |
|---|
| Mean±SD | Mean±SD | Mean±SD | Mean±SD |
|---|
| PD | 28.47±14.67 | 30.53±16.68# | 07.23← | 28.47±12.07 | 15.87±11.20**,### | 44.26↓ |
| ED | 14.20±09.39 | 15.90±09.50 | 11.97← | 13.60±06.93 | 06.00±05.16***,### | 55.88↓ |
| TD | 43.30±20.93 | 45.80±21.25 | 05.77← | 40.87±17.27 | 22.53±15.51**,### | 44.87↓ |
| N | 15 | 15 | | 15 | 15 | |
Physical Distress (PD), Emotional Distress (ED), Total Distress (TD), N=number of participants, *depicts between-groups after comparison, #depicts before compared with respective after state (within group), **stands for p<0.01, ***stands for p<0.001, ###stands for p<0.001
Association between PD and ED: Two regression analyses (one for each males and females) were run to assess the strength and nature of relationship between post PD and ED with the presumption that PD is the function of ED.
In [Table/Fig-6], the R between post- PD and post-ED is 0.51 (p<0.01) thereby, explaining 26% variation in post-PD because of post-ED. Observed Beta value indicates the rate of change of post- PD by 0.51 with per unit change in post-ED. t=6.51, signifies the variance explained by post-ED on post-PD is significant at p<0.001.
Regression of post-PD on post-ED in case of male participants.
| Variables | Beta value | Std. error | Beta value | t | p-value |
|---|
| Constant | 6.63 | 0.51 | | 6.51 | 0.001 |
| ED | 0.45 | 0.07 | 0.514 |
| R | 0.51** | | |
| R2 | 0.26 | | |
| Adj. R2 | 0.26 | | |
Emotional Distress (ED), **stands for p<0.01 for two-tailed test. In case of R, n=120.
In [Table/Fig-7], the R between post-PD and post-ED is 0.58 (p<0.01) thereby, explaining 34% variation in post-PD because of post-ED. Observed Beta value indicates the rate of change of post- PD by 0.58 with per unit change in post-ED. t = 3.77, signifies the variance explained by post-ED on post-PD is significant at p<0.001. The observed Beta values displayed in [Table/Fig-6,7] inferred that ED-emotional health is the predictor of PD-somatic health.
Regression of post-PD on post-ED in case of female participants.
| Variables | Beta value | Std. error | Beta value | t | p-value |
|---|
| Constant | 12.09 | 3.8 | | 3.77 | 0.001 |
| ED | 1.013 | 0.27 | 0.58 |
| R | 0.58** | | |
| R2 | 0.34 | | |
| Adj. R2 | 0.31 | | |
ED: Emotional Distress; **stands for p<0.01 for two-tailed test. In case of R, n=30.
Discussion
That results showed efficacy of 45-day IYI for significant reduction of PD, ED, and TD of the participants in EG compared to controls in case of both males and females. The reduction in post-ED of EG as compared to controls has been found more significant (p<0.001) than reduction in PD (p<0.009) and TD (p<0.002) in case of females. The intra group reduction of PD, ED and TD in EG after the IYI was found significant (p<0.001) for both males and females respectively. Comparison of means between respective before and after states of CG showed non-significant change in PD, ED and TD of males and in ED and TD of females excluding significant increase (7.23%, p<0.05) in post PD of females.
Regression analysis showed 26% and 34% variation in PD explained by ED in males and females respectively. This hints slightly more impact of emotional health on somatic health of females as compared to males. The correlation coefficient between post ED and PD found significant at p<0.01 in both males and females.
Health promotion and reduction of distress as the consequence of prolonged yoga practice has been advocated by substantial studies. According to National Center for Complementary and Alternative Medicine (NCCAM), mind-body medicine typically incorporates health promoting intervention strategies such as relaxation, hypnosis, visual imagery, meditation, yoga, biofeedback, tai chi, qi gong, cognitive-behavioural therapies, group support, autogenic training, and spirituality [21].
Impacts of the proposed IYI comprised of Jala Neti, selected postures, yogic breathing exercises, gestures, locks, meditation and spirituality based cognitive inputs may be based on five-principles namely proper relaxation, proper exercise, proper breathing, proper diet, positive thinking and meditation as reported by Chanavirut R et al., and cleansing as well [22].
Practice of the IYI may improve musculoskeletal functioning, cardiopulmonary status, ANS response and endocrine functioning at physical level; enhance self-esteem, coping, social support and positive mood at psychosocial level; and elevate compassionate understanding and mindfulness at spiritual level [22]. Mechanisms underlying the modulating effects of yogic cognitive-behavioural practices (meditation, asanas, pranayama, caloric restriction etc.,) on human physiology can be categorized into four transduction pathways namely nervous system activity, humoral factors, cell trafficking, and bioelectromagnetism that clarify how yogic practices might optimise health, delay ageing, and ameliorate chronic illness and stress from disability [23].
The effect of mixed meditation included under the IYI can be predicted on the basis of the subsequent findings reported by other researchers. Continued practice of meditation develops the ability to increase activity in the activated bands (alpha, beta, and gamma) of the Electroencephalogram (EEG) and dopamine stimulation through the mesolimbic reward systems resulting in blissful experience [24]. Yoga manages stress, enhances central inhibitory GABA levels, changes CNS blood flow and leads to an autonomic quieting in case of both seizures and its associated autonomic dysfunction [25].
Furthermore, one of the most prevalent presumptions is that promotion of health, prevention of disease and moderation of health problems by the prolonged yoga practice happens through the boosting of immune system. Some of the studies have been supporting this fact as yoga reverses the negative impacts of stress on the immune system by increasing levels of immunoglobulin A and natural killer cells, and decreasing inflammatory markers such as C-reactive protein, interleukin-6 and lymphocyte-1B as cited in Ross A and Thomas S, and Rao RM et al., [9,10].
Efficient cardiopulmonary functioning in the body system is another essential aspect for distress moderation and rehabilitation. Particularly, pranayam, bandha, mudra and asanas practiced under the IYI incorporate systemic and subsequent inhalation, exhalation, inner breath and outer breath retentions which are responsible to cause contraction and stretching of lung tissues and chest wall. These improve the cardiopulmonary function (lung function, heart rate, breath rate, heart rate variability, oxygen consumption, and CO2 expulsion), endocrine and neural secretions and function of associated visceral organs.
The IYI given was comprised of the practice of loosening series of postures synchronised with forceful inhalation and exhalation and mental awareness to the affected body parts, breath control exercises (pranayams), mixed meditation and renewing spiritual contemplations. In case of deep breathing, we inhale 3000 cc and exhale 1500 cc more air in addition to tidal volume; thereby increasing Vital Capacity (VC) and Expiratory Reserve Volume (ERV). This implies that deep breathing enhances Total Lung Capacity (TLC). Moreover, the continuous contraction and relaxation of the lung tissues during the practice of Nadisodhan Pranayam, Bhramari Pranayam and Pranakarshan Pranayam might enhance their elasticity and hence, surface area too. Both of these actions result in increased oxygenation of the blood and eventually increased oxygen supply to cellular level of the body. This results in the efficient functioning of the body organs and regulated endocrine and neuro-hormonal secretions.
Another mode of the effect of the IYI to lower distress can be discussed from a psychological perspective. Hatha yogic scriptures have explicitly asserted the interplay of breath and mind. Flight-fight stage, fear, and arousal fasten the breath rate to increase oxygen supply to the cellular level to make up the additional energy required to cope with the encountered stressor whereas serene, calm and happy moods are associated with slow and steady deep breathing. This concept implies that psychological (cognitive and emotional) status can be affected by yogic breath control exercises like Nadisodhan Pranayam, Bhramari Pranayam and Pranakarshan Pranayam. Breathing is an autonomic process though the rate of breathing can be altered voluntarily during the practice of pranayamas and asanas. Respiratory center can be inhibited and activated voluntarily by the practice of aforesaid pranyams. Practice of postures- padahastasana, pashimuttanasana, parvatasana and marjari; and breath control exercises- Bhastrika Pranayam under the IYI might be responsible to create negative pressures (20-80 mmHg) inside the visceral cavities like esophagus, stomach, urinary bladder, colon [26,27] and possibly in kidneys by restricting the blood flow in the suppressed visceral organs (of abdominal and pelvic cavity) eventually to create cellular hypoxia. Relaxation of Uddiyan Bandha increases the blood flow exponentially in the restricted sites thereby increasing supply of oxygen and nutrients. Decreased supply of oxygen (during Uddiyan Bandha) to the kidneys promotes the process of erothropoiesis and formation of RBCs [27].
Efficacy of the IYI also can be discussed from the perspective of cardiac health. Emotional stress, negative emotions and behaviours such as intense anxiety, depression, feelings of helplessness, and type A behaviour characterised by ambitiousness, competitiveness, impatience, and a sense of time urgency are major causes in the pathogenesis of cardiac diseases [24]. Slow and controlled breathing as practiced in yoga nidra immediately enhances HRV and improves baroreflex sensitivity [28]. The practice of Pranakarshan Pranayam might have similar impact on cardiopulmonary function (to increase heart rate variability and improve barorelflex). Intensive lifestyle changes (consisted of a 10% fat whole–food vegetarian diet, aerobic exercise, stress management training-yoga and meditation, smoking cessation, and group psychological support) could lead to regression of CAD after only one year of a five year program [24]. Pullen PR et al., also reported improved cardiovascular endurance and decreased inflammatory markers (Interleukin-6 and C- reactive protein) in heart failure patients thereby showing similar effects of yoga as massage therapy [11].
Practice of yogic postures causes sponge like squeezing in the soft tissues of the digestive organs, and encourages stale and waste-bearing fluids to be removed from the tissues thereby, facilitating the elimination of the faeces and supply of essential nutrients to these sites. Subsequent opening and stretching of digestive organs during the practice of yogic postures regulates the peristalsis movement that is a key involuntary process for the proper digestion and elimination. Besides, yogic breathing exercises send oxygen deep into the cells of the body and help it to absorb nutrients and excrete morbid matters thoroughly. On the other hand, efficacy of yoga for stress management, rebalance of the autonomic nervous system to create deep relaxation and dominate Parasympathetic Nervous System (PSNS) is well documented. The PSNS dominance induced by the yogic practices facilitates the supply of blood and oxygen to the digestive visceras and betters peristalsis movement. The inverted posture like Vipreetkarni is supposed to heal the problem of hyperacidity and flatulence by inhibiting the growth of helicobacter pylori. Regular practice of Vipreetkarani more than five minutes per day brings down the air filled in the funds part of the stomach to pyloric region and might inhibit the growth and functioning of anaerobic helico bacter pylori. Datta K et al., [29] also reported that practice of 300 head end elevated supine posture and other similar supine postures improved the level of reflux in 15 Endoscopy Normal Reflux Disease (ENRD) patients with age range of 39±7 years. This effect may be due to denervation of fundus and uniform distribution of fundus air thorough stomach during the supine posture like Vipreetkrani since, transient sphincter relaxation happens due to excitation of mechanoreceptors caused by air located in the fundus while movement of fundus air towards pyloric region (in case of supine posture like Viprretkarani) inhibits excitation of mechanoreceptors located in the fundus thereby inhibiting sphincter relaxation [29]. It can be hypothesised that modulation of vagal tone by yoga practices betters the flow of oxygen and blood to the pancreas thereby bettering its exocrine and endocrine secretions. The satiety and appetite center located at lateral part of hypothalamus might be positively affected by optimal feelings and thoughts; energising, tranquilising, and soothing effects induced by breath control exercises and mixed meditation practiced under the IYI. Sequential practice of Tadasana, Triyak Tadasana, Kati Chakra asana and Triyak Bhunjangasana is a proven series of postures to ease egestion during Sankhaprakshalan (one of the potential yogic cleansing techniques of entire gut). The postural series and breath control exercises contained in the IYI seems to be effective to remove both intestinal constipation and psychic constipation which are responsible for the onset of somatic and psychological distress/ailments.
Regular yoga practice is also found to improve the fatigability and other factors of ED like tension, anger, and mental disturbance. Yoshihara, Hiramoto, Sudo and Kubo reported significant reduction in mental disturbance, psychological distress, tension-anxiety, anger-hostility, and fatigue along with decrease of the urine 8-hydroxydeoxyguanosine (8-OHdG) among long-term yoga practitioners (having practice experience two years or more) compared to the controls [30]. Sudarshan Kriya Yoga (SKY) is a potential and low-risk adjunct for the treatment of stress, anxiety, PTSD, depression, stress-related medical illnesses, substance abuse, and for the rehabilitation of criminal offenders in which Ujjayi practice as a major part of SKY calms the mind, reduces obsessive worry, and induces a state of physical and mental calmness conducive to sleep [31]. This implies that Bhastrika and Pranakarshan Pranyam might have similar effects on the participants of EG as their practice techniques resemble to SKY.
The traditional theory of yoga therapy asserts that prana is prime force that needs to be spontaneously and properly circulated to each and every parts of the body to make them healthy and efficient. On contrary, depletion or congestion of prana to particular body site makes it diseased. Moreover, the imbalanced pranic flow into subtle energy channels that exist in etheric body is supposed to be an antecedent of the disease manifestation. In this connection, Acharya argued that the inhalation of negative ions (from cosmos) during yogic breath control exercises like Bhastrika, Nadisodhan, Pranakarshan and Bhramari, their access to alveoli, diffusion into pulmonary capillaries, and circulation through the entire body via blood and their discharge back to the cosmos through the skin pores. This mechanism generates a closed electric circuit between the practitioner and cosmos and hence, enhances and channelises bioelectricity throughout the body [32] leading to perfect health, stillness and heightened awareness as mentioned in the Gherand Samhita.
Thus, the IYI was efficacious to reduce PD, ED and TD of the practitioners as compared to their controls. Interestingly, level of pre PD, ED and TD and the reduction percentage in post PD, ED and TD has been found more in female practitioners compared to the male practitioners. This may be due to work-life conflict met higher among females due to their engagement in office and family as per traditional Indian culture as some of the female practitioners verbally reported the high pressure because of their involvement in children’s care and other family affairs before and after office hours. There was significant association between ED and PD and ED significantly predicted PD thereby ensuring mind-body interplays.
Limitation and Recommendations
This study had some limitations as under: (1) The reduction of distress as the effect of the IYI needs to include measurement of bio-chemical (catecholamine, cortisol, biopyrrin, 8-HOdG) and autonomic (HRV) indices along with psychometric measurements to make the efficacy of the YI more reliable and generalisable as in Indian culture, participants hesitate to disclose their health problems that may lessen reliability of the collected qualitative information;(2) The number of female subjects was small because of low access and availability of female employees in sampled corporate companies; (3) The analysis of data have not been made separately by partitioning included wide age range (20–65 years) to control extraneous effect of age on distress. Hence, in further studies, effect of similar IYI can be assessed separately on different age groups created by considering variation of stressors; (4) This study has included the hypothesis to assess the efficacy of the IYI on individual indicators (particularly health indicators as rated by the CMIHQ) of professional distress. Hence, future studies are suggested to assess the efficacy of the IYI on both major dimensions of distress- professional distress and organisational distress, and their respective factors as determined by White WL [4]; (5) The data analysis did not consider the separate factor-wise difference in pre and post measurements of PD and ED, so the study could not ensure the extent of reduction on 12 and six factors of PD and ED separately; (6)The study could not ensure which yogic practice(s) under the IYI has (have) contributed more to reduce the distress because the IYI was the combination of postures, gestures, neuromuscular locks, breath control exercises, meditation and spiritual assertions. Therefore, more rigorous studies are warranted by caring aforesaid limitations to generalise the efficacy of the IYI for managing distress and empowering general health of corporate workforce.
Conclusion
The 45-day IYI significantly improved psychosomatic health of its practitioners by reducing their PD, ED and TD and implied that work place yoga may be an inexpensive and effective complementary and alternative approach for boosting general health and maximising efficiency of the corporate personnel. The emotional health predicted somatic health by implying emotional wellness as an antecedent for somatic wellness.
Physical Distress (PD), Emotional Distress (ED), Total Distress (TD), N=number of participants, *depicts between-groups after comparison, #depicts before compared with respective after state (within group), ###stands for p<0.001, ***stands for p<0.001
Physical Distress (PD), Emotional Distress (ED), Total Distress (TD), N=number of participants, *depicts between-groups after comparison, #depicts before compared with respective after state (within group), **stands for p<0.01, ***stands for p<0.001, ###stands for p<0.001
Emotional Distress (ED), **stands for p<0.01 for two-tailed test. In case of R, n=120.
ED: Emotional Distress; **stands for p<0.01 for two-tailed test. In case of R, n=30.