Sinonasal Neuroendocrine Carcinoma in a Young Female – A Case Report
Divya Radhakrishnan1, Nilambur Kovilakam Supriya2, K Rajasree Varma3
1 Senior Resident, Department of Pathology, Government Medical College, Kozhikode, Kerala, India.
2 Professor and Head, Department of Pathology, Government Medical College, Manjeri, Kerala, India.
3 Senior Resident, Department of Pathology, Government Medical College, Kozhikode, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Divya Radhakrishnan, Moolasseril Veedu, Kalanjoor Post Office, Pathanamthitta-689694, Kerala, India.
E-mail: divyarlakshmi@gmail.com
Sinonasal Neuroendocrine Carcinoma (SNEC) is a very rare malignancy which is difficult to differentiate from other nasopharyngeal malignancies due to similar morphological characteristics and small biopsy specimen. We report the case of a 35-year-old female who presented with nasal obstruction and recurrent epistaxis. Histopathological examination along with immunohistochemistry for neuroendocrine markers is required for accurate diagnosis.
Epistaxis, Immunohistochemistry, Nasopharyngeal malignancy
Case Report
A 35-year-old female presented with complaints of left sided nasal obstruction and recurrent epistaxis of six months duration. Physical examination revealed a yellowish white mass in the left nasal cavity which seemed to arise from lateral wall with soft consistency, mobile and sensitive to touch. However, it did not bleed on touch. There were no palpable cervical lymph nodes.
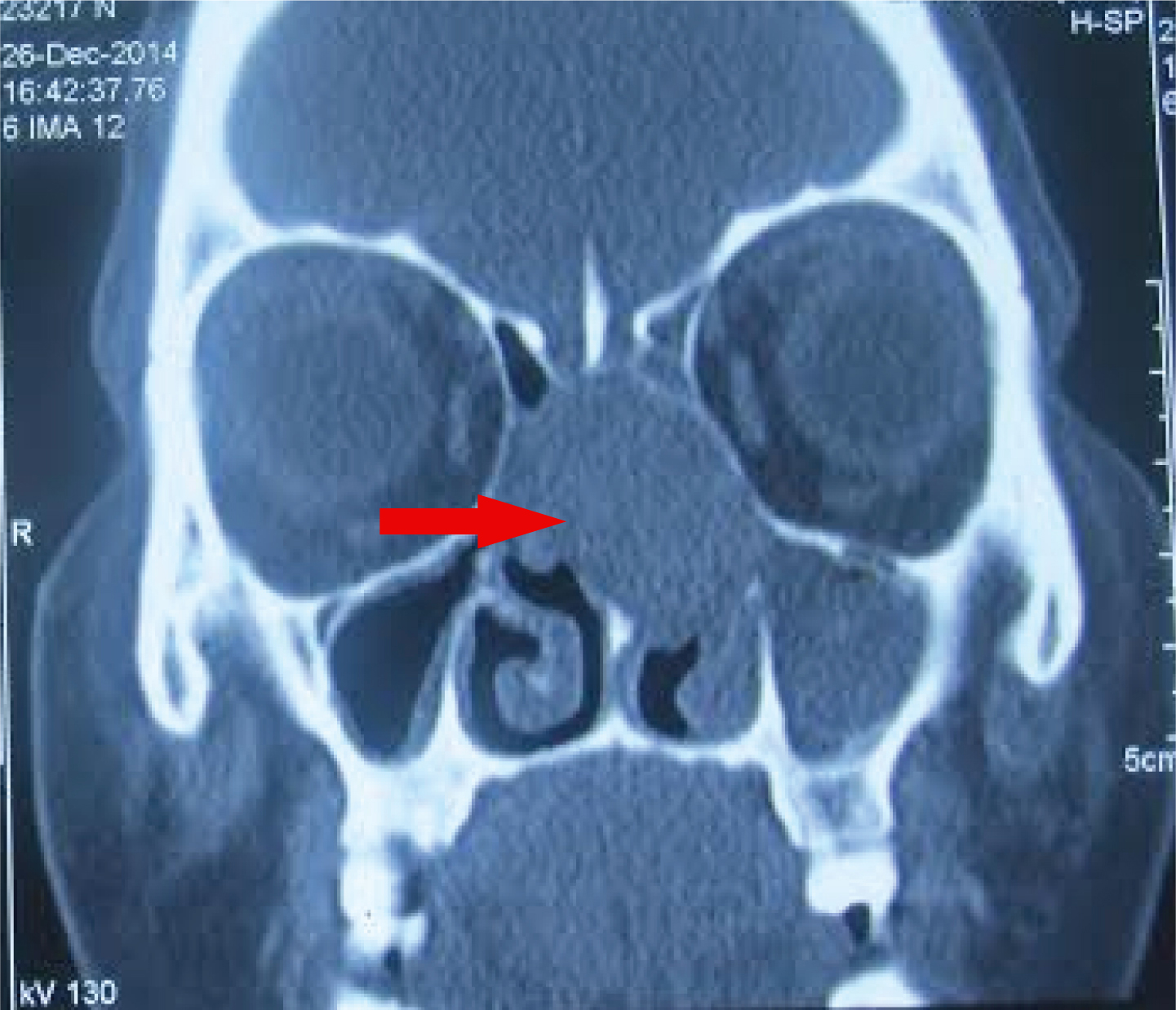
Computed Tomography (CT) study revealed mild deviation of nasal septum with well-defined lobulated soft tissue density mass lesion filling left ethmoidal, frontal and maxillary sinuses and extending into left half of nasal cavity through widened maxillary ostia [Table/Fig-1]. It was also extending through posterior nasal choana into nasopharynx. The patient underwent endoscopic biopsy of the mass and we received multiple bits of grey brown and blackish soft tissue. The specimen was fixed in formalin, routinely processed, embedded in paraffin, 5 μm thick sections cut and stained with Haematoxylin and Eosin (H&E).
CT image showing a well defined lobulated soft tissue density mass lesion filling left ethmoidal & maxillary sinuses.
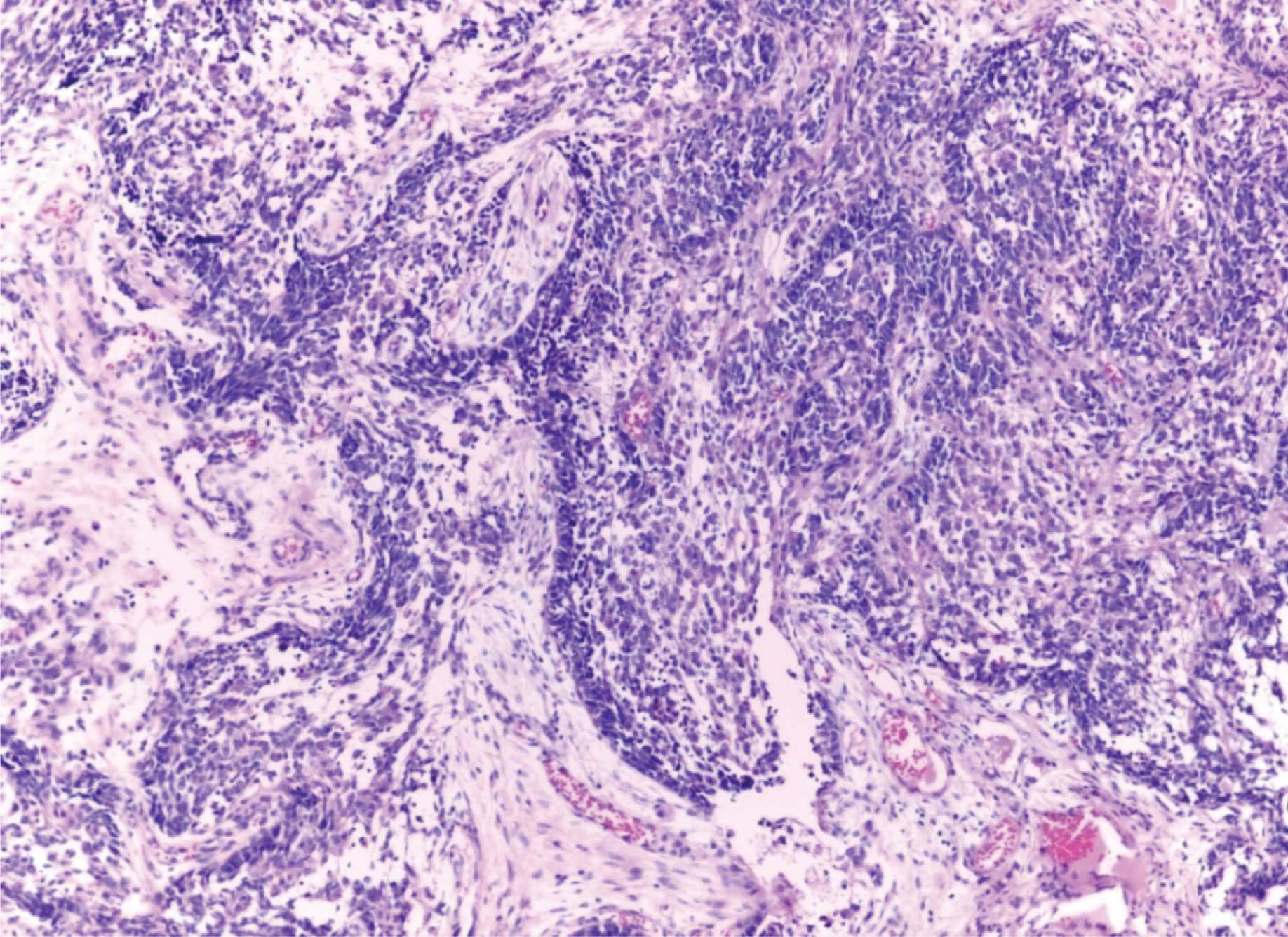
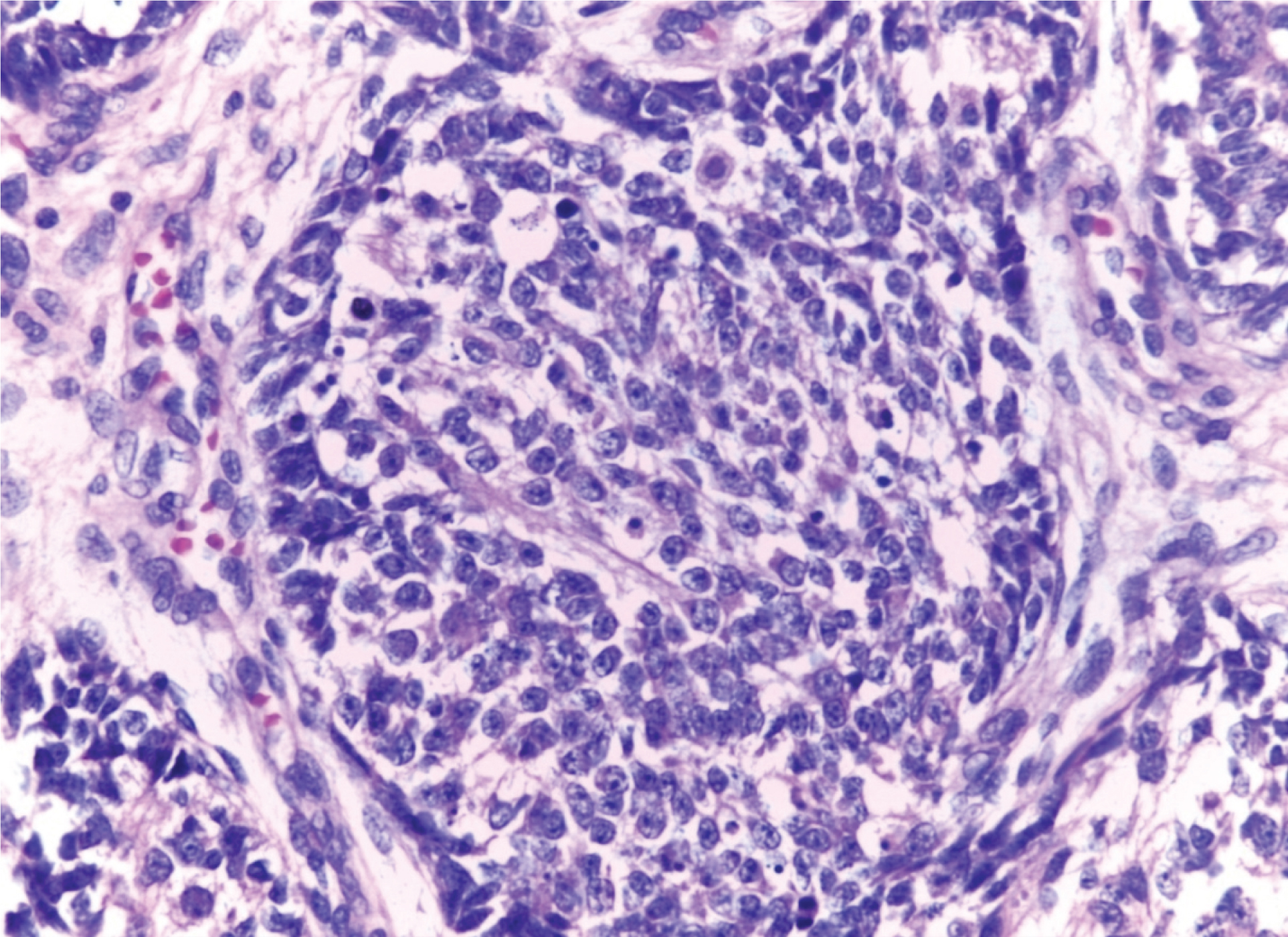
On histological examination, the tumour was characterized by sheets and ribbons of large, round cells with moderate amounts of eosinophilic cytoplasm and large, round nuclei with vesicular chromatin and many showing prominent nucleoli [Table/Fig-2,3]. Mitotic figures and apoptotic bodies were seen. There was no significant pleomorphism and tumour did not show any nests, rosettes or neurofibrillary stroma.
Sheet of tumour cells (H&E 20X).
High power view of the tumour showing mitotic figures and apoptotic bodies (H&E 40X).
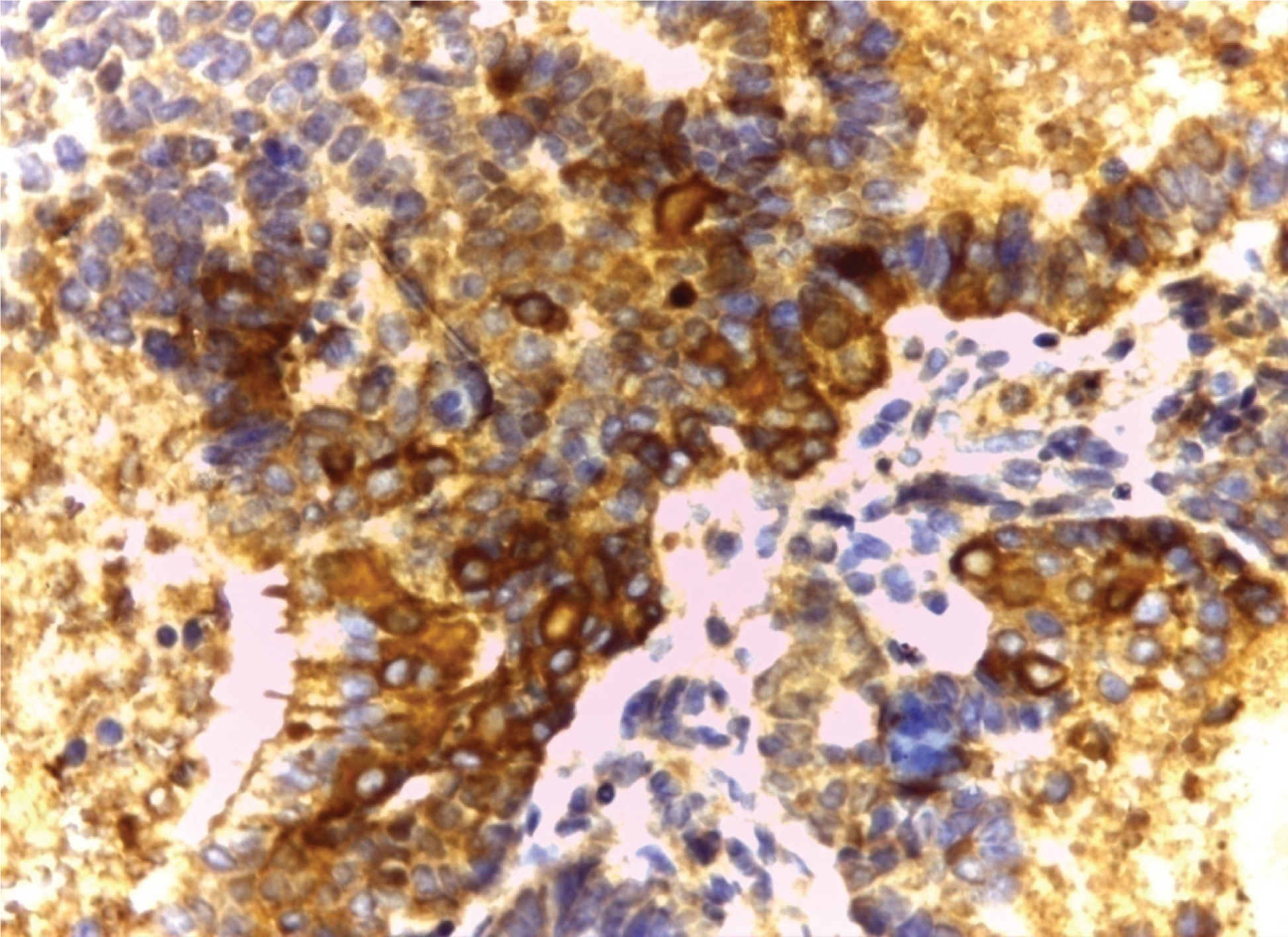
With histopathology, the differentials considered were Sinonasal Undifferentiated Carcinoma (SNUC), SNEC, melanoma and squamous cell carcinoma. Lymphoma was also considered as a differential and we proceeded with Immunohistochemistry (IHC). IHC was performed for LCA (Leukocyte Common Antigen), S-100, CK (Cytokeratin), NSE (Neuron Specific Enolase), p63 and chromogranin. Tumour showed strong positivity for chromogranin, NSE and cytokeratin [Table/Fig-4,5 and 6] and was negative for LCA, S-100, p63.
Immunohistochemistry for Cytokeratin (40X).
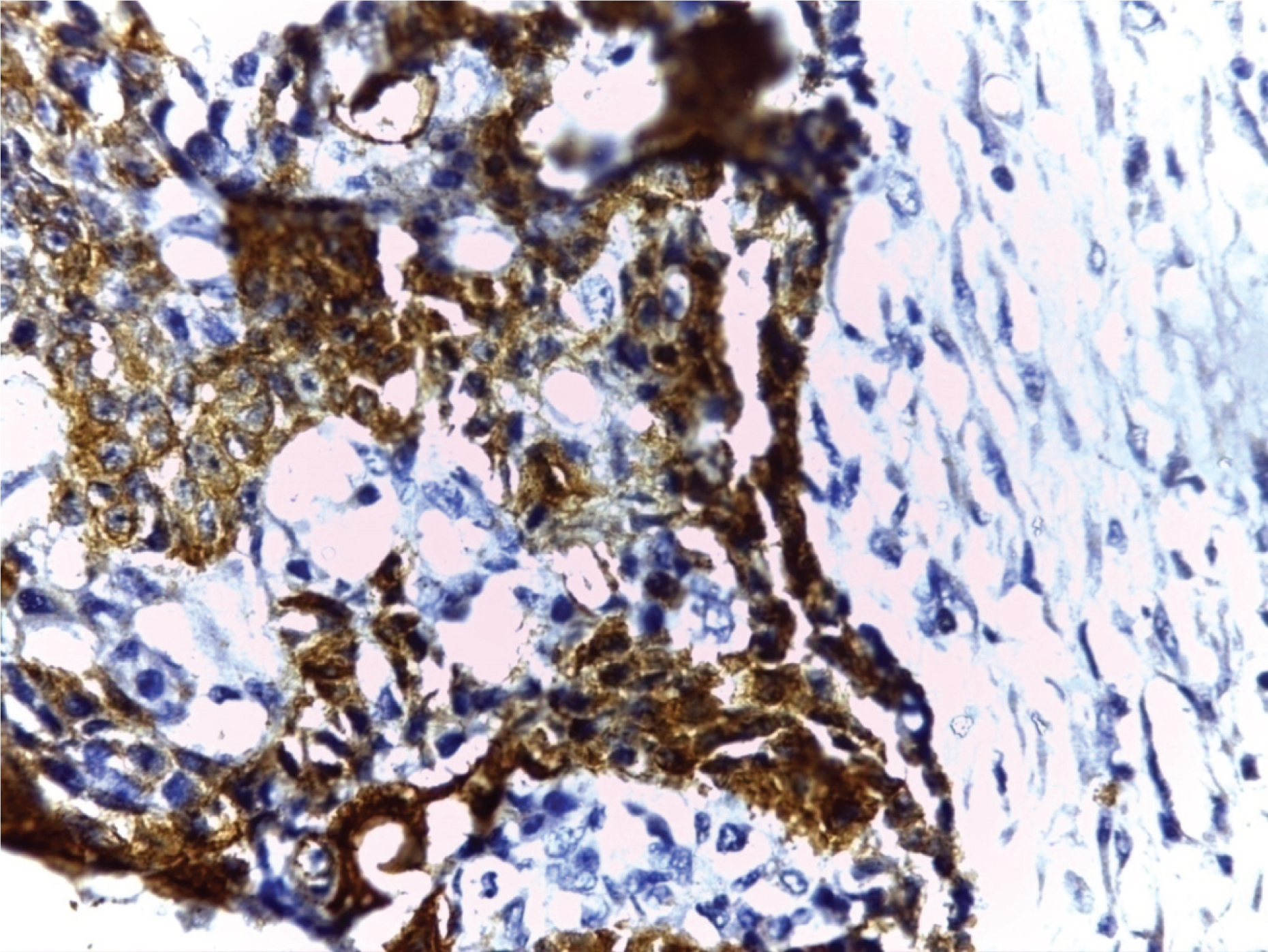
Immunohistochemistry for neuron specific enolase (40X).
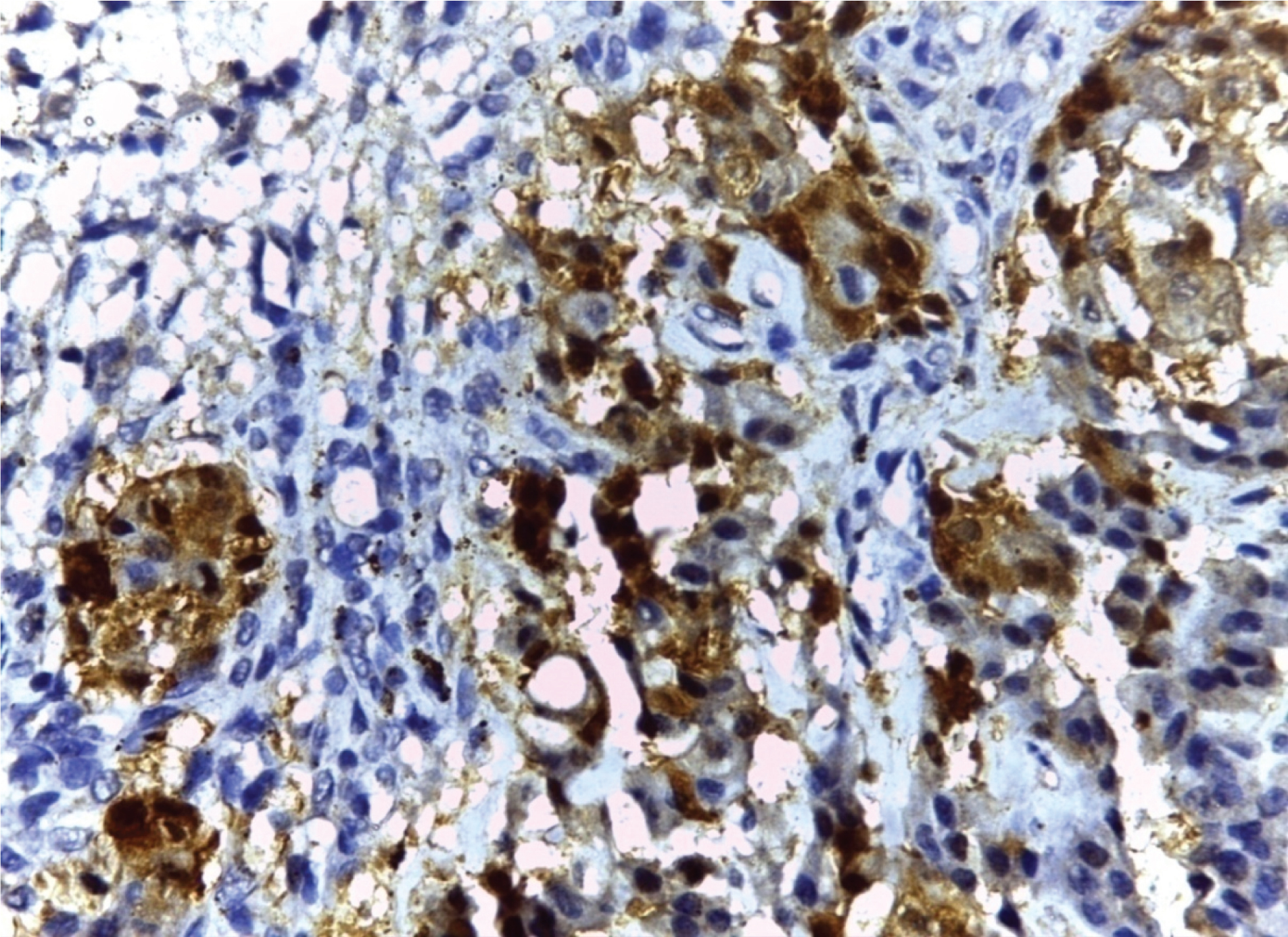
Immunohistochemistry for chromogranin (40X).
Correlating clinical features, cellular architecture and immunohis-tochemistry, the diagnosis of SNEC was favoured. The patient was referred to oncology department and she was treated with chemotherapy drugs Cisplatin and Etoposide. She attended oncology department for only two cycles of chemotherapy after which she was to lost to follow up.
Discussion
The sinonasal tract is highly exposed to carcinogenic substances and it is the location for a wide variety of both benign and malignant tumours. The more common tumour types are of epithelial origin. Carcinomas of the sinonasal tract account for approximately 3% of head and neck malignant neoplasms and less than 1% of all malignant neoplasms [1]. SNEC is a rare and very aggressive malignant tumour. It was first proposed as a distinct entity by Silva EG et al., in 1982 [2]. It appears usually in the sixth to seventh decades of life and shows male predominance. It is unusual under 40 years of age [3]. Neuroendocrine tumours are classified as typical carcinoid, atypical carcinoid and small cell neuroendocrine carcinoma. It is still not clear whether large cell neuroendocrine carcinoma that corresponds to the pulmonary counterpart occurs in these sites. There are few cases that do not fit these categories, and the diagnostic label “neuroendocrine carcinoma, not otherwise specified” may be used [3]. Till now no specific aetiologic factor has been identified [4].
The clinical features of SNEC are nonspecific and include nasal obstruction, epistaxis, facial mass, and/or facial pain. Majority of patients have advanced disease at presentation [5]. Tumours are very aggressive and may extensively involve the skull, orbit, and brain. They may also present with ophthalmic manifestations like exophthalmos, difficulty in visual acuity and restricted eye mobility. Local pain, anosmia and metastatic cervical nodes have also been described [5]. Lungs, liver, and bone are the common sites for distant metastases [2].
Conventional microscopy is generally insufficient for arriving at accurate diagnosis and immunohistochemistry studies are invariably needed to differentiate from other neoplasms involving nasal cavity and paranasal sinuses such as lymphoma, melanoma, olfactory neuroblastoma, SNUC. SNEC is a more cellular tumour and lacks neurofibrillary background of olfactory neuroblastoma. Gland formation can be seen, but true Homer-Wright rosettes with central fibrillary matrix are not seen. SNEC generally has a more compact architecture than olfactory neuroblastoma. The tumour can form either solid sheets or ribbons and trabeculae. Cytologically also the cells differ markedly from olfactory neuroblastoma in that they are larger, with more cytoplasm, coarser chromatin and larger nucleoli. Necrosis and increased mitotic figures may be seen [6,7].
SNEC is immunohistochemically distinct from SNUC. SNEC is frequently positive for chromogranin, synaptophysin and cytokeratin expression is strong. SNUC may express evidence of neuroendocrine differentiation based on NSE staining and sometimes, neurosecretory granules; but generally, synaptophysin and chromogranin staining is negative [8]. Sinonasal lymphoma does not exhibit trabecular, ribboning, or nesting patterns and expresses leukocyte common antigen [9]. Melanoma can mimic SNUC histologically and can be differentiated with the help of S100, since it is strongly expressed in melanoma and negative or only weakly positive in SNUC [9]. Another differential in this case was squamous cell carcinoma for which p63 was done and found negative.
Paranasal neuroendocrine tumours are recurrent and locally destructive. The treatment of SNECs is still a matter of debate. Due to complex anatomy of sinonasal tract and rarity of the sinonasal neuroendocrine tumours, patient often presents in advanced stage and thus requires more aggressive treatment by multimodality approach. As far as the management is concerned a definite protocol is yet to be developed by oncologists and some recommendations has been put forward based on retrospective data. In general, these patients usually present in advanced stages and hence surgery is extremely disfiguring without any cure. Treatment by chemotherapeutic drugs like Cisplatin and Etoposide followed by high dose proton – photon radiotherapy have proven beneficial [10,11].
Conclusion
SNEC presents as diagnostic challenge as it has overlapping histomorphological features with other tumours of the nasopharynx. Ancillary techniques like immunohistochemical studies are inevitable in the diagnosis. The tumour is aggressive and multimodality treatment approach is recommended. The case is being reported due to the extreme rarity of the neoplasm. Only around 80 cases have been reported in literature so far. Treatment approach is also a matter of controversy due to the lack of published literature.
[1]. Ferlito A, Rosai J, Terminology and classification of neuroendocrine neoplasms of the larynxORL 1991 53(4):185-87. [Google Scholar]
[2]. Silva EG, Butler JJ, MacKay B, Goepfert H, Neuroblastomas and neuroendocrine carcinomas of the nasal cavity. A proposed new classificationCancer 1982 50(11):2388-405. [Google Scholar]
[3]. Barnes L, Eveson JW, Reichart P, Sidransky D, World Health Organization classification of tumours: pathology and genetics of head and neck tumoursWord Health Organization Classification of Tumours: Pathology and genetics of head and neck tumours 2005 LyonIARC [Google Scholar]
[4]. Sirsath NT, Babu KG, Das U, Premlatha CS, Paranasal sinus neuroendocrine carcinoma: a case report and review of the literatureCase Reports in Oncological Medicine 2013 2013:728479 [Google Scholar]
[5]. Mitchell EH, Diaz A, Yilmaz T, Roberts D, Levine N, DeMonte F, Multimodality treatment for sinonasal neuroendocrine carcinomaHead & Neck 2012 34(10):1372-76. [Google Scholar]
[6]. Nagy AA, Trombitas V, Vlad D, Albu S, Sinonasal neuroendocrine carcinoma–a case reportRomanian Journal of Rhinology 2014 4(14):117-20. [Google Scholar]
[7]. Weinreb I, Perez-Ordoñez B, Non-small cell neuroendocrine carcinoma of the sinonasal tract and nasopharynx. Report of 2 cases and review of the literatureHead and Neck Pathology 2007 1(1):21-26. [Google Scholar]
[8]. Mills SE, Neuroectodermal neoplasms of the head and neck with emphasis on neuroendocrine carcinomasModern Pathology 2002 15(3):264-78. [Google Scholar]
[9]. Smith SR, Som P, Fahmy A, Lawson W, Sacks S, Brandwein M, A clinicopathological study of sinonasal neuroendocrine carcinoma and sinonasal undifferentiated carcinomaThe Laryngoscope 2000 110(10):1617-22. [Google Scholar]
[10]. Fitzek MM, Thornton AF, Varvares M, Ancukiewicz M, Mcintyre J, Adams J, Neuroendocrine tumours of the sinonasal tractCancer 2002 94(10):2623-34. [Google Scholar]
[11]. Krishnamurthy A, Ravi P, Vijayalakshmi R, Majhi U, Small cell neuroendocrine carcinoma of the paranasal sinusNatl J Maxillofac Surg 2013 4:111-13. [Google Scholar]