Hysterectomy is the second most frequently performed major surgery on women globally, next only to caesarean [1,2]. In recent years, for hysterectomy too, the fast-track perioperative program which primarily was used for gastrointestinal surgery cases [3], has been tried with encouraging outcome [4,5]. Fast-track perioperative program is a multimodal rehabilitation program to decrease convalescence time after surgery. It is a combo-pack of adequate preoperative information and counselling, optimal postoperative pain control, and aggressive postoperative rehabilitation, including early oral feeding and ambulation. This approach seems to have revolutionized the postoperative recovery; thus effectively reducing the hospital stay and patient satisfaction.
In the present study, we tried to analyse the effect of one more component (i.e- spinal anaesthesia versus general anaesthesia) during hysterectomy for benign gynaecological conditions to further hasten the postoperative recovery and evolve the concept.
Materials and Methods
This prospective study was conducted in the Department of Obstetrics and Gynaecology, in a tertiary care hospital affiliated to a Medical School, from November 2012 to August 2014. Study protocol was approved by the institutional ethical committee (IEC 479/2012). Based on a previous study comparing the mode of anaesthesia, anticipating postoperative pain to be 50% less in spinal anaesthesia as compared to general anaesthesia with 80% power at 95% Confidence Interval (CI), sample size of 42 in each group was required. Women who were planned for abdominal hysterectomy for benign gynaecological conditions were recruited. We conducted a counselling session for all these patient on one to one basis, where patients were educated regarding the concept of fast-track hysterectomy and related advantages with the help of printed information leaflets. Patients were given the choice to be able to choose either general or spinal anaesthesia after explaining the expected pros and cons of both.
Unlike our routine protocol no sedative premedication was prescribed to those women who were included in the study. All patients were kept nil per orally from midnight of the day prior to the surgery. As per the predecided plan for individual patient based on the consensus from the patient, the anaesthesiologist and the incharge gynaecologist general or spinal anaesthesia was administered.
Details of anaesthesia: In spinal anaesthesia group, patient received 0.5% heavy bupivacaine with buprenorphine and desired level of blockade was achieved with use of 25 gauge needle. In general anaesthesia group, patients have received intravenous Fentanyl (2-3mg/kg body weight), propofol (2-3mg/kg body weight) and vecuronium (0.1mg/kg body weight). Intubation done with direct laryngoscopy and appropriate endotracheal tube positioned. Anaesthesia maintained with oxygen/nitrous oxide/isoflurane/vecuronium intravenous as and when required. In cases where spinal anaesthesia was inadequate, it was converted to general anaesthesia. But these cases then were excluded from the study.
During the surgery duration (skin to skin), blood loss or any complications (if happened) were noted. All surgeries were performed by either of the two authors with almost equal level of surgical competence.
Postoperatively, all the patients were monitored for pain, vomiting, drowsiness and fatigue. Postoperative pain was managed with intravenous administration of paracetamol (1 gram) every six hours and use of opioids was minimised (adding it only if required). Pain intensity was measured on Visual Analogue Scale (VAS) ranging from 0 to 10, with 0 indicating no pain and 10 indicating the worst pain [6]. On patient’s request, if pain was intolerable in spite of injection paracetamol, injection diclofenac 50 mg intramuscularly was administered. If pain still persisted, injection pethidine 50 mg intramuscularly was administered.
Preventive strategy was adopted for the management of postoperative vomiting by the administration of ondansetron (5HT3 receptor antagonist) or metoclopramide, with the first complaint of nausea.
All patients were encouraged for early oral intake (after confirming the bowel sounds on auscultation) and early ambulation. Transurethral urinary bladder catheter was removed after 24 hours. Patient was instructed to take soft diet and mobilization was actively encouraged. Time of first bowel movement was noted. Patient received combination of paracetamol and diclofenac orally during hospitalization. Postoperative complications and duration of hospital stay were noted. The criteria for discharge of patients were mobilization of the patient, tolerance to normal diet, sufficient pain relief with oral analgesics (VAS<4). Subjective assessment of fatigue at 12h, 24h, 36h and 48h was also done. If patient residence was more than 100km from the hospital, these women were discharged after suture removal.
Statistical Analysis
SPSS version 16.0 was used. Differences in continuous variables were analysed with student’s t-test for normally distributed data and the Mann-Whitney U Test for skewed data. Pain score was analysed by repeated measures of ANOVA. CI 95% was applied wherever it was appropriate. Two tailed p<0.05 was considered statistically significant.
Results
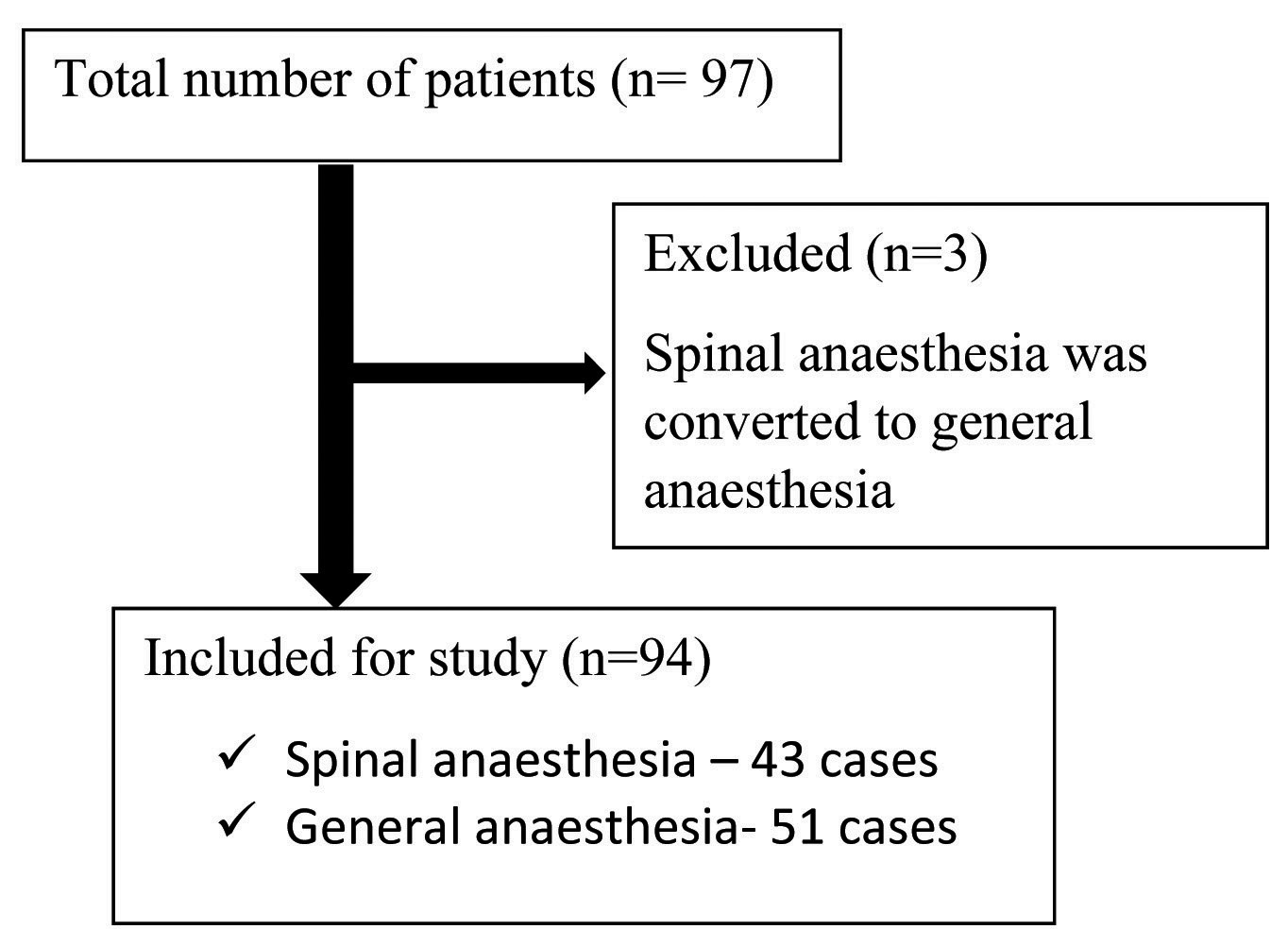
A total of 97 women were recruited for the study, wherein 46 opted for spinal anaesthesia and 51 for general anaesthesia. Three cases had to be excluded, which belonged to spinal anaesthesia group but because of inadequate result was converted into general anaesthesia. Thus, for final analysis we took into consideration only 94 cases (spinal anaesthesia: 43, general anaesthesia: 51). [Table/Fig-1].
Mean age of women who underwent abdominal hysterectomy under spinal anaesthesia (45.35±6.32 years) was comparable with that in general anaesthesia group (45.69±7.29 years). Mean BMI in the two groups were also comparable (spinal anaesthesia: 24 kg/m2, general anaesthesia: 24 kg/m2). In the spinal anaesthesia group 34 women (79.07%) belonged to American Society of Anaesthesia (ASA) class-1 (www.asahq.org) and in the general anaesthesia group also 36 women (70.58%) were in the same group. In the general anaesthesia group, 17% had previous history of laparotomy and one of these had undergone three caesarean sections previously [Table/Fig-2]. The most common symptom for hysterectomy was symptomatic fibroid uterus (spinal anaesthesia: 58.14%, general anaesthesia: 68.71%).
Demographic characteristics of the population studied.
| Characteristics | General Anaesthesian=51 | Spinal Anaesthesian=43 | T-testp-value |
|---|
| Age (years) | Mean(SD) | 45.69 (7.29) | 45.35 (6.32) | 0.227 |
| Median(range) | 44 (35-66) | 45 (35-67) |
| Parity {Median (range)} | 2 (0-7) | 2 (0-7) | |
| Body mass index (kg/m2)Mean± SDNormal (<25)Overweight (25-30)Obese 1(30-35)Obese 2(35-40) | 26.37±4.4524 (47.05 %)17 (33.33 %)09 (17.65 %)01(1.96 %) | 24.56± 4.4524 (55.81 %)16 (37.3 %)03 (6.97 %)00 | 0.333 |
| American Society Anaesthesia (ASA):*Class 1Class 2 | 36(70.58 %)15(29.42 %) | 34(79.07 %)9(20.93 %) | 0.242 |
| Previous operationsOne LSCSTwo LSCSThree LSCSOvarian cystectomy(Laparotomy) | 9 (17.64 %)5211 | 6 (13.9 %)5001 | |
*As per the guidelines of American Society Anaesthesia (ASA); www.asahq.org
[Table/Fig-3] compares the mean operating time, anaesthesia time and estimated blood loss in the two groups. We observed that the mean operating time in the spinal anaesthesia group, was much less (92.72±23.6 minutes) than in the general anaesthesia group (124.20±33.6 minutes), and this difference was statistically significant (p<0.001). On further analysis, it was found that the operative time was observed to be long in those women with BMI >30kg/m2. Mean blood loss was also less in the spinal anaesthesia group (298.14±61.3 ml versus 404.90±110.5 ml; p<0.001).
Comparison of intraoperative variables among the two groups.
| Characteristics | General Anaesthesian= 51 | Spinal Anaesthesian= 43 | T testp-value | 95% CI |
|---|
| Mean ± SD | Median(range) | Mean ± SD | Median(range) |
|---|
| Operating time** (minutes) | 124.20±33.61 | 120 (60-195) | 92.72±23.61 | 90 (60-150) | <0.001* | -43.59 to19.35 |
| Anaesthesia time*** (minutes) | 152.33±33.76 | 150 (90-230) | 115.26±25.5 | 110 (75-180) | <0.001* | -49.52 to 24.6 |
| Estimated blood loss (ml) | 404.90±110.57 | 400 (200-600) | 298.14±61.34 | 300 (150-400) | <0.001* | -144.3 to -69 |
**Time from skin incision to skin closure
*** Time from start of anaesthesia to extubation (GA) or leaving the operating room (SA)
Size of the uterus was statistically comparable among the two groups. In spinal anaesthesia group, 14/43 (32.55%) patients had size of uterus more than 12 weeks, and one patient’s uterus size was 22 weeks. In general anaesthesia group, 17/51 (33.33%) patient’s uterus size was more than 12 weeks, and eight patients had uterus of more than 20 weeks. Ex-vivo all uteri were weighed immediately following their removal. Median weight of the uterus in the spinal anaesthesia group was 175 grams (range 50-800 grams) while in general anaesthesia group it was 200 grams (range 50-950 grams).
As per the protocol, oral sips were started after bowel sounds were heard. As bowel sounds were heard earlier in the spinal anaesthesia group, oral fluids could be started earlier in the spinal anaesthesia group. Only 2/43 patients received oral sips before six hours of operation. However, none of the patients in general anaesthesia group received oral sip before six hours as bowel sounds were not heard.
Time to first bowel movement was a mean of 34 hours in the spinal anaesthesia group, which was significantly shorter than 43 hours in the general anaesthesia group. This might be explained by the need of less opioid during immediate postoperative period.
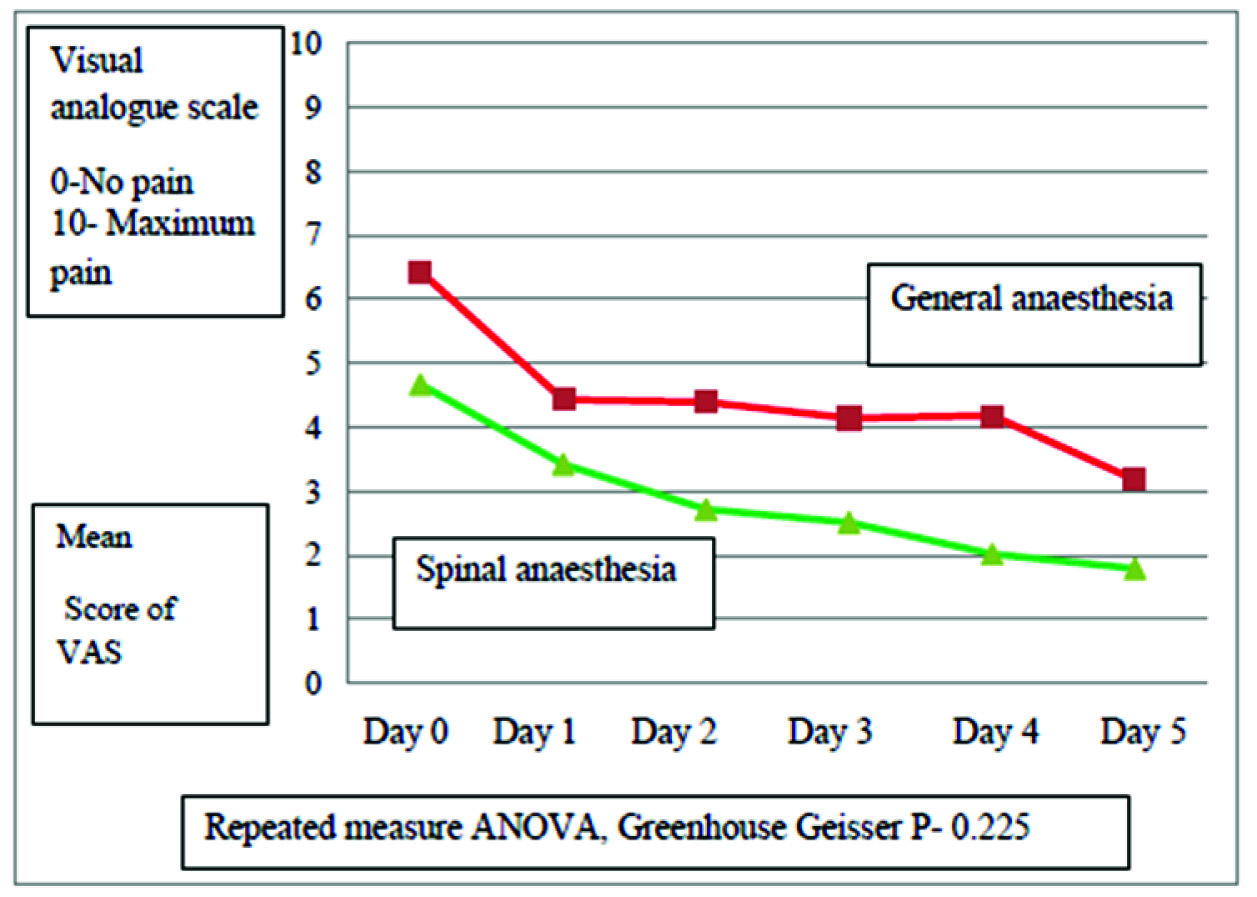
[Table/Fig-4] represents pain intensity after abdominal hysterectomy during the first five days after surgery. It is evident from the graph that the pain scores were throughout less in the spinal anaesthesia group. However, the difference in pain scores was not statistically significant (p-value: 0.225) among the two groups. In the general anaesthesia group 20/51 (39.2%) patients received 50 milligrams of injection diclofenac and 18/51 (35.3%) patients received 100 milligrams of diclofenac as add back analgesia. Comparative number of women in the spinal anaesthesia group (15/43, i.e., 34.89%) required 50 milligrams of diclofenac. However, only 6/43 (14%) patients received 100 milligrams of diclofenac on immediate postoperative day. This difference was also not statistically significant.
Comparison of Pain Scores for the first five days in the two groups.
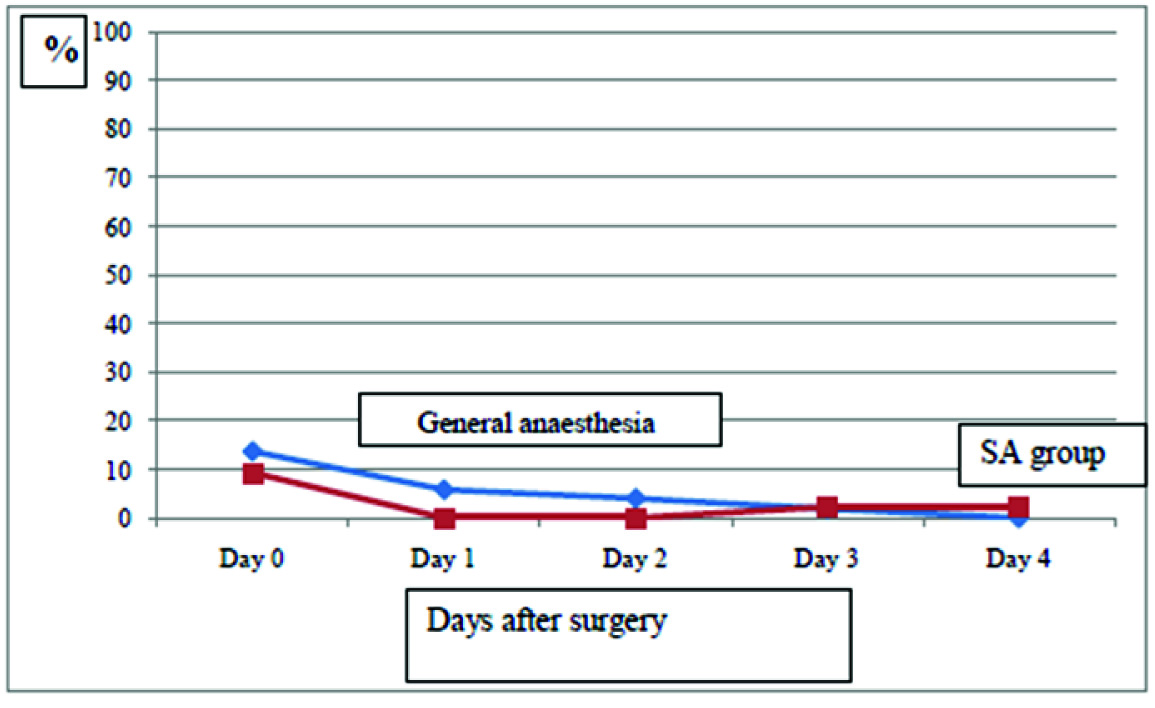
We observed that vomiting occurred more often in general anaesthesia group compared to spinal anaesthesia group during first three days after surgery [Table/Fig-5].
Incidence of vomiting in the two groups during the first 3 days following surgery.
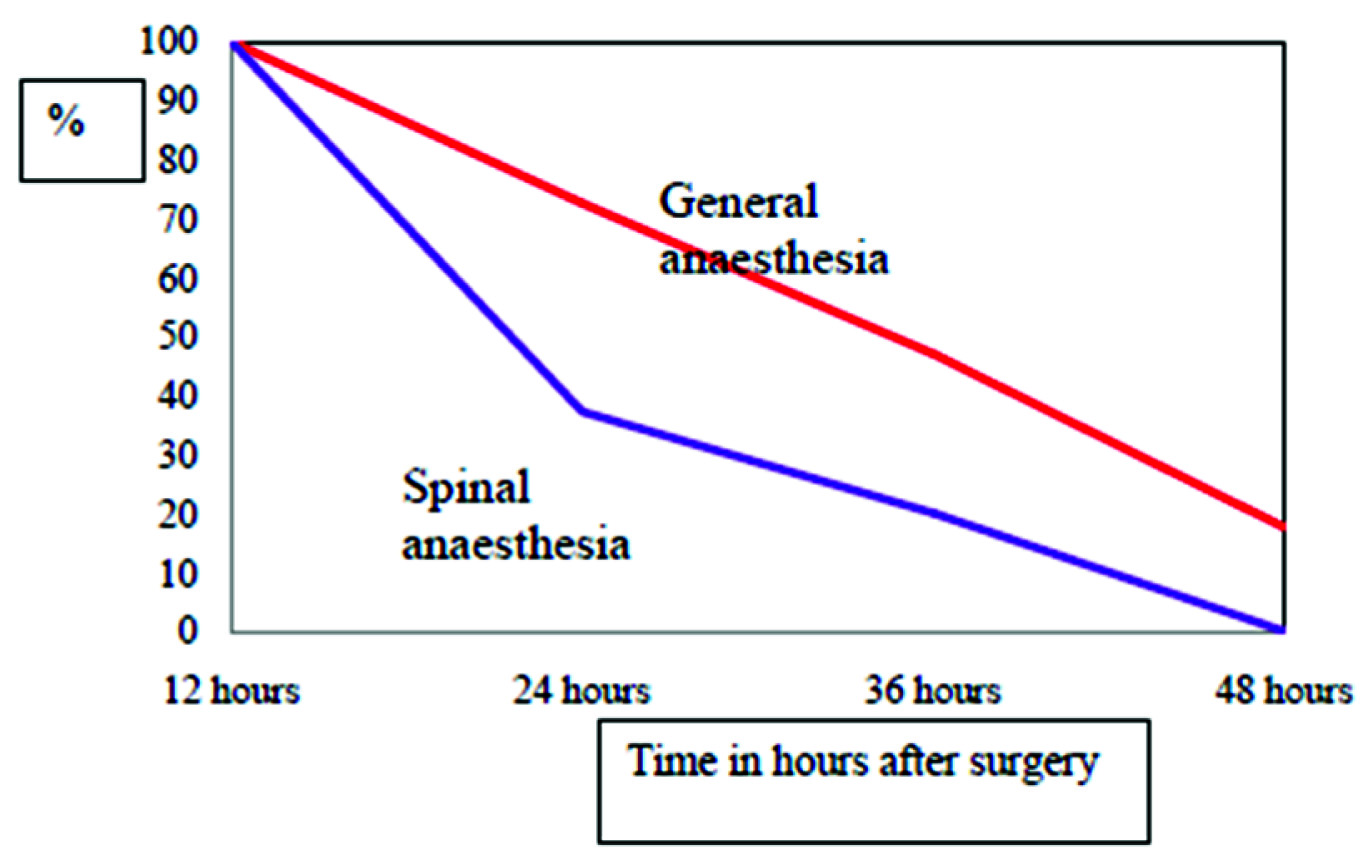
One more interesting view which we came across during the study was the prevalence of fatigue, which was a subjective symptom. [Table/Fig-6] represents fatigue at end of 24 hours, 16 out of 43 patients (37%) in spinal anaesthesia group complained of fatigue which was less compared to general anaesthesia group (37/51 patients, 72.5%). After 48 hours, none of the patients in spinal anaesthesia group complained of fatigue but in general anaesthesia group, nine patients still complained of fatigue.
Prevalence of fatigue in the two groups, postoperatively.
The rate of postoperative complications was low in our study population. In general anaesthesia group, three patients developed wound infection and one had secondary haemorrhage [Table/Fig-7]. One interesting observation we noted that patient in the general anaesthesia group had much higher incidence of postoperative cough (47.05%) as compared to spinal anaesthesia group where only 8/43 (18.60%) had postoperative cough. This difference was statistically significant (p<0.001). All complications were managed conservatively.
Comparison of postoperative complications among the two groups.
| Complications | General Anaesthesian=51 (%) | Spinal Anaesthesian=43 (%) | p-value |
|---|
| Wound infection | 3 (5.88) | 0 | |
| Secondary haemorrhage | 1(1.96) | 0 | |
| Urinary tract infection | 0 | 0 | |
| Febrile morbidity | 0 | 0 | |
| Deep vein thrombosis | 0 | 0 | |
| Postoperative cough | 24 (47.05) | 8 (18.60) | <0.001* |
[Table/Fig-8] summarises the postoperative hospital stay and time of resumption of daily activities in our study population. After abdominal hysterectomy under spinal anaesthesia 33/43 (76.74%) patients and in general anaesthesia group 27/51 (53%) patients were found to be fit for discharge at the end of fifth postoperative day. However, only 12/43 (27.9%) patients and 14/51 (27.45%) patients in respectively in the two group were discharged before fifth postoperative day, as patients were feeling insecure to get discharge early, being from far of places. Women in spinal anaesthesia group resumed their house work after 15 days of surgery which was significantly less compared to general anaesthesia group (18 days) (p<0.001). None of the patients were readmitted in both the group.
Discharge from the hospital and resumption of daily activities in the two groups.
| Characteristics | General Anaesthesia(n=51) | Spinal Anaesthesia(n = 43) | IndependentT testp-value | 95% Cl |
|---|
| Mean ± SD | Median (range) | Mean ± SD | Median (range) |
|---|
| Duration of hospital stay (days) | 7.10±2.47 | 6(4-15) | 6.05±1.09 | 6(4-9) | 0.011 | -1.861 to 0.24 |
| Resume of house work (days) | 18.55±4.25 | 20 (10-30) | 15.47±2.77 | 15 (10-25) | <0.001 | -4.58 to 1.58 |
Discussion
The idea of fast-track surgery using multimodal approach to hasten the postoperative recovery was conceptualized and promoted by Professor Kehlet in 1990s [7]. In the beginning it was used for colorectal surgeries. Recently this approach has gained popularity among the gynaecologist too.
Our study compared the choice of anaesthesia (spinal versus general) for benign hysterectomy in a fast-track model. We observed that in spinal anaesthesia, the anaesthesia time, operative time, blood loss was less. Women in this group could be started on oral fluids earlier, had less vomiting and fatigue postoperatively, and passed motion earlier. Though the hospital stay was comparable and women in spinal anaesthesia group resumed their routine activities earlier.
The only similar study (GASPI study group) comparing the two anaesthesia in fast-track setting for hysterectomy also couldn’t find a difference in hospital stay, but concluded that the need of add up analgesia was less in the spinal group, as was the faster bowel function recovery [8]. One negative point against spinal anaesthesia is some studies were that in the immediate postoperative period or the first day these patients complained of more vomiting episodes. Spinal anaesthesia was found to be associated with a higher prevalence of postoperative itching too [8,9]. This might be because of the use of intrathecal morphine with spinal anaesthesia. In our study we did not combine intrathecal morphine with spinal anaesthesia and may be this was the reason that we did not have this problem.
A study comparing the two anaesthesia in the same fast-track model found that the total costs (hospital costs plus cost-reduced productivity costs) were lower for the spinal anaesthesia group. Women in this group also had a faster recovery that was measured by health-related quality of life and quality adjusted life-years gained in the first postoperative month [10]. In our study cohort, there were multiple bias as patient’s wish to stay for a longer duration in the hospital, variations in the type of wards (general or special) they were admitted, so cost effective analysis was not possible. Other investigators have also realized that the calculations to compare the cost effectiveness in such protocols are complex and need too many issues to be taken into consideration [11].
A higher incidence of postoperative complication like minor infections and problems with wound healing was observed in a fast track setting [12]. In our setup we did not find any such correlation. However as other studies, obesity (BMI> 30 kg/m2) was associated with increased operative time [12,13]. An interesting finding which has not been analysed before in the literature was noticed in our study. The incidence of postoperative cough was more than 2.5 times higher in cases of general anaesthesia group. This might be due to the epithelial trauma sustained in the process of intubation which caused throat irritation. As every episode of cough increases the intra-abdominal pressure leading to operative site pain, it definitely increases the morbidity and postoperative recovery.
Limitation
First one was that it was not a randomized controlled trial. After recruitment patients were allowed to choose which anaesthesia they would prefer that might have led to some bias. The second issue to be noted was that our hospital is a tertiary care centre and patient comes from far off places, so even if they are fit to be discharged on postoperative day three, they were not willing for early discharge because of the fear of travelling a long distance in early postoperative period. Owing to this, hospital stay could not be properly analysed in the groups.
Conclusion
Spinal anaesthesia should be considered in cases who are planned for hysterectomy under fast-track setting to optimise the results. It encourages early oral intake and early ambulation, decreases the need of analgesic medication, causes less postoperative vomiting and fatigue. As a result, the basic idea of early discharge and resumption of activities is reinforced with the use of spinal anaesthesia in fast-track setting.
*As per the guidelines of American Society Anaesthesia (ASA); www.asahq.org
**Time from skin incision to skin closure
*** Time from start of anaesthesia to extubation (GA) or leaving the operating room (SA)