World Health Organization (WHO) defines Health needs as objectively determined deficiencies in health that require health care, from promotion to palliation [1]. Health Needs Assessment (HNA) is a systematic process for determining and addressing health-related needs or gaps between current and desired conditions [2]. HNA was used for the first time in the 19th century with an aim to identify and meet health needs in England. Despite the fundamental role of HNA in health policy, it has been paid less attention than outcome assessment; while it is vital for better health outcomes [3]. However, health policy makers constantly complain about the lack of access to some necessary evidence [4].
The evolution of health systems in most developing countries has been dominated by Western models. This process often neglects real health needs of local people and their healthcare seeking patterns including traditional medicine [5]. HNA as a popular tool for health policy makers is used to match health services with needs [6].
The same method cannot be used always for health needs assessment, as different subjects should be seen and investigated from different angles. In most cases, to collect needed data and information, a combination of qualitative and quantitative studies is used [5]. HNA should be performed in three steps: determination of the desired condition, assessment of the current condition, and identification of the gaps between desired condition and the current condition [6]. Identification of desired condition and priorities can occur through both using the community members opinions and experiences of experts who are aware of the needs [7].
A limited number of HNA studies are available in the literature. For example, a study was conducted in a rural community in North India by Mathias KR et al., [6]. Similarly, a few studies have been published on HNA of female adolescents; however, the available studies are mostly about their attitudes toward puberty [8]. As an example, a clinical trial has shown that teenage girls have flawed, wrong, and inadequate knowledge about puberty and health needs of the stage [9].
Health policy-makers and managers need accurate and timely information about changing health needs of the community and its subgroups including female adolescents [10]. WHO identifies adolescents from ages 10 to 19 [11]. Adolescence in girls is an important stage of fundamental changes that can positively or negatively affect their future lives, children, and families. The dual role of female adolescents on the health of communities and future generations has made one of the Millennium Development Goals (MDGs) be assigned to ensuring the health of this age-sex group [10]. United Nations Population Fund (UNFPA) urged all member countries to identify and meet the specific needs of female adolescents [12].
Female adolescents are about 7% of Iran’s population; 72% of them live in the cities and the rest live in the villages; 98% of them are literate; 11% of them are married, with 12.6% in cities and 9.3% in rural areas. Khorramabad as a metropolis is the center of Lorestan province in the southwest of Iran, which is one of the less developed provinces in Iran [13].
As we could not find any published comprehensive HNA study of female adolescents by its specific measuring tool published by Shahhosseini Z et al., we designed and conducted the current study on assessment of health needs among a sample of Iranian adolescent girls chosen from Khorramabad city in the year 2015 [14]. The study results can increase awareness of parents of their girls’ health needs. The findings can also help authorities plan and provide appropriate health services to girls in this age group.
Materials and Methods
The statistical population of the cross-sectional study was female adolescents studying in the first and second levels of high schools in Khorramabad city, in the year 2015. Using n= {(Z1-α/2×s)/d}2 formula and considering α=0.05, s= 0.55, and d=0.06 the minimum sample size was calculated as 320. Due to possible loss, 400 samples were collected.
The girls were selected through using the stratified and multistage cluster sampling. The first and second levels of high school were defined as stratums. Within these stratums different districts of the city were considered as clusters. After numbering the high schools, some of them were selected from the stratums and clusters randomly. Classrooms and students were selected using a systematic random sampling.
The inclusion criteria of the study were being within the ages of 12 and 18 and providing informed consent (from parents or themselves) to take part in the study. Before conducting the study, the required permits were received from officials at the city’s education office. Before collecting the required data and information, the study’s goals was explained to the students. Moreover, they were ensured that their information and comments would not be disclosed to anyone except for researchers and they will be used only for research purposes.
The tool used for data collection was Female Adolescents’ Health Needs questionnaire which had 63 questions in five categories including physical health, mental-emotional health, social health, spiritual health, and educational health. A five-point Likert scale was used to allow students to express how much they agree or disagree with the questions and statements. Validity and reliability of the questionnaire were approved by Shahhosseini Z et al., (CVI= 92%, IC=90%, and ICC= 98%) [14].
Statistical Analysis
The collected data were analysed using the SPSS (Statistical Package for Social Sciences) Version 20 software and its tools including correlation coefficient (for testing the correlation between different dimensions of health needs), t-test (for testing correlation between demographic variables except for the number of children and different dimensions of health needs), and ANOVA (for testing the correlation between number of children and different dimensions of health needs) and results were reported at a significance level of 0.05.
Results
The average age (years) of the participants was 14.61±1.64, with 63.25% of them studying in the first high school level and the rest in the second level. The mean and Standard Deviation (SD) of the participants’ Body Mass Index (BMI) was 20.86±8.25.
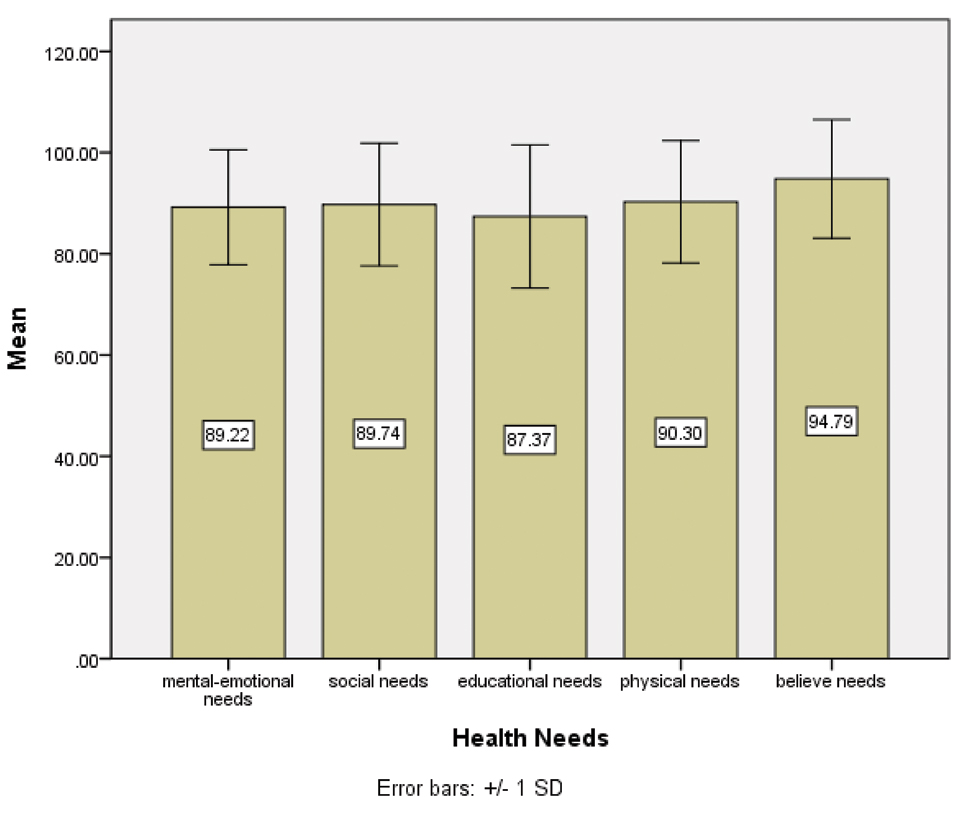
The study findings indicated that the mean and Standard Deviation (SD) of the girls’ health need scores is 89.79±11.47. The highest and lowest needs were spiritual and educational needs with the average scores of 94.79±11.70 and 87.37±14.13, respectively. The mean of other dimensions of the girls’ health needs is presented in [Table/Fig-1].
The mean score of different health needs among female adolescents.
Multivariable analysis (p-value<0.001) indicated that there is a significant difference between an average score of one of the health needs and educational level of female adolescents. Results also suggest that there is a significant difference between the average score of mental-emotional and social needs of the female adolescents and their educational level (p-value <0.05), where the average scores of female adolescents studying in the first level of high school were respectively 4.39 and 2.86 higher than the scores of the students studying in the second level of high school. No other significant differences were seen between educational level and other dimensions of health.
Also, the multivariable analysis indicated that there is no significant relationship between female adolescents’ easy access to the internet and their health needs (p=0.09). Correlation coefficients between age and mental-emotional needs and age and social needs were -0.17 and -0.11, respectively. The correlation coefficients are significant at 0.05 levels. The correlation coefficient (p<0.009) between weight and mental-emotional needs was -0.13. No significant linear relationship was seen between other dimensions. Also, there was no significant relationship between grade level of counselor, access to sports facilities, having a cellphone, and access to leisure-time facilities and different health needs of the female adolescents (p>0.05) [Table/Fig-2].
The Mean and Standard Deviation, and significance level of the relationships between health needs and demographic characteristics.
| Variable | Mental needs | Social needs | Educational needs | Physical needs | Spiritual needs |
|---|
| Level | FirstSecond | 90.83±8.3986.44±14.76 | 90.79±9.5187.93±15.55 | 87.62±12.5586.95±16.55 | 90.56±9.9089.84±15.10 | 95.35±9.5493.80±14.68 |
| p-value | 0.001 | 0.023 | 0.64 | 0.56 | 0.20 |
| Number of Child | 2 children-13- 4 childrenAbove 4 | 90.35±9.0290.00±12.9486.91±10.70 | 90.50±10.8289.81±13.0587.42±12.09 | 88.07±13.3487.21±15.2386.07±12.13 | 90.64±10.5389.95±13.4290.61±10.95 | 95.26±9.6594.56±13.4994.27±9.87 |
| p-value | 0.14 | 0.27 | 0.65 | 0.85 | 0.80 |
| Grade level of counsellor | Bachelor’s degreeMaster’s degree | 89.68±11.5786.87±10.57 | 89.94±12.9086.33±12.83 | 87.59±13.9683.18±17.23 | 90.28±12.1890.35±10.28 | 94.92±12.1892.50±9.66 |
| p-value | 0.34 | 0.19 | 0.17 | 0.97 | 0.36 |
| Internet access | havedoesn’t have | 89.68±9.8388.56±13.20 | 90.73±10.0388.32±14.55 | 87.49±12.8587.20±15.82 | 90.27±10.2790.33±14.26 | 95.04±9.9394.42±13.86 |
| p-value | 0.33 | 0.49 | 0.84 | 0.96 | 0.60 |
| Sport hall in the school | Havedoesn’t have | 89.82±8.7688.42±14.04 | 90.32±9.8388.97±14.66 | 87.17±12.5787.64±16.00 | 89.45±12.5791.41±13.82 | 94.49±10.5395.17±13.11 |
| p-value | 0.22 | 0.27 | 0.74 | 0.10 | 0.56 |
| Cellphone | Havedoesn’t have | 89.53±9.5488.98±12.54 | 90.30±10.3989.08±13.93 | 87.34±13.0387.41±15.38 | 90.35±10.1790.23±13.99 | 94.83±10.1294.72±13.35 |
| p-value | 0.54 | 0.31 | 0.96 | 0.92 | 0.92 |
| Leisure Program | Havedoesn’t have | 89.53±9.5688.98±12.54 | 89.75±11.0489.72±12.94 | 86.36±13.5988.13±14.51 | 90.23±10.6990.34±13.02 | 94.94±9.7994.67±12.98 |
| p-value | 0.63 | 0.98 | 0.21 | 0.93 | 0.81 |
The girls’ different health needs correlation coefficients are shown in [Table/Fig-3]. Correlation Coefficient test indicated that there are strong relationships between different needs of the girls. Social (75%) and spiritual (65%) dimensions had the highest and the lowest correlations with other dimensions, respectively. The highest and lowest correlation coefficients were between mental-emotional needs and social needs (0.77) and educational needs and spiritual needs (0.54), respectively. Spiritual needs had the highest correlation with mental-emotional needs. Physical needs had the highest correlation with social needs and educational needs had the highest correlation with social needs. Also, social needs had the highest correlation with mental-emotional needs.
Correlation coefficients between different dimensions of girls’ health needs.
| Dimensions of health needs | Mental-emotional | Social | Educational | Physical | Spiritual |
|---|
| Mental-emotional | 1 | 0.77* | 0.63* | 0.67* | 0.58* |
| Social | 0.77* | 1 | 0.68* | 0.73* | 0.57* |
| Educational | 0.63* | 0.68* | 1 | 0.67* | 0.54* |
| Physical | 0.67* | 0.73* | 0.67* | 1 | 0.57* |
| Spiritual | 0.58* | 0.57* | 0.54* | 0.57* | 1 |
| Mean | 0.73 | 0.75 | 0.70 | 0.73 | 0.65 |
* p-value <0.001
The highest and lowest average scores were given by the female adolescents to these two statements: “I want to be successful in life by having faith in God” (97.50%) and “I prefer group discussion as consulting programs” (62.60%), respectively. Noticeably, the highest and lowest health needs were seen in the mental-emotional dimension [Table/Fig-4].
The highest and lowest average scores on different health needs of female adolescents.
| Health needs | Statement with Highest Average Score | Percent | Statement with Lowest Average Score | Percent |
|---|
| Mental-emotional | I need peace of mind. | 97 | I prefer group discussion as consulting programs. | 62.60 |
| Social Health | There should be intimate behaviour between me and my family. | 96 | Experts should be invited to the schools to solve students’ problems. | 85.30 |
| Educational Health | I should receive training about essential life skills. | 90.80 | I need to use social media (internet, mobile phone) for educational purposes. | 80 |
| Physical Health | I want to have easy access to safe uncontaminated water. | 97 | Free food should be provided to students by schools. | 78.50 |
| Spiritual Health | I want to be successful in life by having faith in God. | 97.50 | Interesting knowledge about religion should be offered to students. | 93.80 |
Discussion
The aim of the present study was to identify health needs of female adolescents in Khorramabad as a sample group, representing teenage girls living in Iran in 2015. The range of scores obtained for the female adolescents’ health needs was 87.37-94.79, showing that the research subjects greatly needed various kinds of health needs. The priority order of health needs for female adolescents was spiritual health, physical health, social health, mental-emotional health, and educational health, in the order of their appearance.
The average score of spiritual health needs among the subjects was 94.79. According to the religious background in the society and the possibility of easy fulfillment of the above-mentioned need in Iran, it was presumed that the spiritual needs of female adolescents are acceptably fulfilled; this result is in disagreement with the results of the present study. The most frequent spiritual need among the subjects was “achieving success by having faith in God” and the least frequent was “being offered interesting knowledge about religion”. In a qualitative study investigating female adolescents’ spiritual needs in Sari city (Iran) in 2009, “having faith in God” and “avoiding from picturing a violent image from religion” were among the highlighted items [15].
The average scores of physical health needs, as the second presented need was 90.30. The most frequent physical needs mentioned by the subjects included easy access to dairy products, fruits and vegetables, breakfast and free meals in school. Given the rather acceptable availability of different products and health facilities for female adolescents living in big cities, physical health needs were expected to have a lower priority for the subjects, however, the findings showed opposite results.
The average score of social health needs, as the third need, was 89.74. The most frequent needs mentioned by the participants were “having friendly relations in family”, “no prejudice among children”, and “popularity and acceptability among peers”. In a qualitative research on female adolescents’ health needs focused on the role and importance of family in Mazandaran province (Iran), “the need for a friendly relation in the family” was identified as a crucial need of the subjects [16]. Some researchers have shown a negative relation between friendly family relations and dangerous behaviours, such as smoking among teenagers [17,18]. In addition, in some other studies, the relationship between family support and an increase in self-confidence, life satisfaction, the ability to deal with stressful conditions, and a decrease in depression have been reported [19,20]. In this regard, Hamidi pointed out that having friendly family relations are one of the teenagers’ mental-emotional needs [21]. It is worth mentioning that in the instruments used in the current research, the friendly family relations is a subdivision of social health needs, while in the study by Hamidi the variable was categorized as a subdivision of mental-emotional needs.
The average score of mental-emotional needs for the female adolescents was 89.22. According to the special atmosphere of teenage years, mental-emotional needs were expected to gain a higher priority. In a research by Shah Hosseini and colleagues, the average score of mental-emotional health needs of female adolescents in Mazandaran province (Iran) was 35.83. The disparity between the results of the present study and that by Shahhosseini Z et al., is due to the difference in the average score calculation methods used. In this study, the average of Likert scale percentage was calculated instead of the actual score of each variable [22]. In another research, on 502 female high school students in the city of Isfahan (Iran), mental-emotional health needs were ranked in the first priority among all 57 needs of teenagers. The study showed that teenagers’ needs are more spiritual and the emotional dimensions of their needs are stronger from other dimensions [23]. Yet, the results obtained from the current research showed that family and society could be able to partially fulfill mental-emotional needs of the subjects. The most frequent mental-emotional health needs mentioned by the subjects was “having mental peace” and the least mentioned was “holding consolation programs as group discussions”. In comparison, in the study by Shahhosseini Z et al., the most and the least mentioned needs were “stressful school tests” and “having a same-sex counselor”, respectively [22]. As mentioned earlier, the difference might be due to the various methods used in the calculation of average scores.
The average score of educational health need was 87.37. It is seen that that educational health needs have been estimated much higher than other health needs. In this regard, 4 out of all mentioned needs were the most important; i.e., life skills, appropriate diet, common diseases, and sexual hygiene. In the qualitative research by Shahhosseini Z et al., the need for life skills was among the items highlighted [24]. In another study the average score of educational needs of female teenagers in Sari city (Iran) was 77.2 that are 15% lower than the number obtained in the present research. The four most frequently mentioned educational needs in Shah Hosseini’s study were appropriate behaviour with a future spouse, preventing from dangerous sexual affairs, life skills, and maturity hygiene, in the order of their appearance [25].
The results of the current research showed that there is a direct relationship between all dimensions of female adolescents’ health needs with other variables. Social and spiritual needs were respectively the most and the least correlated variables. These findings, however, are inconsistent with the results of other studies. The researchers expected the mental-emotional needs to have the strongest and educational needs to have the weakest correlation with other health needs. The specific age-sex related features might have affected the correlation between the variables.
An explanation for this observation is that teenagers’ full-time access to the internet and social networks affect different dimensions of their physical, social, mental-emotional, spiritual, and educational health needs. However, no significant relationship was found between the above-mentioned variables in the present study. The direct relation between internet addiction and social solitude or depression, and also its negative relation with educational output, family relations, and general health have been reported in other studies [26,27]. However, Tamannayaifar M and Mohseni Tabrizi A HH et al., showed there was no relationship between full-time internet access and religious beliefs, poor educational outputs, and family relations. They also reported educational use of the internet by the teenagers [28,29]. According to the paradoxes detected in the findings, it is recommended conducting more research to more accurately investigate the relation between the aforementioned variables.
A poor negative significant correlation between age and mental-emotional and social health needs could be largely attributed to the large size of the sample group; because, in that case, the calculated correlation coefficient in various educational level would reduce significantly, showing no meaningful relationship. Therefore, it can be concluded that the significant difference between average scores of mental-emotional and social needs in the first and second levels of school is not affected by the age. This outcome can be attributed to the beginning of sexual and emotional maturity period coincident with teenage. Based on the presumptions of the researchers, in maturity period, mental-emotional, social and spiritual needs undergo drastic changes. However, in the present research, there was no significant change in the variables detected. No relation between physical and educational needs and age was consistent with the presumptions of the researchers. Given the poor relation between mental-emotional and social needs with age, and also no relationship between spiritual needs and the mentioned variable, it is highly recommended that the relations be examined in further researches.
Conclusion
Considering the poor negative relation between mental-emotional needs and body weight, it is concluded that character type of the subjects might be in relation to their phenotype. Thus, people with higher weights are more sociable and have less mental-emotional needs. A relation between the availability of recreation facilities and mental-emotional needs among the subjects was expected. However, the results showed no relation among the variables.
To the best of our knowledge, the present study is the first comprehensive research on female adolescents’ health needs assessment using a special instrument, published in the world. Serious health needs of female adolescents in Iran calls for the relevant authorities, such as policy makers and health service providers, school managers, Ministry of Youth Affairs and Sports, and parents to design appropriate interpretive programs to fulfill different health needs of the teenagers. The researchers recommended conducting a similar study in the other countries of Eastern Meditation Region.
* p-value <0.001