Unilateral Connation of Primary Mandibular Lateral Incisor and Canine Associated with Missing Succedaneous Teeth: Report of a Rare Case in Siblings
Umapathy Thimmegowda1, Pavana Mysore Parameshwara2, Navin Hadadi Krishnamurthy3, Naveena Preethi4
1 Professor, Department of Pedodontics and Preventive Dentistry, Rajarajeswari Dental College and Hospital, Bengaluru, Karnataka, India.
2 Senior Lecturer, Department of Pedodontics and Preventive Dentistry, Sri Siddhartha Dental College, Agalakote, B.H. Road, Tumkur, Karnataka, India.
3 Professor, Department of Pedodontics and Preventive Dentistry, Rajarajeswari Dental College and Hospital, Bengaluru, Karnataka, India.
4 Senior Lecturer, Department of Pedodontics and Preventive Dentistry, Rajarajeswari Dental College and Hospital, Bengaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Umapathy Thimmegowda, Rajarajeswari Dental College, No.14, Ramohalli Cross, Kumbalgodu, Bengaluru-560074, Karnataka, India.
E-mail: umapathygowda@gmail.com
Connation is one of the developmental anomalies of the dental hard tissue. The terms such as double formation, double teeth, twinned teeth, synodontia, joined teeth, or fused teeth are often used to describe connation. Connation can be defined as union of two normally separated tooth germs typically leading to one tooth less than normal in the affected arch. It may be complete or incomplete. Connation in siblings are rare and probably show a hereditary aetiology. Here, we report two cases of unilateral connation of primary mandibular incisor and canine associated with missing succedaneous permanent lateral incisor in siblings along with their diagnosis and management.
Developmental anomalies, Mandible, Partial anodontia, Primary teeth
Case Report
A six-year-old male child came to the department of Pedodontics and Preventive Dentistry with a chief complaint of multiple decayed teeth. Patient previously had cleft palate and he was referred from a private hospital for the restoration of his decayed teeth. His mother gave a family history of consanguineous marriage, past dental history of surgical repair of unilateral cleft lip and palate. On physical examination, the child was detected with no abnormalities other than a surgical scar with an aesthetically unsatisfactory appearance seen in his maxillary left anterior region. The intraoral examination revealed an anterior segmental crossbite. Shovel-shaped tooth seen in mandibular right primary lateral incisor and canine region with an indentation on the labial surface extending from the incisal edge to the cervical margin [Table/Fig-1].
Segmental Crossbite with shovel-shaped tooth seen in mandibular right primary lateral incisor and canine region.

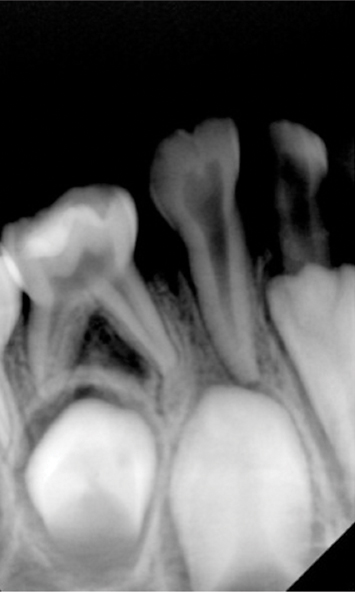
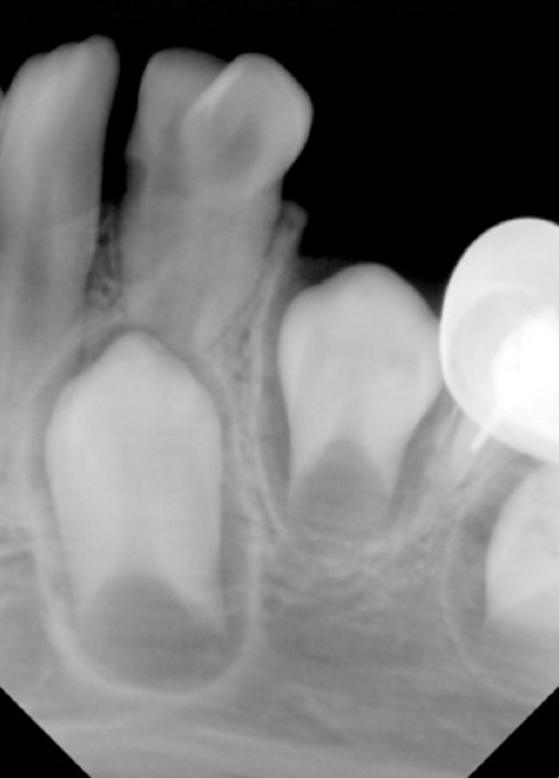
Soft tissue examination revealed presence of Bifid Uvula [Table/Fig-2]. Dental caries was evident with respect to (w.r.t) 75, 84 and 85. Restored teeth w.r.t 55 and 65 were observed. On radiographic examination the intraoral periapical radiograph revealed connated teeth w.r.t 82 and 83 with missing 42 [Table/Fig-3] and the panoramic radiograph exhibited that the crowns and roots were connated with joining of their pulp chambers and root canals in primary mandibular right lateral incisor and canine with missing permanent successor [Table/Fig-4].
Soft tissue examination showing presence of Bifid Uvula.

Intraoral periapical radiograph showing connated teeth w.r.t 82 and 83 with missing 42.
Panoramic radiograph showing connated teeth w.r.t 82 and 83 with missing 42. Restored teeth in relation to 55 and 65.

On routine clinical examination of his elder brother aged seven years nine months also had connated primary teeth with an enlarged bifid crown i.e., between 72 and 73 along with an incisal ditch extending both labially and lingually [Table/Fig-5]. Carious involvement w.r.t 54, 55, 64 and 65 was evident. Endodontically treated tooth in relation to 75 with placement of stainless steel crown and missing teeth w.r.t 84 and 85 [Table/Fig-6]. On radiographic examination, the intraoral periapical radiograph exhibited presence of connated teeth w.r.t 72 and 73 with missing 32 [Table/Fig-7] and the panoramic radiograph revealed that the enlarged bifid crown was due to connation of the crown and roots resulting in separate pulp canals [Table/Fig-6]. No other member of the family was affected by similar dental anomalies. Parents were informed about the missing teeth in both the cases. Based on all the findings both the sibling had a reduction in the number of teeth and were diagnosed with connated teeth with corresponding succedaneous missing tooth. Both the children were kept under observation and are under follow up treatment. Oral prophylaxsis was done followed by fluoride application of the fused teeth as there was no caries involvement.
Showing connated primary teeth w.r.t 72 and 73 with an enlarged bifid crown along with an incisal ditch extending labially.

Panoramic radiograph showing connated teeth w.r.t 72 and 73. Endodontically treated tooth with stainless steel crown in relation to 75 is also evident.

Intraoral periapical radiograph showing connated teeth w.r.t 72 and 73.
Discussion
Developmental anomalies of teeth are a significant category of dental morphological variations and one of the most unusual anomalies of shape of the tooth is connation [1-3].
Connation of teeth can be regarded as a developmental anomaly caused by the persistence of the dental lamina between two or more tooth germs, or by attempt of a supernumerary tooth to develop from the remnants of the dental lamina after it has divided from a neighboring tooth germ. Physical pressure leading to the union of teeth or genetic inheritance can be considered as possible aetiologies [4].
It has also been stated that connation results when two tooth germs develop so close to each other that, as they grow they come into contact and fuse before calcification [5]. Grahnen H et al., reported that connation of teeth is more common in the deciduous than in the permanent dentition with a high incidence in primary mandibular anteriors. Males are affected more than females [6].
Systemic documentation provides adequate information which is required for a precise diagnosis [7]. The early diagnosis further avoids clinical complications associated with connation and helps us to establish a proper treatment at an appropriate time. Very rarely, the anomaly has been reported in siblings of a family [8] affecting mandibular laterals and canines [9]. Anomalies of both primary and permanent dentition can be due to morphology and number of the teeth involved [10,11]. Connated tooth can be confirmed as when it appears single and the number of teeth in the dental arch are less. In the present case the number of teeth in the arch were less. The terms such as double formation, double teeth, twinned teeth, synodontia, joined teeth, or fused teeth are often used to describe connation [12]. The aetiology of connation in siblings remains unclear. A report showing double teeth with familial characteristics are very few and has a genetic background [8,9]. In the present case both the siblings had connated teeth with missing succedaneous teeth. It has been claimed that local metabolic interferences such as trauma, viral infection or genetic basis possibly autosomal dominant with reduced penetrance, environmental factors such as thalidomide embryopathy and high doses of vitamin A may induce dental fusion [1]. The prevalence of unilateral connation in the primary dentition is 0.1% to 1.5% [3]. In the present case both the male siblings were affected with the anomaly seen in mandible.
Connated teeth are frequently observed during routine oral examination. The condition of Primary Double Teeth (PDT) and their successors can be evaluated thoroughly by periapical, occlusal and panoramic radiographs [7-15]. Recent advances like Vista Scan, Cone Beam Computed Tomography (CBCT) can also be used. The classification of primary double teeth was presented in [Table/Fig-8] [14]. Herein this case report the younger brother had Type I catergory with a large crown with a notch on the incisal edge and a bifid pulp chamber, with normal dimensions of the root and radicular canal and cervical widening, whereas the elder brother had Type IV category with separate crown roots with separated pulp chambers and canals.
Showing the classification of primary double teeth.
| Types | Detail of tooth structure | Table/Figure |
|---|
| I | Bifid crown, single root: A large crown with a notch on the incisal edge and a bifid pulp chamber, with normal dimensions of the root and radicular canal and cervical widening. | 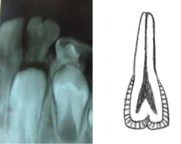 (Bifid crown and single root) (Bifid crown and single root) |
| II | Large crown, large root: A large crown, usually lacking a groove or notch, with single shared, large root canal and pulp chamber and a wider than normal root. | 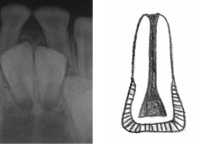 (Large crown, Large root) (Large crown, Large root) |
| III | Two fused crowns, double conical root: Two fused crowns with a partial or total vertical groove extending cervically; the crowns may be symmetrical or show distinct differences, and the pulp chambers may be separate. One large conical root. The coronal and radicular portions of the pulp canal may be fused, or the coronal portion may be shared and end in two radicular canals | 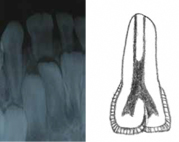 (Two fused crowns, Double conical root) (Two fused crowns, Double conical root) |
| IV | Two fused crowns, two fused roots: Two crowns (as in type III) and two distinct, joined roots with separate root canals | 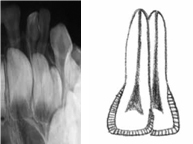 (Two fused crowns and Two fused roots) (Two fused crowns and Two fused roots) |
The clinical complications with connation include deep grooves leading to unpleasant aesthetic appearance, delayed exfoliation, occlusal disturbances, space discrepancies and agenesis of permanent successors. When there is an aesthetic issue without any underlying risk factors, reshaping of the tooth conservatively, directly bonding with composite and porcelain veneers can be used. Minimal invasive procedures can be considered if the caries is extending only into enamel and dentin. The access opening varies if the carious lesion involves the pulp when compared to normal tooth. Severe bleeding can be controlled by 2.5% sodium hypochlorite as an irrigant to ensure complete removal of voluminous pulp. Flexi files, NiTi files or S1 Protaper rotary files aids in biomechanical preparation. To compensate with the missing succedaneous teeth and to maintain the teeth in the arch obturation can be done with Zinc Oxide Eugenol (ZOE).
Two separate roots of connated tooth can be managed successfully with hemi-sectioning and restoration of one root. Custom made crowns fit the exact morphology of connated tooth. Connated tooth if grossly decayed with missing permanent successor, extraction followed by removable functional space maintainer should be the choice of treatment. Once the growth ceases and arch development is completed fixed prosthesis, implants and orthodontic rehabilitation can be planned [16].
Conclusion
To prevent the damage to the aesthetics, arch symmetry, occlusal harmony, and eruption of permanent successors connation has to be identified at the earliest stage. Its morphology could predispose to dental caries and periodontal diseases and may sometimes compromise pulp vitality. Therefore, to avoid clinical complications careful monitoring of the connation at appropriate time is recommended.
[1]. Sharma D, Bansal H, Sandhu SV, Bhullar RK, Bhandari R, Kakkar T, Fusion: a case report and review of literatureJournal of Cranio-maxillary diseases 2012 1(2):114-18. [Google Scholar]
[2]. Rao PK, Mascarenhas R, Anita A, Devadiga D, Fusion in deciduous mandibular anterior teeth – a rare caseDentistry 2014 S2:001 [Google Scholar]
[3]. Neves AA, Neves MLA, Farinhas JA, Bilateral connation of permanent mandibular incisors: a case reportInt J Paediatr Dent 2002 12(1):61-65. [Google Scholar]
[4]. Hitchin AD, Morris I, Geminated odontome: connation of the incisors in the dog, its etiology and ontogenyJ Dent Res 1966 45:575-83. [Google Scholar]
[5]. Joshi V, Pavankumar K, Ramana V, Joshi S, Saritha M, Bilateral fusion of the mandibular primary incisors: a case reportInternational Journal of Oral and Maxillofacial Pathology 2011 2(2):40-43. [Google Scholar]
[6]. Grahnen H, Granath LE, Numerical variations in primary dentition and their correlation with the permanent dentitionOdont Rev 1961 12:248-57. [Google Scholar]
[7]. Wadhawan R, Rajan P, Reddy Y, Singh A, Goel N, Jain A, Fusion of left primary mandibular lateral incisor and canine in a seven year old male child: a case reportSch J Dent Sci 2016 3(2):67-70. [Google Scholar]
[8]. Kamal R, Dahiya P, Garg A, Kumar M, Fused primary incisors in siblings: Case report and literature reviewAsian Pacific Journal of Health Science 2014 1(1):26-30. [Google Scholar]
[9]. Mukhopadhyay S, Ghosh C, Roy P, Chakraborty M, Primary double teeth in siblings: a reportSRM J Res Dent Sci 2016 7(3):187-89. [Google Scholar]
[10]. Eidelman E, Odont Fusion of maxillary primary central and lateral incisors bilaterallyPediatr Dent 1981 3(4):346-47. [Google Scholar]
[11]. Sekerci AE, Sisman Y, Ekizer A, Sahman H, Gumus H, Aydinbelge M, Prevalence of double (fused/ geminated) primary teeth in Turkey – a studyPakistan Oral & Dental Journal 2011 31(1):7-13. [Google Scholar]
[12]. Bharghava M, Chaudhary D, Aggarwal S, Fusion presenting as gemination- a Rare Case ReportOMPJ 2012 3(1):211-14. [Google Scholar]
[13]. Reddy NN, Munshi AK, Fusion of primary incisors: a report of six casesJ Indian Soc Pedod Prev Dent 1999 17(2):55-60. [Google Scholar]
[14]. Aguiló L, Gandia JL, Cibrian R, Catala M, Primary double teeth. A retrospective clinical study of their morphological characteristics and associated anomaliesInt J Paediatr Dent 1999 9(3):175-83. [Google Scholar]
[15]. Mehta V, Fusion of primary mandibular anterior teeth associated with partial anodontia of primary and permanent dentition: a case reportJ Dent health Oral Disord Ther 2015 3(3):00090 [Google Scholar]
[16]. Baratto-Filho F, Leonardi DP, Crozeta BM, Baratto SP, Campos EA, Tomazinho FSF, The challenges of treating a fused toothBraz Dent J 2012 23(3):256-62. [Google Scholar]