Clinical Significance of Presence of Extensor Indicis Brevis Manus – A Case Report
N Esakkiammal1, Renu Chauhan2, Rakhee Sharma3
1 Senior Demonstrator, Department of Anatomy, University College of Medical Sciences, Delhi, India.
2 Professer and Head, Department of Anatomy, University College of Medical Sciences, Delhi, India.
3 Senior Demonstrator, Department of Anatomy, University College of Medical Sciences, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. N Esakkiammal, Senior Demonstrator, Department of Anatomy, UCMS and GTB Hospital, Dilshad Garden-110095, Delhi, India.
E-mail: esakki510@gmail.com
Anatomical variations of additional muscles and tendons are commonly encountered in extensor aspect of the forearm and hand during surgeries and dissections. There are reports on different kinds of variations like, extra tendons, additional bellies, and abnormal attachments of the muscle. Surgeons should have the knowledge about these variations for muscle or tendon grafting and also to plan surgeries. While dissecting the extensor compartment of the forearm and dorsum of hand of an elderly female cadaver, an anomalous muscle belly was noticed on dorsum of hand bilaterally alongwith the main tendon of extensor indicis muscle. This additional belly of extensor indicis muscle was called Extensor Indicis Brevis Manus (EIBM). This muscle originated from the dorsal carpal ligament and joins the main tendon of extensor indicis muscle in both the hands. Awareness of existence of this kind of variation is important for clinicians and surgeons for a correct diagnosis and eventual surgery in patients presenting with a cyst on the dorsum of hand, to avoid accidental mishaps.
Additional belly of extensor indicis, Extensor muscles, Hand surgeries
Case Report
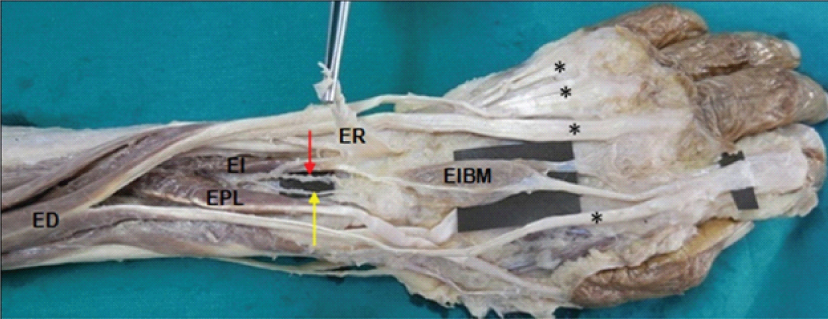
During a routine dissection of the back of a forearm and dorsum of the hand of a 62-year-old formalin fixed female cadaver at University College Of Medical Sciences (UCMS), Delhi, an atypical presentation of extensor indicis was observed in both the hands. In the left hand [Table/Fig-1], an additional fusiform shaped muscle belly of extensor indicis was observed arising from dorsal carpal ligament. This belly was larger in size in comparison to the belly size of normal extensor indicis. The muscle fibers of this additional belly joined the main tendon of extensor indicis distally. It also gave a small slip of muscle fiber on the medial side of main tendon of extensor indicis. This slip of muscle fiber merged with the fascia covering dorsum of hand at the level of head of the third metacarpal.
Showing fusiform shaped EIBM in the dorsum of left hand arising from dorsal carpal ligament. Distally, it joins the main tendon of extensor indicis and small slip fiber merging with the fascia of the dorsum of hand at the level of head of the third metacarpal.
*ED-extensor digitorum, EI-extensor indicis, EPL-extensor pollicis longus, ER-extensor retinaculum everted, EIBM-extensor indicis brevis manus. Asteric marked tendinous slips of extensor digitorum, Red arrow pointing at anterior interosseous artery, Yellow arrow pointing at posterior interosseous nerve.
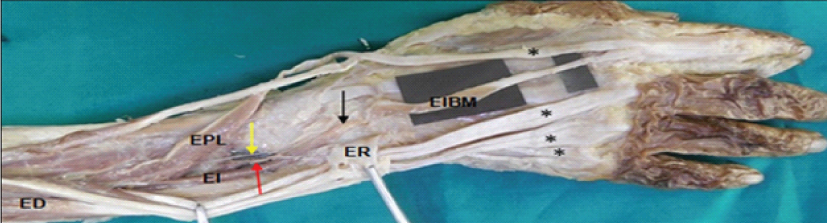
In the right hand [Table/Fig-2], extensor indicis muscle extended till the dorsal carpal ligament present in the fourth compartment of the extensor retinaculum. Additional slender muscle belly arose from dorsal carpal ligament and joined main tendon of extensor indicis. These anomalous bellies were called as EIBM. Posterior interosseous nerve supplied EIBM on both the sides.
Showing slender slip of EIBM in the dorsum of right hand originating from dorsal carpal ligament. Distally, it joins with the main tendon of extensor indicis.
*ED-extensor digitorum, EI-extensor indicis, EPL-extensor pollicis longus, ER-extensor retinaculum everted, EIBM-extensor indicis brevis manus, Asteric marked tendinous slip of extensor digitorum, Red arrow pointing at anterior interosseous artery, Yellow arrow pointing at posterior interosseous nerve, Black arrow pointing at muscular fibers of EI extending till the fourth compartment of extensor retinaculum.
Discussion
Accessory muscles are anatomical variants representing additional muscles that are present along with normal muscles. Extensive variations exist in the form, size and the pattern of insertion of the muscles. Many accessory muscles especially in the musculature of the hand have been described by Natsis K et al., 2007 [1]. Earlier studies have reported anomalous extensor muscles of dorsum of the hand for example anomalous Extensor Indicis Propius (EIP), Extensor Digitorum Brevis Manus (EDBM), Extensor Mediiproprius (EMP), Extensor Indicis etmediicommunis (EIMC), and an accessory belly of the dorsal interosseousmuscle [2,3].
Variation of the extensor indicis muscle is quite common. Accessory slips, accessory tendons and various other anomalies have been reported by Yoshida Y in 1990 [4]. In the present case, while dissecting the upper limbs of an elderly female, apart from the presence of normal belly of extensor indicis, an additional belly of extensor indicis muscle was also noticed on dorsum of the hand bilaterally. This belly was called EIBM. According to Standring Susan, additional muscle belly of extensor indicis muscle can be rarely found [5]. Arathala R et al., reported a rare variation of the extensor indicis muscle that arose from the lunate bone and dorsal radiocarpal ligament and inserted into the distal phalanx of the index finger on ulnar side of the extensor expansion [6].
Variations in origin of extensor indicis muscle were found in three cases out of 263 cases of back of the forearm and dorsum of hand dissected by Cauldwell EW et al., in 1943. Additional belly of extensor indicis muscle either arose from the dorsal carpal ligament or arose as two heads from dorsal aspect of the carpal bones or from the distal end of the radius or from both dorsal carpal ligaments and carpal bones [7]. Variation observed in the present case was similar to the first type as reported by Cauldwell EW et al., i.e., additional belly arose from the dorsal carpal ligament.
Yoshida Y dissected 22 upper limbs out of which he observed absence of extensor indicis muscle in 11 upper limbs but at the same time he observed the presence of EDBM in these limbs. EDBM had a short belly on the proximal part of the dorsal surface of hand. They noticed origin of this muscle belly from dorsal carpal ligament. However, absence of extensor indicis was reported by them whenever this additional belly (EDBM) was present [4]. Whereas, in the present case extensor indicis was also present along with this additional belly (EIBM). In the present case an additional muscle belly arose from the dorsal carpal ligament similar to the observation by Yoshida Y. Presence of this kind of muscle variations can be associated with pain and swelling at the back of the hand and it may be confused with the presence of a dorsal synovial cyst [8].
Extensor indicis muscle, in the present case extended into the fourth dorsal compartment of the extensor retinaculum. The presence of additional muscle in the fourth compartment of the extensor retinaculum may lead to a condition called fourth-compartment syndrome, which is manifested by chronic dorsal wrist pain of the fourth compartment. The signs and symptoms produced by increased pressure within this compartment may compress the posterior interosseous nerve directly or indirectly [9].
In the present case, EIBM and extensor indicis muscle were also being commonly supplied by posterior interosseous nerve. Accordingly, EIBM could be a variant of extensor indicis muscle. In chronic disability produced as a result of malfunctioning of the tendons of abductor pollicis brevis and opponens pollicis muscles, grafting of extensor indicis tendon is the treatment of choice [10]. Whenever EIBM is present, it should be cleared to get absolutely muscle free tendon of extensor indicis for grafting. Awareness of the types of variation discussed is important for a successful surgery.
From an embryological perspective, the extensor muscle mass of the forearm develops from the mesoderm of the forelimb. The radial part of the mesoderm on the extensor aspect divides into a superficial and a deep part. The deep part gives rise to the abductor pollicis longus and the extensor pollicis brevis on the radial side, the extensor pollicis longus and the extensor indicis on the ulnar side [2]. According to studies, extensor indicis seems to be phylogenetically unstable and is inclined to considerable evolutionary changes as is observed by the significant variation in its expression in different species of primates [11]. Presence of EIBM in the present case report could be one such variation.
Conclusion
Interpreting unusual clinical presentations of the dorsum of hand requires in-depth understanding of anatomical variations of the musculoskeletal system. Clinicians must be aware of the kind of variation seen in this case report so as to correctly diagnose the patient with unusual pathological presentation of dorsum of hand. The surgeons should also know about the existence of EIBM to obtain a clean graft of the tendon of extensor indicis for reparative surgeries.
[1]. Natsis K, Levva S, Totlis T, Anastasopoulos N, Paraskevas G, Three-headed reversed plamarislongus muscle and its clinical significanceAnnals of Anatomy 2007 189:97-101. [Google Scholar]
[2]. Tan ST, Smith PJ, Anomalous extensor muscles of the hand: a reviewJ Hand Surg Am 1999 24(3):449-455. [Google Scholar]
[3]. Baker J, Gonzalez MH, Snapping wrist due to an anomalous extensor indicis proprius: a case reportHand 2008 3:363-65. [Google Scholar]
[4]. Yoshida Y, Anatomical study on the extensor digitorumprofundus muscle in the JapaneseOkajimas Folia Anat Jpn 1990 66(6):339-53. [Google Scholar]
[5]. Standring Susan, Gray’s Anatomy; The anatomical basis of clinical practice 2008 40th ednNew YorkElsevier Churchill Livingstone:851 [Google Scholar]
[6]. Arathala R, Sankaran PK, Ragunath G, Harsha SS, Sugumar TS, The extensor indicis brevis – a rare variation and its significanceJ Clin Diagn Res 2016 10(2):AD03-AD04. [Google Scholar]
[7]. Cauldwell EW, Anson BJ, Wright RR, The extensor indicisproprius muscle. A study of 263 consecutive specimensQ Bull Northwest Univ Med Sch 1943 17:267-79. [Google Scholar]
[8]. Antonio A, Extensor digitorum brevis manus associated with a dorsal wrist ganglion. Case ReportClin Anat 2008 21(8):794-95. [Google Scholar]
[9]. Hoffman J, Ellison MR, Extensor digitorumbrevismanus in the nondominant hand of two brothersJ Hand Surg Am 1987 12(2):293-94. [Google Scholar]
[10]. Gonzalez MH, Weinzweig N, Kay T, Grindel S, Anatomy of the extensor tendons to the index fingerThe Journal of Hand Surgery 1996 21(6):988-91. [Google Scholar]
[11]. Abu-Hiljleh MF, Bilateral extensor mediidigiti: a rare anatomical variationJournal of Hand Surgery 1993 18(5):579-82. [Google Scholar]