EARR is defined as a definite and permanent shortening of root apex that is typically documented using radiograph [1]. EARR is characterized by loss of the superficial layer of cells that protect the tooth root.
EARR occurs during orthodontic treatment when forces at the root apex exceed the resistance and reparative ability of the periapical tissues [2]. Increased root resorption has been observed during orthodontic tooth movement, when compared with physiologic root resorption in humans [3]. The incidence of apical root resorption during orthodontic treatment can range from 5% to 18%. About 5% of adults and 2% of adolescents are likely to have at least one tooth that resorbs more than 5 mm during treatment [4].
The recent development of three dimensional imaging and analysis provide accurate measurement without superimposition. Dentascan is a CT software program that allows the maxilla and mandible to be imaged in different planes. It combines the details of CT imaging with the convenience of interacting with the images on a computer [9].
Although, many studies have been done on EARR, very few studies have examined root resorption of permanent teeth with adequate radiographic technique during retraction of anterior teeth. Therefore, the aim of the study was to investigate the prevalence and degree of orthodontically induced EARR with fixed appliances in permanent teeth, from central incisor to first molar after en-masse retraction of anterior teeth using Dentascan.
Materials and Methods
This was a prospective study. It was approved by Ethical Committee of Institute of Dental Sciences, Bareilly, Uttar Pradesh, India. Subjects reporting to the Department of Orthodontics and Dentofacial Orthopaedics at Institute of Dental Sciences, Bareilly requiring orthodontic treatment were included in the study. Treatment plan was presented to the patients and consent forms were signed.
Total 20 arches of patient between 15 to 24 years with (mean±SD) 18.4±3.13 years were taken for this clinical study. Purposive sampling was used to determine the sample size. Inclusion criteria were patients having anterior dentoalveolar protrusion with minimal crowding (≤3 mm) with no use of anti-inflammatory drugs for at least six months before or during the study, no significant medical history and patients with good periodontal health were taken for the study. Exclusion criteria were patients showing any signs of active periodontal disease, previous traumatic dental history, or orthodontic treatment, individuals with inadequately treated endodontic problems and bruxism, any signs of EARR observed at the first examination using orthopantomogram. Duration of en-masse retraction was nearly six months.
Indicated first premolars were extracted and patients were bonded with MBT brackets 0.022 slot (UnitekTMGemini MBTTM Metal Brackets), initial alignment and levelling was done by using 0.016” NiTi arch wire and till a 0.017 x 0.025” stainless steel wire fits passively in the bracket slots. To reinforce the anchorage, Trans Palatal Arch (TPA) was used in all the patients. In patients with vertical growth pattern (Frankfort mandibular plane angle (FMPA) >30°) along with TPA, second molars were included in the anchorage unit by placing a bonded attachment and ligating first and second molars.
After the alignment and levelling was completed, en-masse retraction was performed in lower arch (working wire 0.017 x 0.025” stainless steel) using sliding mechanics. Retraction was carried out using NiTi closed coil spring (GAC Sentalloy, extra heavy), exerting a force of 250 g on each side. The coil spring was extended from canine to the first molar. The six anterior teeth were tied in a figure of 8 segment.
En-masse retraction in the upper arch was done using loop mechanics [Table/Fig-1]. Figure of 8 was done in the anterior segment from canine of one side to canine of another side. Segmental mechanics with T-loop, fabricated using 0.017”×0.025” TMA wire were used for the en masse retraction in the upper arch. Six preactivation bends were given in the T-loop [Table/Fig-2]. A sum total of 180°bend was incorporated, comprising of four bends of 25°each in the horizontal arm of the T-Loop and two bends of 40° each were given in the loop. Trial activation was done to relieve the stress and after initial activation of 5 mm was done. The loops were activated at an interval of six to eight weeks.
Photograph showing en-masse retraction with T-loop in maxillary arch and closed coil spring in mandibular arch.

Line diagram showing bends in preactivated T-Loop.
Computed Tomography was used for evaluating the changes in the root resorption before and after the retraction of anterior teeth. All the CT scans were carried out by a single experienced radiologist using the same tomographer.
The CT scans (GE Bright Speed 16 Slice China) were obtained for both maxillary and mandibular arches with contiguous 0.625 mm slice thickness at 120 kV, 175 mA, with the window width set at 1500 HU and 3600 rotations. The resultant images were then reconstructed, using Dentascan software (GE,USA). The same measurements were repeated after the completion of retraction.
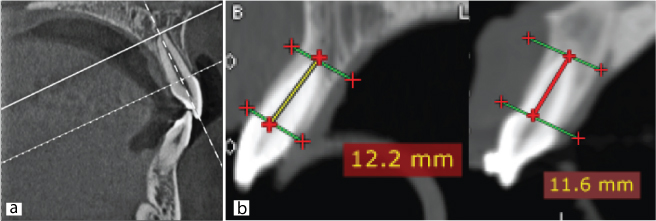
To evaluate changes in root resorption, CT images were taken pre-retraction (T0) and post-retraction (T1). Reconstructions were made so that the axial slices became perpendicular to the long axis of the tooth/root. This provided optimal visualization of the tooth/ root in axial, coronal, and sagittal planes. A reference line was placed connecting the buccal and palatal/ lingual cementoenamel junctions [Table/Fig-3a]. Parallel to this, a second reference line was placed at the root apex. Without access to previous radiographs or protocols, the perpendicular distance between these reference lines was measured for incisors to first molars by one of the authors. It was measured to be around 0.01 mm approximately in fully erupted teeth in which the cementoenamel junction (CEJ) and the apex could be clearly identified [Table/Fig-3a]. For teeth with multiple roots, each root was separately assessed. The same measurements were repeated after completion of retraction. Post-retraction (T1) measurements were taken at the same slice levels as the pre-retraction (T0) measurements [Table/Fig-3b]. All measurements were determined by a single investigator.
Measurement of root resorption.
The changes in the root length of maxillary teeth (central incisor, lateral incisor, canine, second premolar, first molar- mesiobuccal root (mbr), first molar- distobuccal root (dbr) and first molar-palatal root (pr) and mandibular teeth (central incisor, lateral incisor, canine, second premolar, first molar- mesial root (mr) and first molar-distal root (dr) were assessed at pre-retraction and post-retraction using CT scan.
Statistical Analysis
Difference in root resorption (pre and post) was compared by paired t-test. Comparisons of root resorption between maxillary and mandibular arches were estimated by Student’s t-test. A two-tailed p<0.005 was considered statistically significant. Analyses were performed on SPSS software (Windows version 17.0).
Results
The present CT study assesses degree of root resorption and comparison for both the arches was done.
Root Resorption in Maxillary Arch
The pre-retraction (T0) and post-retraction (T1) root length of maxillary arch is summarised in [Table/Fig-4]. Comparing the mean root length, paired t-test showed significant (p<0.001) reduction in length of roots after retraction.
Comparison of mean root length (mm) of various teeth in maxillary arch at pre-reatraction (T0) and post-retraction (T1) (mean±SD).
| Linear measurements (mm) | Pre(T0)(n=20) | Post(T1)(n=20) | Change(Pre-Post) | t-Value | p-value |
|---|
| Central incisor | 10.70±0.53 | 9.12±0.83 | 1.57±0.88 | 7.98 | <0.001 |
| Lateral incisor | 10.31±0.73 | 8.52±0.52 | 1.79±0.71 | 11.22 | <0.001 |
| Canine | 13.12±0.56 | 12.52±0.28 | 0.60±0.55 | 4.86 | <0.001 |
| Second premolar | 11.99±0.39 | 11.50±0.31 | 0.49±0.32 | 6.90 | <0.001 |
| First molar-mbr | 10.88±0.95 | 10.39±0.88 | 0.49±0.49 | 4.50 | <0.001 |
| First molar-dbr | 10.88±0.82 | 10.07±0.61 | 0.81±0.53 | 6.83 | <0.001 |
| First molar-pr | 12.25±0.74 | 11.00±0.70 | 1.25±0.96 | 5.86 | <0.001 |
The mean root resorption (i.e. mean change in root length from pre to post) was found highest in lateral incisor 1.79 mm (17.3%) followed by central incisor 1.57 mm (14.7%), first molar-pr 1.25 mm (10.2%), first molar-dbr 0.81 mm (7.4%), canine 0.60 mm (4.6%), first molar-mbr 0.49 mm (4.5%), and second premolar 0.49 mm (4.1%) i.e. (second premolar = first molar-mbr< canine < first molar-dbr< first molar-pr < central incisor < lateral incisor) [Table/Fig-4].
Root Resorption in Mandibular Arch
The mean root resorption (i.e. mean change in root length from pre to post) was found highest in lateral incisor 1.51 mm (16.3%) followed by central incisor 1.49 mm (16.0%), canine 0.53 mm (4.5%), first molar-mr 0.42 mm (4.0%), first molar-dr 0.42 mm (4.0%), and second premolar 0.38 mm (3.5%) i.e. second premolar < first molar-mr = first molar-dr< canine < central incisor < lateral incisor [Table/Fig-5].
Comparison of mean root length (mm) of various teeth in mandibular arch at Pre-retraction (T0) and post-retraction (T1) (Mean±SD).
| Linear measurements (mm) | Pre (T0)(n=20) | Post (T1)(n=20) | Change(Pre-Post) | t-value | p-value |
|---|
| Central incisor | 9.31±0.71 | 7.83±1.03 | 1.49±0.85 | 7.82 | <0.001 |
| Lateral incisor | 9.29±0.65 | 7.78±0.97 | 1.51±0.85 | 7.92 | <0.001 |
| Canine | 11.73±0.91 | 11.20±0.80 | 0.53±0.27 | 8.85 | <0.001 |
| Second premolar | 10.87±0.44 | 10.49±0.48 | 0.38±0.20 | 8.66 | <0.001 |
| First molar-mr | 10.44±0.97 | 10.02±1.14 | 0.42±0.25 | 7.50 | <0.001 |
| First molar-dr | 10.37±1.01 | 9.95±0.91 | 0.42±0.20 | 9.13 | <0.001 |
Comparison of Root Resorption between Maxillary and Mandibular Arches
The comparison of root resorption between maxillary and mandibular teeth was also done and summarised in [Table/fig-6]. Student’s t-test showed significantly (p<0.001) more reduction (50.9%) of mean root resorption of maxillary first molar as compared to mandibular first molar. However, on comparing other maxillary teeth, to mandibular teeth no significant differences were found [Table/Fig-6].
Comparison of extent of root resorption of respective teeth between maxillary and mandibular arches.
| Linear measurements (mm) | Maxilla(n=20) | Mandible(n=20) | %change | t-value | P-value |
|---|
| Central incisor | 1.57±0.88 | 1.49±0.85 | 5.5 | 0.32 | 0.754 |
| Lateral incisor | 1.79±0.71 | 1.51±0.85 | 15.4 | 1.11 | 0.275 |
| Canine | 0.60±0.55 | 0.53±0.27 | 11.6 | 0.51 | 0.614 |
| Second premolar | 0.49±0.32 | 0.38±0.20 | 22.4 | 1.32 | 0.196 |
| First molar | 0.85±0.61 | 0.42±0.15 | 50.9 | 3.10 | 0.004 |
| Total | 1.06±0.56 | 0.86±0.37 | 18.4 | 1.30 | 0.203 |
Discussion
External apical root resorption (EARR) is a side effect related to the biological tissue response during movement of teeth [10]. The frequency of root resorption examined by histological procedure is found to be 100% among orthodontically treated teeth but it is not so frequently observed with conventional radiographic technique [11]. These radiographic techniques may either underestimate or overestimate the amount of root structure loss [12].
Conventional radiographic methods for assessing root length cannot reliably compensate for inherent radiographic distortion. According to several studies, conventional intraoral radiography is not a reliable technique for the diagnosis of external root resorption in its early stages. So this study design, included the use of CT to minimize the errors in radiographic evaluation.
During orthodontic treatment with fixed appliances, the objective is to produce tooth movement as much as possible by frontal resorption. Lighter forces are compatible with survival of the cells within the PDL and a remodelling of the tooth socket by a relatively painless “frontal resorption” of the tooth socket. Keeping this in mind, the force of retraction was kept within the advised limit in the present study [13].
En-masse retraction was done following premolar extraction in both the arches. En-masse retraction is an effective procedure in controlling loss of anchorage as compared to two-step retraction technique. Two-step retraction technique results in formation of unaesthetic spaces distal to the lateral incisor teeth and is more time consuming [14]. The fixed appliances treatment duration was found to contribute significantly to apical root resorption [15].
During en-masse retraction in maxillary arch, lateral incisors showed highest root resorption (1.79±0.71 mm) followed by central incisors (1.57±0.88 mm) as compared to any other teeth. These findings were in agreement to the study done by Artun J et al [16] who have reported a root shortening of 1.17±1.15 mm in lateral incisor and 1.01±1.05 mm in central incisor. Smale I et al., [17] also reported greater root resorption in maxillary lateral incisors (0.59±0.68 mm) than in maxillary central incisors (0.48±0.53 mm). Lateral incisor root is smaller and more conical in shape, so it experiences heavier forces as compared to other teeth [18,19]. These studies were in contrast to findings of Jung YH and Cho BH. [20] where maxillary central incisors showed highest root resorption followed by maxillary lateral incisors.
In general, the most frequent and severe EARR is seen in the type of tooth which moved the farthest. During the treatment, the maxillary incisors comparatively moved a greater distance than any other tooth. Hence, in these teeth this can be a major factor for greater extent of root resorption.
Extraction cases shows higher incidence of root resorption as compared to non-extraction cases as incisors have to move a greater distance than in nonextraction cases as suggested by Sharpe W et al., [21].
After incisors, molar teeth showed highest resorption among all teeth. Palatal roots showed a shortening of 1.25±0.96 mm and distobuccal root resorption of 0.81±0.53 mm. Similar results were reported by Sharpe W et al., [21]. They observed that molars had the second highest incidence of EARR after maxillary central incisors. The high incidence of post-treatment EARR of molar teeth may reflect the increased mechanical stresses placed over molar teeth for longer period compared to premolar teeth [22].
Root resorption in canine was 0.60±0.55 mm in our study. Least root resorption was seen in second premolar (0.49±0.32 mm) as well as mesiobuccal root of first molars. Agarwal SS et al., [22] in their study reported minimum root resorption in premolar roots in extraction cases. However, in a study conducted by Ajmera S et al., [23], canine roots showed least root resorption following en-masse retraction.
Similarly, in the mandibular arch, amount of root resorption was found to be highest in lateral incisors (1.51±0.85 mm) followed by central incisors (1.49±0.85 mm). Jung YH and Cho BH et al [20] in their study reported a root resorption of 0.63±0.52 mm in mandibular lateral incisors and EARR of 0.62±0.67 mm in mandibular central incisors in extraction cases. In present study, root resorption in canine was found to be 0.53±0.27 mm and minimum root resorption was seen in the premolar (0.38±0.20 mm). Other authors have also reported minimum root resorption in premolars of mandibular arches [22].
When comparing maxillary and mandibular arch, it was observed that maxillary teeth showed greater root resorption than mandibular teeth. More root resorption was seen in maxillary incisors than mandibular incisors, though the difference was not significant. Similarly Huang Y et al., [24] demonstrated more root resorption in upper incisors as compared to lower incisors. Apajalahti S and Peltola JS [15]. also observed maxillary incisors to be more resorbed than mandibular incisors. No significant difference was seen while comparing upper and lower canines and premolars. However, when molars were compared for root resorption in both the arches, significant difference was found between the two arches.
Proximity between the roots of maxillary central incisors and the cortical bone of the socket, the incisive canal and the alveolar bone on the buccal surface, combined with the increased torque of maxillary incisor roots against the palatal cortical plate may explain the higher incidence of severe EARR in maxillary teeth.
When comparing frequency of root resorption, all teeth showed some extent of root shortening. Similar findings were reported in studies by Levander E and Malmgren O [25]. and Smale I et al., [17] wherein root resorption to some extent was observed in all the teeth. A great variation in prevalence of root resorption is reported due to variation in examination method, definition of root resorption and type of appliances used. According to Lund H et al., [10] almost all patients showed some degree of root resorption during orthodontic treatment.
EARR is an unavoidable iatrogenic consequence of orthodontic treatment. The severity of root resorption increases when maxillary and mandibular anteriors are retracted in premolar extraction cases. In the present study, root resorption was observed in almost all the teeth to some extent. The highest chances of root resorption were observed in the lateral incisors and minimum resorption was seen in the roots of premolars.
The significant finding indicates that root resorption is more common in incisors. This may lead to unfavourable crown-root ratio of these teeth. So, periodic monitoring may limit these common iatrogenic sequelae of orthodontic treatment.
Limitation
The extent of root resorption was observed at one point of time, thus the observation of complete process of root resorption and repair was beyond the scope of this study design. So, a further longitudinal study following up the patients is advised in order to understand the process of root resorption and repair of root resorption. Also, comparison between two-step retraction and en-masse retraction was not made in the present study. Purposive sampling was used in the study and the sample size was less due excessive radiation exposure during dentascan of the patient. This may be considered as the limitation of the study.
Conclusion
EARR occurred in almost all the teeth from incisors to first molar during en-masse retraction of anterior teeth. Maxillary teeth are more prone to external apical root resorption than mandibular teeth. Lateral incisors showed more root resorption followed by central incisors and molars, whereas minimum root resorption was seen in premolars in both the arches.