Introduction
Composite resins are the most frequently used direct tooth coloured restorative materials. Their use in the posterior teeth has increased because of their improved mechanical performance and wear resistance. However, marginal leakage is one of the major concerns for composite failures especially in the gingival margins of posterior teeth which leads to subsequent failure of the restoration. So, under magnification good integrity can be ensured by maintaining the ergonomics.
Aim
To compare the effect of magnification on the marginal integrity of proximal composite resin restorations.
Materials and Methods
Non-bevelled proximal slots (4.1x4x2.5) mm were prepared on the mesial surfaces of extracted mandibular first molars (N=40) for this in vitro study conducted over a period of one week in the Department of Conservative Dentistry and Endodontics at Army College of Dental Sciences, Secunderabad, Telangana, India. The teeth were randomly divided into two groups (n=20) based on the use of magnification: Group1, direct vision and Group 2, magnification with dental operating microscope. After establishing proximal contacts, the slots were restored with composite resin (Tetric N-Ceram, Ivoclar Vivadent, Mumbai, India) using a sectional matrix system (Palodent Plus Sectional Matrix System Kit, Dentsply, Caulk, US). The margins were analysed using an environmental Scanning Electron Microscope (SEM).
The data was statistically analysed using Kruskal–Wallis and Mann–Whitney U tests (p<0.05).
Results
Indicate that the difference in marginal quality of gingival margin was significantly influenced by magnified vision when compared with unaided direct vision (p<0.05). However, the difference was not statistically significant between the groups in relation to buccal and lingual margins.
Within the groups, Group 1 showed a higher percentage of gaps in gingival margins as compared to buccal and lingual margins. Whereas, in Group 2, the marginal gaps in both lingual and gingival margins were higher than buccal margins.
Conclusion
The marginal integrity of proximal composite restorations can be improved when performed under magnification.
Introduction
With the advent of minimal invasive dentistry, composite resins have been the most versatile and widely used direct restorative material.
They have continuously evolved and have been popularly used over the past few years because of their good aesthetic and physical handling properties [1].
However, inspite of their improved properties, composite resins exhibit significant disadvantages like polymerisation shrinkage, poor wear resistance, and microleakage.
Marginal leakage is a major concern for composite failure [2], especially in gingival margins of posterior composite restorations, which leads to decay and subsequent failure [3].
Various techniques such as incremental layering technique [4], use of liners [5], low shrinkage composite [6], different curing methods and use of indirect composite restorations [7] have been adapted in order to enhance the marginal integrity of composite restorations. Apart from these, refinement in the clinical application techniques and options like magnification can minimize operator related errors.
Under magnification, good integrity can be ensured as it is easier to pack a thin layer of composite material evenly against the cavity walls as well as the matrix band. Packing of the oblique layers of composite right up to the cavity margins without any excess material minimizes the finishing procedure and provides a restoration with improved physical and mechanical characteristics [8].
Magnification can be achieved by using concave mirrors, magnifying lenses, magnification loupes, intraoral camera and Dental Operating Microscope (DOM) and as compared to unaided visual examination; chances of correct diagnosis and treatment planning are higher [9].
The shadow free light provided by coaxial radiating light source and adjustable magnifications with a microscope facilitate better performance of dental procedures. In 1999, Dr Gary Carr introduced a DOM that had Galilean optics and was ergonomically configured for dentistry, especially for endodontic as well as restorative procedures.
The benefits of using the DOM and accompanying documentation systems (digital microphotography and videography) includes: refined quality and accuracy of treatment due to magnified vision, enhanced ergonomics, proper digital documentation and better ability to communicate through integrated video [10] because of which the use of the operating microscope by endodontists has increased from 52% in 1999 to 90% in 2007 [11].
Thereafter, DOM has been commonly used for examination, diagnosis of cracked teeth, complete excavation of caries, better visualization of prepared cavities and pulp chamber, locating hidden canal orifices and canals, identification and removal of obliterations, calcifications and denticles, for perforation repair, removal of fractured post and instruments, microsurgical apicoectomy and in open apex cases for root end filling [10].
In order to reduce gap formation in composite restorations in conservative non-bevelled proximal slot cavities, practical techniques to minimize operator related errors should be explored.
The aim of this study was to compare marginal integrity of direct proximal composite resin restorations performed under direct vision and DOM by evaluating the gap formation immediately after placement of the restoration.
Materials and Methods
Forty freshly extracted human mandibular first molars were selected for this in-vitro study conducted in the year 2016 in the Department of Conservative Dentistry and Endodontics at Army College of Dental Sciences, Secunderabad, Telangana, India.
The inclusion criteria were: teeth with intact crowns; teeth which were extracted due to periodontal reasons; teeth free of caries; cracks or any restorations.
The exclusion criteria were: teeth with caries; restorations; cracks; fractured crowns; attrition; abrasion; and erosion. Ethical approval was obtained from the Institutional Ethical Committee. The teeth were stored in saline solution for 30 days before starting with the study. The study was performed over a period of one week and then the samples were evaluated for marginal gaps. The teeth were divided into two groups of twenty teeth each. For standardization, mesial surfaces of the teeth were selected for cavity preparation. Group 1 (n=20) consisted of the mesial surfaces of teeth restored without magnification under direct vision and Group 2 (n=20) consisted of the mesial surface of teeth restored under magnification using DOM (600 operating microscope, Seiler, Seiler Precision Microscopes, St Louis, Missouri, USA). On the mesial surface of each tooth, standardized non-bevelled proximal slot shaped cavities were prepared with the following dimensions: proximal depth of 2.5 mm, occlusal depth of 4 mm, and buccolingual width of 4 mm using a no. 245 carbide bur (Bur Carbide FG 245, SS White, Lakewood, New Jersey) in high speed hand piece under copious amount of water. During preparation, the dimensions were measured for all cavities using a periodontal probe (GDC, CE Hoshiarpur, India) and a digital sliding caliper (PAV; Gottingen, Germany). To simplify the evaluation of marginal gaps, the cavities were further subgrouped according to the margins being studied- buccal margin (subgroup A), lingual margin (subgroup B) and gingival margin (subgroup C).
Restorative procedure: After establishing proximal contacts, using same adjacent tooth, all the samples were restored with composite resin (Tetric N-Ceram, Ivoclar Vivadent, Mumbai, India) using sectional matrix system (Palodent Plus Sectional Matrix System Kit, Dentsply, Caulk, US).
The restorations in Group 1 were performed with unaided direct vision with the tooth kept at a standard distance equal to that recommended between an operator and patient’s oral cavity [12]. The restorations in Group 2 were performed under dental operating microscope at 1.6X magnification with the tooth kept at a distance of approximately 25-35 cm from the microscope which is generally adequate for utilization of microscopy in intraoral procedures [13].
The etchant (N-Etch, 37% phosphoric acid etching gel, Ivoclar Vivadent, Mumbai, India) was applied for 15 seconds and rinsed for 10 seconds. The cavities were dabbed dry with a cotton pellet to leave the surface slightly moist. The bonding agent (Tetric N- Bond, total etch dental adhesive, Ivoclar Vivadent, Mumbai, India) was applied actively and light cured for 10 seconds (Smart LiteTM PS, Dentsply DeTrey GmbH 78467 Konstanz Germany). Composite resin restorations (Shade-A3, Tetric N-Ceram, Ivoclar Vivadent, Mumbai, India) were done using Incremental layering technique and each increment was cured for 20 seconds after which finishing and polishing was performed using polishing discs (Super-Snap Mini Kit, Shofu, Shofu Dental Corporation, San Marcos, USA).
The various factors affecting the marginal integrity such as: cavity geometry (4x4x2.5) mm, configuration factor (class II: C-factor: 2), type of composite resin: Tetric N-Ceram, Ivoclar Vivadent, Mumbai, India (nanocomposite, etch and rinse type), restorative technique (incremental layering technique), curing method: (continuous) were kept standard for both the groups.
Marginal analysis: Caries detector dye (Caries indicator, Prime dental products Pvt. Ltd., Mumbai, India) was applied on the margins of the restored cavities for five seconds, rinsed with water and then air-dried. The margins of the restorations of each sample were then observed under Measuring Microscope (Olympus STM6, Measuring Microscope, Seiler Precision Microscopes, St Louis, Missouri, USA) at 1.25 turbo X magnification [Table/Fig-1].
Measuring Microscope Images at 1.25 turbo X magnification; a) Unaided direct vision; b) DOM.
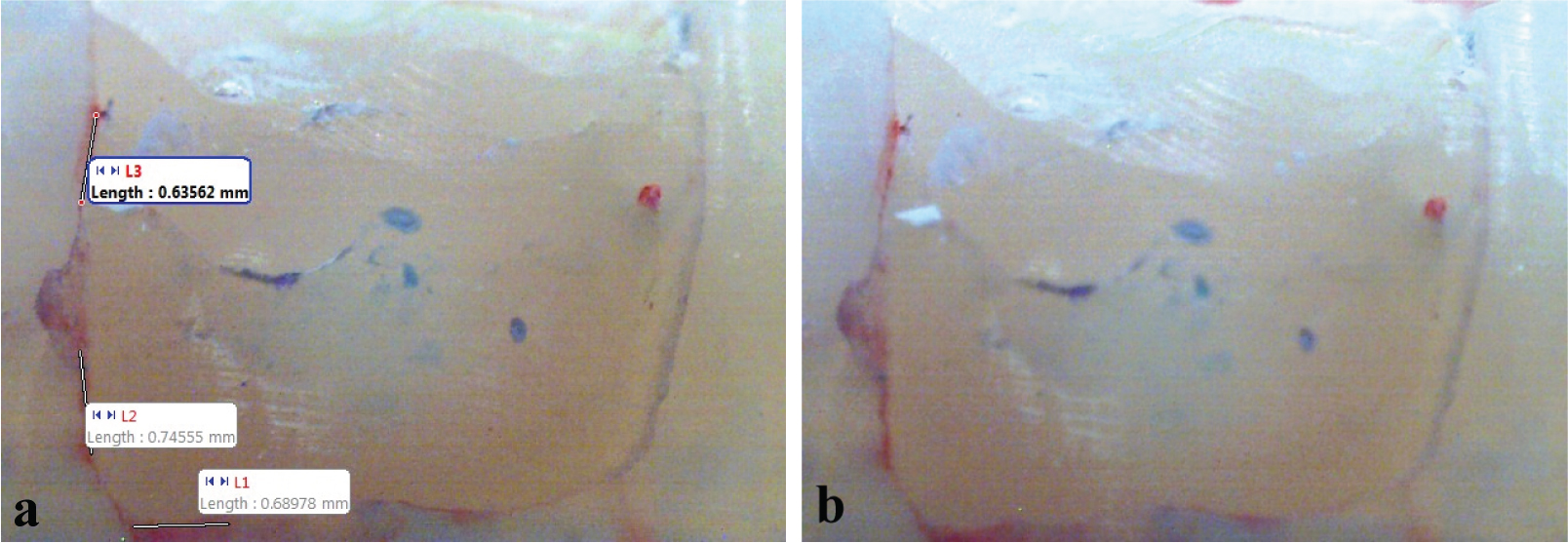
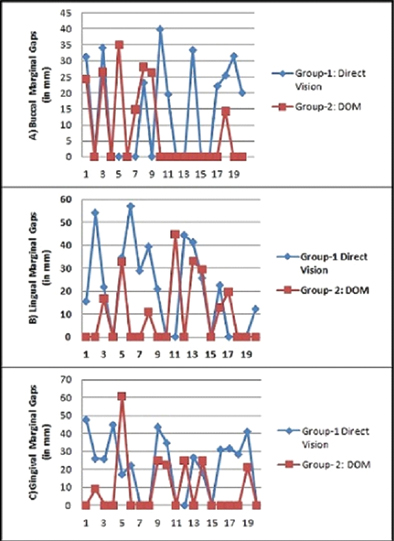
Motic Image Plus 2.0 ml Software which captures a live image by a digital camera and displays it on a monitor was used to measure lengths of the marginal gaps individually for buccal, lingual and gingival margins of each sample separately in millimetres (mm) which is frequently used to refer to any dimension of a margin of a cavity at clinical level. Graphs depicting the comparison of values of gaps (in mm) for each margin between the two groups are shown in [Table/Fig-2].
Comparison of Marginal gaps (in mm) between Group-1 and Group-2; a) Buccal margin; b) Lingual margin; c) Gingival Margin.
Percentage of Marginal Gap was calculated using the formula:
Percentage of Marginal Gap = Length of Gap/Total Length of Margin x100
The mean values for each margin were calculated and statistically analysed [Table/Fig-3].
Table showing Mean values ± Standard deviation (in %age) of Marginal gaps of the Subgroups.
| Groups (and Subgroups) | N | Mean±SD | SE | Min. | Max. |
|---|
| Group 1 (Direct vision) |
| Subgroup A (buccal margin) | 20 | 14.0320±15.16673 | 3.39138 | 0.00 | 39.96 |
| Subgroup B (lingual margin) | 20 | 20.8500±19.36983 | 4.33122 | 0.00 | 56.89 |
| Subgroup C (gingival margin) | 20 | 21.9580±16.82773 | 3.76279 | 0.00 | 47.68 |
| Total | 60 | 18.9467±17.27953 | 2.23078 | 0.00 | 56.89 |
| Group 2 (DOM) |
| Subgroup A (buccal margin) | 20 | 8.4785±12.56932 | 2.81059 | .00 | 35.07 |
| Subgroup B (lingual margin) | 20 | 9.9545±14.42647 | 3.22586 | .00 | 44.59 |
| Subgroup C (gingival margin) | 20 | 9.4050±15.88627 | 3.55228 | .00 | 60.53 |
| Total | 60 | 9.2793±14.12622 | 1.82369 | .00 | 60.53 |
(SD- Standard Deviation, SE- Standard Error, Max- Maximum, Min- Minimum.)
Statistical Analysis
The normality of data was assessed using Kolmogorov - Smirnov test. The values obtained were statistically analysed using Kruskal–Wallis test followed by Mann–Whitney U test using IBM SPSS for Windows, Version 19.0 (SPSS; Chicago, IL, USA) with the significance level set at p<0.05 to compare influence of magnified vision on the marginal integrity of proximal composite restorations.
Results
According to Kruskal Wallis analysis [Table/Fig-4] there was no significant difference between the mean values of the two groups and Mann Whitney U test [Table/Fig-5] showed that the difference was statistically significant at p=0.013 between the two groups only in relation to subgroup-C, i.e., gingival margin. Results indicate that the difference in marginal quality of gingival margin was significantly influenced by magnified vision when compared with unaided direct vision (p<0.05). However, the difference was not statistically significant between the groups in relation to buccal and lingual margins as well as between the three margins within each group.
| Groups | Total N | Mean±SD | Min. | Max. | Kruskal-Wallis test |
|---|
| X2 | p-value |
|---|
| Group-1: (Direct vision) | 60 | 18.9467±17.27953 | 0.00 | 56.89 | 2.455 | 0.293 |
| Group-2: (DOM) | 60 | 9.2793±14.12622 | 0.00 | 60.53 | 0.152 | 0.927 |
SD: Standard Deviation, Max- Maximum, Min- Minimum.
Pair wise comparison of the three margins using Mann-Whitney U test.
| Subgroups | Groups | N | Mean Rank | Mann- Whitney U | Z-value | p-value |
|---|
| (Group-1 v/s Group- 2) |
|---|
| Subgroup A(buccal margin) | Group-1 | 20 | 22.35 | 163 | -1.112 | .327 |
| Group-2 | 20 | 18.65 |
| Total | 40 | | | | |
| Subgroup B(lingual margin) | Group-1 | 20 | 23.75 | 135 | -1.861 | .081 |
| Group-2 | 20 | 17.25 |
| Total | 40 | | | | |
| Subgroup C(gingival margin) | Group-1 | 20 | 25.05 | 109 | -2.605 | .013* |
| Group-2 | 20 | 15.95 |
| Total | 40 | | | | |
*- statistically significant (p<0.05)
Total three samples in Group 2 showed no marginal gaps at all whereas only one sample gave such a result in Group 1.
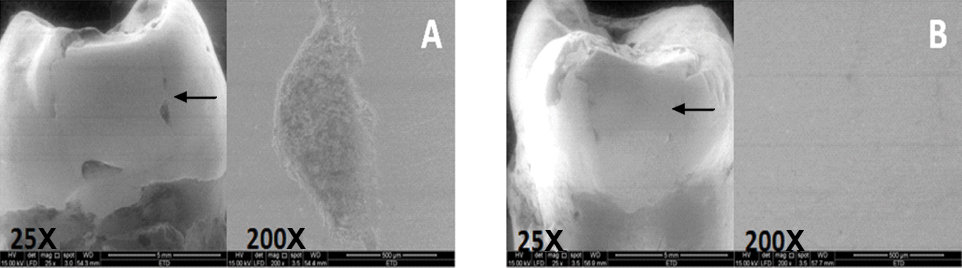
To further verify the results obtained through measuring microscope, one sample from each group was evaluated under Environmental SEM at 25X and at 200X magnifications [Table/Fig-6].
SEM images at 25X and 200X; a) Group-1; b) Group-2.
Discussion
This in vitro study was performed to assess the influence of magnification on marginal integrity of proximal composite restorations.
Marginal gap was calculated as a percentage of the entire marginal length which is in accordance with the method used in previous studies [5,14] as this method aids in evaluating the margins of restoration quantitatively as well as qualitatively.
The results showed that percentage of marginal gaps were higher in the restorations performed with unaided direct vision (Group-1) as compared to restorations performed under DOM (Group-2). As suggested by J. Mamoun, dentist’s ability to prepare, bond, restore and adjust composite restorations might be improved with use of microscope level magnification combined with coaxial illumination (MLMCI) in comparison to use of unaided vision and non-coaxial shadow forming over head lighting [15].
According to the present study, gingival margins showed higher percentage of gaps as compared to buccal and lingual margins in Group 1. This is in accordance with the results seen by Nadig RR et al., where in microleakage was significantly higher in the gingival margins in comparison to the occlusal margins of class II composite restorations [4]. In a study by Campos EA et al., the marginal gaps were higher in cervical margins as compared to proximal and occlusal margins in proximal restorations performed with different types of bulk fill composite resins [16]. Similarly greater microleakage occurred along the gingival margin than the axial wall as observed by Miletic V et al., while comparing bulk fill, low-shrinkage and conventional composites [17]. The above mentioned studies in which the gingival margins showed more gaps as compared to occlusal/ buccal/lingual margins were performed under direct vision.
In Group 2 lingual and gingival margins showed comparable range of gaps and were higher than buccal margins. However, least number of samples showed marginal gaps compared to Group 1 at all margins.
Reason for the better results obtained in Group 2 could be that magnification aids in better visualization of the microscopic gaps in the matrix band seal, stabilization and adaptation of the band gingivally with a wedge which improves the interproximal contact and contours, better condensation thereby improving the seal. An unconstrained volumetric shrinkage of 2.5% has been demonstrated due to improperly condensed composite resin material [18]. A magnified view helps in proper condensation of composite into all aspects of the preparation by aiding in adjustments of the angle and direction of instrument working tip which directs composite into the required direction [15]. Also, clinical research studies indicate that for well controlled insertion techniques, only 3% incidence of secondary caries was seen after 10 years [19].
In the present study, statistically significant difference was observed with the gingival margin between the two groups because the gingival margins are the most inaccessible areas with direct vision as compared to dental operating microscope which yields a better visualisation of the preparation, adaptation of the band and restoration of the tooth with increased precision in an ergonomic position [13]. On the contrary, buccal and lingual margins more or less have comparatively better access and visibility in both the groups due to which the statistically insignificant difference is observed.
Limitation
In the present study, only composite restorations were evaluated. The quality of margins may be different for different materials and bonding systems.
The margins under scanning electron microscope are best studied by making epoxy resin replicas of the samples. However, in this study, the marginal gaps were measured by directly observing the tooth samples under the SEM.
Conclusion
The present study showed that the use of a dental operating microscope improved the marginal integrity of proximal composite restorations. Hence, the clinical studies or tutorials should routinely incorporate magnification in training students to perform high quality composite resin restorations.
(SD- Standard Deviation, SE- Standard Error, Max- Maximum, Min- Minimum.)
SD: Standard Deviation, Max- Maximum, Min- Minimum.
*- statistically significant (p<0.05)
[1]. Willems G, Lambrechts P, Braem M, Vanherle G, Composite resins in the 21st centuryQuintessence Int 1993 24(9):641-58. [Google Scholar]
[2]. Hickel R, Manhart J, Longevity of restorations in posterior teeth and reasons for failureJ Adhes Dent 2001 3(1):45-64. [Google Scholar]
[3]. Mjör IA, The location of clinically diagnosed secondary cariesQuintessence Int 1998 29(5):313-17. [Google Scholar]
[4]. Nadig RR, Anupriya B, Usha G, Karthik J, Rao R, Vedhavathi B, Effect of four different placement techniques on marginal microleakage of class II composite restorations: an in vitro studyWorld J Dent 2011 2(2):111-16. [Google Scholar]
[5]. Alonso RC, Cunha LG, Correr GM, Puppin-Rontani RM, Correr-Sobrinho L, Sinhoreti MA, Marginal adaptation of composite restorations photoactivated by LED, plasma arc, and QTH light using low-modulus resin linersJ Adhes Dent 2006 8(4):223-28. [Google Scholar]
[6]. Yamamoto T, Hanabusa M, Momoi Y, Sakaguchi RL, Polymerization stress of dental resin composite continues to develop 12 hours after irradiationJ Esthet Restor Dent 2015 27(1):44-54. [Google Scholar]
[7]. Bortolotto T, Onisor I, Krejci I, Proximal direct composite restorations and chairside CAD/CAM inlays: marginal adaptation of a two-step self-etch adhesive with and without selective enamel conditioningClin Oral Investig 2007 11(1):35-43. [Google Scholar]
[8]. Terry DA, Restoring the interproximal zone using the proximal adaptation technique-Part 2Compend Contin Educ Dent (Jamesburg, NJ: 1995) 2005 26(1):11-12. [Google Scholar]
[9]. Erten H, Üçtasli MB, Akarslan ZZ, Uzun Ö, Semiz M, Restorative treatment decision making with unaided visual examination, intraoral camera and operating microscopeOper Dent 2006 31(1):55-59. [Google Scholar]
[10]. Das UK, Das S, Dental operating microscope in endodontics-a reviewIOSR-JDMS 2013 5(6):1-8. [Google Scholar]
[11]. Kersten DD, Mines P, Sweet M, Use of the microscope in endodontics: results of a questionnaireJ Endod 2008 34(7):804-07. [Google Scholar]
[12]. Wilder AD, Preliminary considerations for operative dentistry. In: Roberson, editorSturdevant’s Art and Science of Operative Dentistry 2006 5th edUnited StatesSt. Louis Mosby Publishers:449-92. [Google Scholar]
[13]. Khayat BG, The use of magnification in endodontic therapy: the operating microscopePract Periodontics Aesthet Dent 1998 10(1):137-44. [Google Scholar]
[14]. El-Marhomy AM, Genaid TM, Abdalla AI, Effect of different configuration factors on marginal gap formation of two composite resin systemsTanta Dent J 2013 10(3):160-67. [Google Scholar]
[15]. Mamoun J, Preparing and restoring composite resin restorations. The advantage of high magnification loupes or the dental surgical operating microscopeN Y State Dent J 2015 81(4):18-23. [Google Scholar]
[16]. Campos EA, Ardu S, Lefever D, Jassé FF, Bortolotto T, Krejci I, Marginal adaptation of class II cavities restored with bulk-fill compositesJ Dent 2014 42(5):575-81. [Google Scholar]
[17]. Miletic V, Peric D, Milosevic M, Manojlovic D, Mitrovic N, Local deformation fields and marginal integrity of sculptable bulk-fill, low-shrinkage and conventional compositesDent Mater 2016 32(1):1441-51. [Google Scholar]
[18]. Vyver PVD, New clinical innovations and the benefit of magnification to ensure predictable posterior composite restorations–Part 2International Dentistry – African Edition 2011 2(1):4-18. [Google Scholar]
[19]. Bayne SC, Thompson JY, Biomaterials. In: Roberson, editorSturdevant’s Art and Science of Operative Dentistry 2006 5th edUnited StatesSt. Louis Mosby Publishers:135-242. [Google Scholar]