Breast cancer is the most common type of cancer in Asian countries. In Iran, the crude incidence rate of breast cancer is about 21.4 per 100,000 population [1]. It seems that Iranian women develop breast cancer 10 years earlier than women in the developed countries [2]. While early diagnosis can increase the patient’s five-year survival rate up to 97% [3], many Iranian women are not aware of warning signs of breast cancer [4]. Although, BSE has been found to be a useful screening tool, but BSE is not routinely practiced (17%) in Iran [2,5]. Based on the purpose of the screening programs, it is recommended that 70% of women older than 20 years should annually perform BSE [3] yet, the rate of women in this age group who actually screen is only 31.7% in Iran [5]. Knowledge and attitudes about BSE is also limited [6]. Making women aware of the warning signs of breast cancer and the benefits of the screening methods can help to save their lives [2]. In order to increase women’s participation in breast cancer screening and prevention programs, especially among high-risk groups, intervention strategies should be designated according to their knowledge and sociodemographic factors [1].
Although, there is an emphasis on healthcare training and counseling for students, the question of "which method of the education is the most effective one on students’ behaviors, communication and counseling skills?" has been left unanswered [9]. Sangestani G and Khatiban M, have shown that active strategies in midwifery education can be very effective [10]. Role-playing is a special kind of active educational strategy [11] commonly used in communication skill programs due of its accessibility, low cost and effectiveness [12].
Role-playing is based on social learning theory with following steps: 1) preparing the group; 2) choosing the presenter; 3) staging; 4) making the audience ready; 5) role-playing; 6) evaluating; 7) replaying the role; 8) evaluating; 9) Generalising and transfering the experiences to the others [11]. In the present study, we applied a method in which the students were learning while were training and counseling their clients about BSE.
In order to determine the effectiveness of role-playing strategy we compared the BSE training and counseling skills of midwifery students in the role-playing group with those in the conventional group. We also compared the knowledge, health beliefs and skills of women trained by the role-playing students with those trained by the conventional students.
Materials and Methods
Design
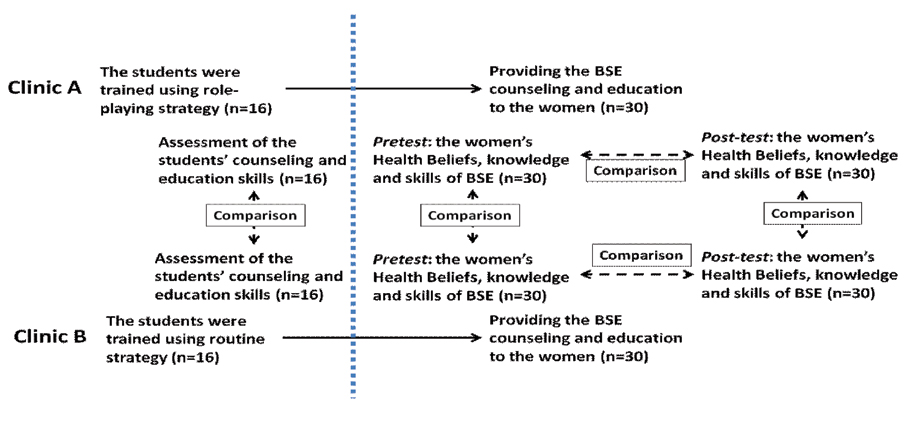
This was a quasi-experimental study. A post-test only design study with control group was conducted for the first objective (comparing the BSE training and counseling skills of midwifery students in the role-playing group with those in the conventional group), and a pre-test post-test design with control group was conducted for the second objective (comparing the knowledge, health beliefs and skills of women in experimental group with those in control group). Both parts of the study were reported in May, 2014 at Hamadan University of Medical Sciences, Hamadan, Iran. The flow diagram of study phases and participants is shown in [Table/Fig-1].
The flow diagram of study phases and participants.
Participants
For the first objective, all eligible students were invited to participate in the study. Inclusion criteria included being in the third-year undergraduate midwifery program and practicing the clinical course of the “Gynaecology” in Hamadan city. By census, 32 students in two separate healthcare clinics were assigned randomly to either the role-playing group (16 students, in Clinic-A) or the conventional group (16 students, in Clinic-B). None of the students has been excluded from the study because, they did not meet the exclusion criteria as being transitional, guest or on probation during the study and excessive absences. This clinical course was held in semester six of undergraduate midwifery program for 10 days (60 hours).
For the second objective, all the women of the study period referred to both the clinics were considered as the research population. In this part of the study, the sample size with 5% error and 80% power was calculated 60 women.
From those, through convenience sampling, 30 women were assigned to the experimental group (trained and counseled by the role-playing group of students) and 30 women were assigned to the control group (trained and counseled by the conventional group of students). In order to participate, the women had not to be pregnant and without a history of either physical or mental illness.
Procedure
To meet the first objective, two course plans based on the objectives of clinical course of the “gynaecology” for both the role-playing and conventional groups were designed. All the features of the course plans were similar with the exception of the strategies for preparation of the students for training and counseling of the women. The timetable of the courses was in four parts: 1) orientation; 2) preparation; 3) training and counseling; and 4) evaluation.
At the first day, the researcher provided the BSE training and counseling to a small group of women as an orientation session for the students. Educational materials such as mannequins, pamphlets, posters, photos and powerpoints were provided to the students by the researchers. The contents of the BSE curriculum included the domains of the health belief model which was the same for the both role-playing and conventional groups.
The role playing strategy was developed based upon Benbassat J and Baumal R, extensive study [13]. The scenarios of the BSE training and counseling were given to the role-playing group on the first day. The role for each student in the role-playing strategy was addressed as well. There were eight students in each group; one played in the role of the consultant, one played the woman who received care and the rest observed. Two days later, the role-playing exercise was repeated by the students under the supervision of the instructor. The strengths and weaknesses of the program were discussed and suggestions for improvement were given to the students at the end of each session. Finally, an evaluation was conducted by the instructor and students. The conventional students were asked to study the educational materials in order to prepare for the training and counseling of the women.
Both group of the students provided training and counseling to the women in the clinic within four days. The students used the relevant pamphlets and posters for training the women to practice the BSE. Finally, the students were expected to respond to questions raised by the women about perceptions of susceptibility, severity, BSE benefits, barriers to BSE, and BSE self-efficacy. The duration of each session was about one hour. The instructor supervised all the sessions. On the tenth day, there was a discussion with both groups about the whole program and then the students were evaluated by the instructor.
Instruments
Two tools were used for data collection in this study. Each was evaluated for face and content validity by 10-expert panel who were faculty members with enough experience in clinical education. They were developed according to the literature as follows:
The first tool is an observational structured checklist of the students’ training and counseling skills. The “Direct Observation through Structured (DOS) checklist” developed in this study was principally inspired from the previous study [7] and modified for the present study with 20 items containing “yes” and “no” responses [Table/Fig-2]. The given score for answers “yes” was one, and for answers “no” was zero. So, the range of the grades was 0-20. In this sample, Cronbach’s alpha was 0.85, indicating good level of internal consistency. This checklist was filled by one of the researchers through direct observation.
A checklist for evaluation of student’s counseling and training skills to the women on how to do breast self-examination.
| Row | Classifications | Item | Yes=1 | No=0 |
|---|
| 1 | Introduction | She began the meeting with greetings and introduced herself | | |
| 2 | She announced the time, regulations and objectives of the session | | |
| 3 | She brought up some questions to determine the needs of the women’s counseling | | |
| 4 | Content | She described about breast cancer | | |
| 5 | She described the factors affecting breast cancer | | |
| 6 | She explained the importance of breast cancer early detection | | |
| 7 | She explained the benefits of breast self-examination (BSE) | | |
| 8 | She explained the BSE barriers | | |
| 9 | She talked about the best time for BSE | | |
| 10 | She explained how to do the “observation” as the first step of BSE | | |
| 11 | She explained how to report on the results of the observation | | |
| 12 | She explained how to do the “palpation” as the second step of BSE | | |
| 13 | She explained how to report on the results of the palpation | | |
| 14 | Assessment | She summed up the content | | |
| 15 | She responded to the participants questions | | |
| 16 | She thanked the participants for their attention | | |
| 17 | Educational and Counseling behavior | She used the appropriate audiovisual aids for better understanding of the audience | | |
| 18 | She tried to attract the attention of women by appropriate moving and changing the tone of her voice | | |
| 19 | Her presentation was according to the counseling needs of the women | | |
| 20 | She developed a situation for group discussion | | |
The second tool is a scale for health beliefs, skills, and knowledge of BSE in the women referred to health centers in Hamadan. This scale has four sections:
1) The demographic data questionnaire obtained information about the women’s sociodemographic characteristics (age, current marital status, ethnicity, level of education, employment status, husband level of education, husband employment status, income level, and having children), and other factors (having knowledge of breast cancer, doing BSE, having a family history of breast cancer, and having problem of breast).
2) The Champion’s Health Belief Model Scale (CHBMS) of breast cancer screening is a tool with 31 items in five subscales: perceptions of susceptibility (3 items), severity (6 items), BSE benefits and barriers to BSE (12 items), and BSE self-efficacy (10 items). It employs five-point Likert responses. The CHMBS, developed by Champion VL [14] was adapted for Iranian women by Tavafian SS et al., [15]. Higher scores reflect a higher degree of health beliefs in all subscales except in the barriers to BSE and severity. In our study, Cronbach’s alpha or internal consistency was 0.79, indicating good levels of internal consistency. The CHBMS were completed by the women (self-reporting) in both arms of the study, both before and after interventions.
3) The observational BSE skills checklist was developed according to Wood’s instrument in breast self-examination proficiency rating [16]. It is used to assess the BSE inspection and palpation skills as the woman demonstrates BSE on herself before and after BSE training and counseling session. It has 13 items with “yes” and “no” responses with scores of 0-13. Its Cronbach’s alpha for internal consistency was 0.73, indicating sound levels of internal consistency. The BSE skill was measured at pre and post intervention in both groups.
4) The BSE knowledge questionnaires were filled for each woman by a student through interview before and after BSE training and counseling session. The BSE knowledge questionnaire has 15 items and was developed by researchers for this study based on an extensive review of the literature [17,18]. Reponses include “correct”, “incorrect” and “uncertain” answers. The correct answer was given one point and the incorrect or uncertain answers were given zero. Knowledge scores were rated 0-15. Its Cronbach’s alpha for internal consistency was 0.77, indicating sound levels of internal consistency. It was applied at pre and post intervention in both groups of women.
To have interobserver reliability, all students were taught how to interview with the women on the BSE knowledge questionnaire and how to observe the women according to the checklists. Then, the students were asked to fill the checklists and questionnaires for one of the participant under the supervision of the researchers.
The research proposal was registered in the Iranian Registry of Clinical Trial (IRCTID: IRCT201205269862N1). Then, the Ethics Committee and Research Council of Hamadan University of Medical Sciences approved the study (No: 16/35/9/1005). All the participants voluntarily signed informed consent form before the enrollment in the study.
Statistical Analysis
The significant differences between the personal and social characteristics of women in the experimental and control groups were assessed by Chi-square test or the Fisher’s exact test. The results of women’s mean grades of BSE health beliefs, skills and knowledge in experimental and control groups are presented as the means ± standard deviation before and after intervention. The significant differences between groups were assessed by t-test and intra group were assessed by paired t-test. The differences were considered significant if the two-tailed p-values were ≤0.05. We used SPSS-version 16.0 for the data analysis.
Results
The participating students in the conventional (n=16) and in the role-playing group (n=16) had respectively a mean age of 22.06 (±0.93) and 22.19 (±1.47) years; high school Grade Point Average (GPA) of 17.43 (±1.27) and 17.50(±1.90); and GPA 16.47 (±1.07) and 16.78(±1.32) in the previous semester. There were no significant differences between the two groups (p>0.05) in these variables. About, 87.5% students in the conventional group and 93.8% students in the role-playing group were single; 75.0% in the conventional group and 62.5% in the role-playing group were not living in the dormitory. None of the students participated in this study had a history of working as a health care staff.
The scores of the students’ skills in the BSE training and counseling are shown in [Table/Fig-3]. The mean score of the BSE training and counseling skills in the role-playing group students was significantly higher than that of the conventional group (t=-13.00, df=30, p<0.001).
The scores of the BSE counseling - training skills in both groups of students based on DOS (range of the grades are 0-20).
| Grades | Role-playing group (n=16) | Conventional group (n=16) |
|---|
| 0-8 | 0 (0.0%) | 0 (0.0%) |
| 8-11 | 0 (0.0%) | 11 (68.8%) |
| 12-15 | 1(6.2%) | 5 (31.2%) |
| 16-20 | 15 (93.8%) | 0 (0.0%) |
All the women participating in the study were married and living in the city. Their mean age was 30.87 (±6.29) in the control group, and 31.83 (±6.72) in the experimental group. Other social and demographic characteristics are presented in [Table/Fig-4]. The statistical tests showed that the studied demographic characteristics were similar in the two groups of women.
Comparing the personal and social characteristics of women in the experimental group with those in the control group.
| Characteristics | Experiment group (n=30) | Control group (n=30) | p-value |
|---|
| Age (year) | <25 | 6 (20.0%) | 9 (30.0%) | 0.57§ |
| 25-30 | 6 (20.0%) | 5 (16.7%) |
| 31-35 | 8 (26.7%) | 7 (23.3%) |
| 36-40 | 8 (26.7%) | 9 (30.0%) |
| >40 | 2 (6.7 %) | 0 (00.0%) |
| Ethnicity | Fars | 17 (56.7%) | 19 (63.3%) | 0.15§ |
| Others | 13 (43.3%) | 11(36.6%) |
| Education | 1-5 year | 4 (13.3%) | 5 (16.7%) | 0.34§ |
| 6-11 year | 9 (30.0%) | 6 (20.0%) |
| Diploma | 14 (46.7%) | 15 (50.0%) |
| Associate degree | 2 (6.7%) | 1 (3.3%) |
| Bachelors or higher | 1(3.3%) | 3 (10.0%) |
| Work | Housekeeper | 17 (56.7%) | 20 (66.7%) | 0.57§ |
| Employee | 9 (30.0%) | 7 (23.3%) |
| Free job | 4 (13.3%) | 3 (10.0%) |
| Number of children | 0 | 2 (6.7%) | 1(3.3%) | 0.74§ |
| 1 | 8 (26.7%) | 7 (23.3%) |
| 2 | 14 (46.7%) | 17 (56.7%) |
| 3 | 6 (20.0%) | 5 (16.7%) |
| Husbands’ work | Unemployment | 1 (3.3%) | 2 (6.7%) | 0.47§ |
| Employee | 8 (26.7%) | 9 (30.0%) |
| Free job | 21 (70.0%) | 19 (63.3%) |
| Husbands’ education | 1-5 year | 2 (6.7%) | 4 (13.3%) | 0.66§ |
| 6-11 year | 7 (23.3%) | 5 (16.7%) |
| Diploma | 14 (46.7%) | 9 (30.0%) |
| Associate degree | 5 (16.7%) | 6 (20.0%) |
| Bachelors or higher | 2 (6.7%) | 6 (20.0%) |
| Husbands’ ethnicity | Fars | 13 (43.3%) | 14 (46.7%) | 0.59§ |
| Others | 17 (56.7%) | 16 (53.3%) |
| Monthly income (χ10000 R %) | 200-450 | 15 (50.0%) | 11 (36.7%) | 0.31§ |
| 451-600 | 5 (16.7%) | 9 (30.0%) |
| 601-850 | 6 (20.0%) | 5 (16.7%) |
| 851-1100 | 4 (13.3%) | 3 (10.0%) |
| >1100 | 0 (00.0%) | 2 (6.7%) |
| BSE information | No | 24 (80.0%) | 22 (73.3%) | 0.68§ |
| Somewhat | 6 (20.0%) | 8 (26.7%) |
| Have problem in Breast? | No | 4 (13.3%) | 3 (10.0%) | 0.47§§ |
| Don’t know | 26 (86.7%) | 27 (90.0%) |
§ Non significant; Chi-square test
§§ Non significant; Fisher’s-exact test
[Table/Fig-5] shows the average scores of women in the areas of the Health Belief Model, knowledge and skills of breast self-examination. Paired t-test showed that the average response to the realm of "perception of susceptibility" in both the control (p<0.01) and experimental (p<0.001) groups had a significant improvement. But the test showed that the average response to the area of the "perception of seriousness" improved significantly in the experimental group (p<0.001) only. The paired t-test also showed that the mean score of the participants’ response in the both experimental and control groups in terms of the "BSE benefits", "BSE barriers", "BSE self-efficacy", skills in and knowledge of the BSE had a significant increase (p<0.001). Independent t-test showed that the mean score of responses in both groups were almost similar in the areas of the Health Belief Model, skills in and knowledge of the BSE (p<0.05) before the intervention but after the intervention it significantly improved in the experimental group when compared to the control group (p<0.001).
Comparison of the mean grades of BSE perceptions of susceptibility, seriousness, self efficacy, benefits, barriers, skills and knowledge before and after intervention in experimental and control groups.
| Variables | Experimental group (n=30) | Control group (n=30) | p-value |
|---|
| Perception of susceptibility(0-4) |
| Before intervention | 1.69±0.38 | 1.63±0.35 | 0.56 |
| After intervention | 3.12±0.37 | 1.82±0.36 | <0.001** |
| p-value | <0.001* | 0.002* | <0.001*** |
| Perception of seriousness (0-4) |
| Before intervention | 3.27±0.19 | 3.38±0.24 | 0.06 |
| After intervention | 2.68±0.18 | 3.33±0.21 | <0.001** |
| p-value | <0.001* | 0.18 | <0.001*** |
| BSE benefits (0-4) |
| Before intervention | 2.19±0.26 | 2.18±0.25 | 0.79 |
| After intervention | 3.49±0.26 | 2.45±0.23 | <0.001** |
| p-value | <0.001* | <0.001* | <0.001*** |
| BSE barriers (0-4) |
| Before intervention | 2.70±0.25 | 2.71±0.23 | 0.84 |
| After intervention | 0.90±0.23 | 2.47±0.21 | <0.001** |
| p-value | <0.001* | <0.001* | <0.001*** |
| BSE Self-efficacy (0-4) |
| Before intervention | 1.15±0.18 | 1.13±0.22 | 0.75 |
| After intervention | 3.33±0.19 | 1.68±0.21 | <0.001** |
| p-value | <0.001* | <0.001* | <0.001*** |
| BSE Skills (0-13) |
| Before intervention | 1.73±1.3 | 1.67±0.99 | t=-0.23, p=0.82 |
| After intervention | 10.03±1.73 | 6.20±1.4 | <0.001** |
| p-value | <0.001* | <0.001* | <0.001*** |
| BSE Knowledge (0-15) |
| Before intervention | 2.37±1.8 | 2.70±1.5 | 0.44 |
| After intervention | 9.10±2.5 | 5.90±1.7 | <0.001** |
| p-value | <0.001* | <0.001* | <0.001*** |
* Significant; Paired t-test
** Significant; Unpaired t-test
***Significant; Repeated Measurement
Discussion
In line with the first objective of the study, the results showed that using the role-playing strategy can improve students’ training and counseling skills of BSE. This finding is consistent with existing research on the use of role playing for medical education. For example the findings of a study from Pakistan showed using role playing can enhance the medical students’ communication skills [7]. In a Germany study, researchers used role playing method for teaching communication skills in medical students. They found that role playing is very useful in teaching and learning this kind of subject from the student’s point of view [19]. In Iran, researchers found that the role playing method is useful for teaching communication skills [20,21]. Use of role playing strategy is recommended for training midwifery students’ consulting skills in clinics as well [22]. Research has shown that role playing is also particularly useful for some groups. For example in primiparous women, the knowledge and attitude to the kind of delivery can change significantly after role play exercises when compared with other teaching methods [23]. The use of role-playing strategy and subsequently its application in the clinical practice can facilitate the transition from being a student to a professional person in midwifery students [24].
In line with the second objective of the study, our findings showed that the women’s pre-training scores of health beliefs, knowledge and skills of BSE were low. These findings are supported by similar studies [25,26]. Despite our research, in a study in Malaysia 81.1% of subjects were aware of breast cancer and 55% used BSE [27] and in another study 67.7% of women were aware about BSE and 55.8 % used it [28]. This inconsistency may be due to the lack of educated women (11.7%) in our sample. Specially, in Turkey, the researchers found that the scores of "perceived susceptibility" and "perceived barriers" in graduated women were significantly higher than that of others [29].
Although the BSE training and counseling by students did improve the women’s “perceived susceptibility”, "perceived benefits", "perceived barriers", "self-efficacy" and "perceived severity" in both the groups, the women trained by the role-playing group of students had dramatically higher scores in health beliefs about BSE (p<0.001). In line with this finding, some studies showed that training can improve women’s health beliefs (perceived susceptibility, perceived severity, perceived benefits and barriers) significantly [30-33]. The health belief model is applicable even for short programs. A program of about 120-minutes can promote breast health education and result in a significant increase in the frequency of BSE skills and knowledge to provide breast health [34]. It can be concluded that the improvement in the health beliefs and attitudes can lead to the persistence of using BSE [35].
The improvement in the BSE knowledge and skills were significantly higher in women taught by the role-playing group of students than those taught by the conventional students (p<0.001). Research has shown that regardless of educational method, BSE education is able to increase both women’s knowledge and screening behaviors [36]. It has been shown that the BSE education presented by healthcare professionals can improve BSE awareness and practice among women [5,34,37]. We found that training by the midwifery students about BSE can also be effective in other healthcare settings. In Iran, it has been shown that training provided by the students compared with those provided by the staffs can change people’s attitudes about barriers to BSE more effectively [38]. There are many studies assessing knowledge and attitude of females towards Breast self-examination. But only a few interventional studies have conducted to show the effects of the educational intervention by the nursing/midwifery personnel on the women’s attitudes, knowledge and practice. The present study is unique because the participated students were engaged in learning while were training and counseling their clients about BSE.
Limitation
The differences in the students’ interests and their efforts for training and counseling could be the limitation of the present study. The sample size of the students was small as well. So, we recommend conducting a study with a higher number of the students in other field of clinical education.
Conclusion
The training and counseling skills in the role-playing group of students were improved due to using the role playing strategy so they could be more effective in transferring knowledge and skills of BSE and in developing health beliefs to the women. In turn, it can aid in early detection of breast masses and timely treatment in the susceptible population. Therefore, we recommend this method not only in midwifery education but also in the other fields of study which have clinical training.
§ Non significant; Chi-square test
§§ Non significant; Fisher’s-exact test
* Significant; Paired t-test
** Significant; Unpaired t-test
***Significant; Repeated Measurement