Treatment of Three-and Four-Part Proximal Humerus Fractures by MultiLoc Nailing Technique- A Prospective Study
Gaurav Mahesh Sharma1, Lokesh Gudda Naik2, Waghchoure Chaitanya3, Sushant Chavan4, Kunal Roy5, Prashant Pawar6, Akshay Bhardwaj7, Kalyan Tadepalli8
1 Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
2 Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
3 Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
4 Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
5 Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
6 Resident, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
7 Senior Resident, Department of Orthopaedics, Lokmanya Hospital, Pune, Maharashtra, India.
8 Resident, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Gaurav Mahesh Sharma, Clinical Associate, Department of Orthopaedics, Sir HN Reliance Foundation Hospital, Mumbai-400004, Maharashtra, India.
E-mail: sharmagaurav@live.com
Introduction
Proximal humerus fractures are third most common fractures with lack of proper consensus for treatment, especially in three-and four-part fractures. With the advent of Multiloc technique, the advantages of nailing can be successfully applied to the proximal humerus fractures.
Aim
To assess the functional and radiological outcome in three-and four-part fractures treated with Multiloc nailing.
Materials and Methods
A prospective study patients over a period of two years between December 2013 and February 2015 was conducted on 21 patients with proximal humerus fracture treated with Multiloc nailing system. Patients with three-and four-part fractures above 60 years were included in the study and regular follow-ups were done till the end of two years.
Results
The most common mechanism of injury was fall comprising of 15 (71.4%) cases followed by Road Traffic Accident (RTA) with six (28.6%) cases. As per Neer’s classification, 13 (61.9%) cases had three-part and eight (38.1%) cases had four-part fracture respectively. Mean operative time was 112±8.6 minutes. The average duration of hospital stay was 4.6±1.3 days. Radiological union was seen at 13±2.6 weeks. There was one (4.7%) case with varus collapse. Two (9.5%) cases had shoulder impingement in the present study. The mean Constant shoulder score was 61±12.4. The final outcome was measured using the Constant scoring system. There were 8 (38.2%) excellent, 9 (42.9%) good, 2(9.5%) satisfactory, 1 (4.7%) fair and 1 (4.7%) poor case respectively.
Conclusion
MultiLoc nailing is a good angular stable device which gives a secure fixation in communited three-and four-part fractures especially in osteoporotic bones.
Radiological, Road traffic accident, Shoulder
Introduction
Proximal humerus fractures are third most common fractures in elderly after neck femur and distal end radius fractures [1,2]. This fracture accounts for approximately 5% of all the fractures with a predilection towards female gender which can be between 73% and 85% [2-4]. This fracture is more common in geriatric population with low energy trauma and osteoporosis as a predisposing factor. Stable fractures can be treated conservatively whereas, unstable fractures with dislocation warrant surgery. Conservative treatment has been associated with complications like nonunion, malunion, stiffness, post-traumatic arthrosis.
Albeit various surgical options have been proposed for this fracture namely, pinning, suture or wire fixation, plating, intramedullary nailing and arthroplasty, no evidence till date has proved the superiority of one modality over another [5,6]. Intramedullary nailing techniques have been evolving continuously since past four decades from first generation rush nails to the recently introduced third generation nails like Proximal humerus nail and Multiloc nailing system. Nails apart from being load sharing devices have a better rotational control, better soft tissue respect and preserve the precarious blood supply. Nailing has been associated with problems like impingement, rotator cuff dysfunction and malunion. However, with the third generation nails, these complications have reduced significantly. The aim of the present study was to study the functional and radiological outcome of patients with three-and four-part proximal humerus fractures treated with Multiloc nailing system.
Materials and Methods
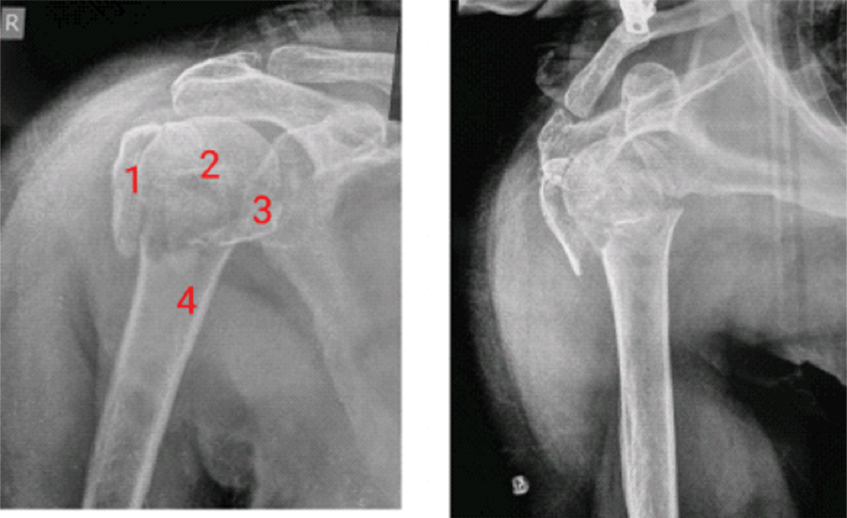
A prospective study was conducted on 21 patients with proximal humerus fracture treated with Multiloc nailing system between December 2013 and February 2015 at a tertiary care hospital. The inclusion criterion was patients above the age of 60 years with three-or four-part proximal humerus fracture. Patients with one-and two-part humerus fractures, compound and pathological fractures, history of previous shoulder surgery, pre-existing shoulder pathology like rotator cuff arthropathy were excluded from the study. Once the patient met up the required criteria, further investigation in the form of antero-posterior [Table/Fig-1] and axial radiograph along with CT scan of the affected shoulder with Three Dimensional (3D) reconstruction was done. All the fractures were classified as per the Neer classification system [7]. All the patients were operated using the MultiLoc® Proximal Humerus Nail (Synthes-DePuy, West Chester, USA) by a senior orthopaedic consultant.
Preoperative AP and Lateral radiograph.
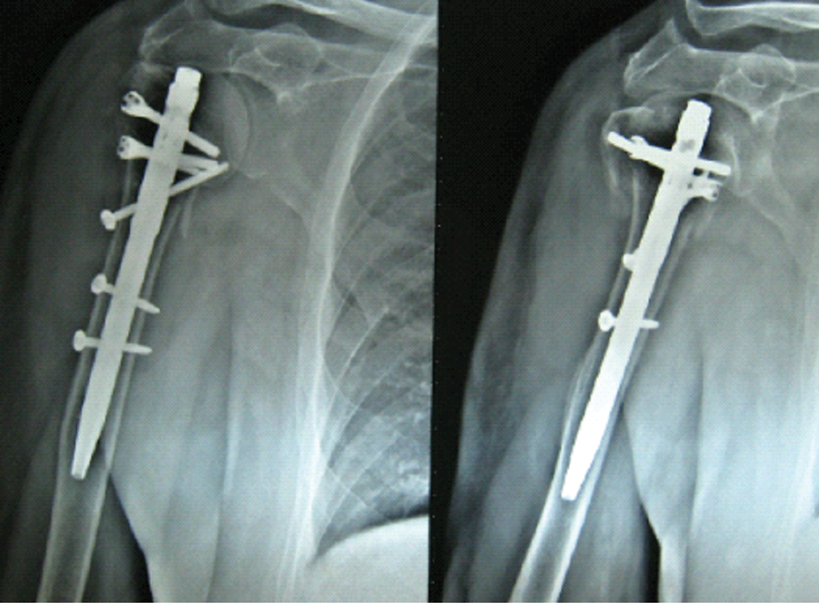
Written consent was obtained from all the enrolled patients. Prior ethical committee approval was obtained before the commencement of the study. Regular follow-up was done for all the patients at one, three, six, 12 and 24 months respectively [Table/Fig-2]. Final outcome was done using the Constant scoring system [8,9]. This system is independent of the diagnostic or radiographic abnormality and assesses the clinical functionality of the shoulder, making it widely acceptable and easy to apply. It is divided into two parts namely the subjective findings which includes assessment of severity of pain, activities of daily living and working in various positions. The second part comprises of the objective measurements like active range of movements in forward flexion, extension, external and internal rotations. The former has 35 while the latter has 65 points respectively [10]. The final results were determined as excellent (>90), good (89-80), satisfactory (79-70), fair (69-60) and poor (<59).
Surgical Technique
All the patients were operated under general anaesthesia combined with interscalene block in beach chair position. After preparing the shoulder, anterolateral deltoid splitting approach was used. Closed reduction of the fracture was done Under C-arm image intensifier by using K-wires as joysticks. Reduction sutures comprising of the small fragments were used as and when required, especially in cases with 4-part fractures. The ideal entry point for this nail is the apex of the humeral head, which is usually a part of the fracture, especially in three- and four-part fractures. Thus, a guide wire was passed after the provisional reduction was done through the fracture site, in the line of the medullary canal. The straight MultiLoc humerus nail was then mounted over the zig and inserted over the guide wire as per the determined diameter of the canal. This nail usually comes in two diameters- 8mm and 9.5mm with a length of 160mm. The proximal multiple locking was done using the 3.5mm and 4.5mm screw in screw. Ascending screws were then inserted followed by distal locking. The repair of the cuff was done using the holes in the proximal screws and the wound was closed over layers. Postoperatively, the patients were kept in a sling and passive range of movements was started after 24 hours. Patients were assessed clinically and radiologically at 1,3,6,12 and 24 months respectively.
Results
The mean age of the patients was 61.2±3.8 years. There were seven (33.34%) males and 14 (66.6%) females in the present study. Nine (42.8%) cases had right sided limb involvement whereas, left side was involved in 12 (57.2%) cases. The most common mechanism of injury was fall comprising of 15 (71.4%) cases which was followed by RTA with six (28.6%) cases. As per the Neer’s classification system, 13 (61.9%) cases had three-part and eight (38.1%) cases had four-part fracture respectively.
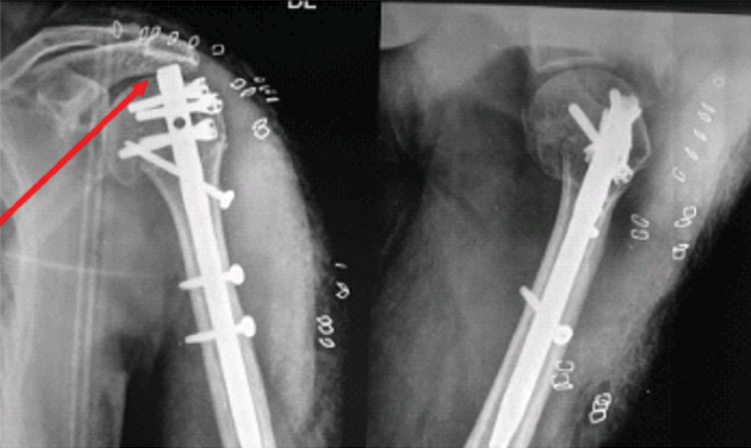
Mean operative time was 112±8.6 minutes. The surgical time was more in initial cases due to the steep learning curve in the surgical technique which declined in subsequent cases. The average duration of hospital stay was 4.6±1.3 days. Serial radiographs were done for all the patients enrolled in the study. Radiological union was seen at 13±2.6 weeks. There was one (4.7%) case with varus collapse (Neck-shaft angle <120°) which showed malunion [Table/Fig-3]. There were no clinical symptoms and thus, no active intervention was done for the same. Two (9.5%) cases had shoulder impingement in the present study. There was one (4.7%) case in which there was articular surface intrusion of the screw, which was removed at a later date after six months. The mean Constant shoulder score was 61±12.4 in the operated shoulder which was 79% compared to the non-operated shoulder at the end of 24 months. The final outcome was calculated using the constant scoring system which showed eight (38.2%) cases as excellent, nine (42.9%) cases as good, two (9.5%) cases as satisfactory and one (4.7%) case as fair and poor respectively [Table/Fig-4,5].
Clinical outcome and range of movements at the end of 24 months.
| Parameter | Finding |
|---|
| Forward flexion | 133±400 |
| Lateral elevation | 122±470 |
| External rotation | 27±130 |
| Constant score | 61±12.4 |
Functional outcome as per the Constant score.
| Score | Finding (%) |
|---|
| >90 (Excellent) | 8 (38.2) |
| 89-80 (Good) | 9 (42.9) |
| 79-70 (Satisfactory) | 2 (9.5) |
| 69-60 (Fair) | 1 (4.7) |
| <59 (Poor) | 1 (4.7) |
Discussion
Traditionally, the preferred modality of treatment for fixation of three- and four-part proximal humerus fractures has been angular stable locking plates with the use of intramedullary nails reserved for two-part fractures.
The proximal humerus is an area of spongy bone where severe comminution with soft tissue destruction can lead to further collapse. Secondary loss of fixation followed by screw cut-out are the two most common reasons for the failure in these fractures [6,11]. These are more commonly seen in patients where plating is contemplated [12,13].
Unlike tibia and femur, where the interlock nailing is considered as gold standard, nailing in humerus fractures has come a long way due to its unique anatomical peculiarities. Antegrade nailing has been associated with complications such as difficulty in reduction, rotator cuff morbidity, iatrogenic fracture at the entry site and fixation failure due to severe osteoporosis and lack of orientation [14-16].
The second generation nailing techniques had better rotational control with good radiographic and clinical outcomes than the first generation ones [17]. However, lack angular stability, inappropriate design for the osteoporotic bone, lateral entry point and rates of malunion as high as 50% [18]. Third generation nails like Proximal humerus nail and MultiLoc nailing system were introduced to alleviate these problems. They have better angular stability, screw in screw technology for better fixation in osteoporotic bones, countersunk heads, blunt screw tips to reduce the chances of secondary perforation at a later date and calcar ascending screw for the posteromedial region with a better bone density area [14,19-21]. It has been observed that nails with an inbuilt varus bend are likely to displace the fracture into a neck shaft angle of less than 1200 which can lead to fixation failure and screw loosening [14,22].
Various studies have demonstrated the rate of screw loosening and back-out to be between 4% and 26% in curved nails like Polarus as compared to straight nails like MultiLoc [14,17]. There was no case of screw loosening or break-out in the present study. Nails with more medial entry point avoids the critical hypovascular myotendinous zone and thus, protects the rotator cuff muscles [14,23]. There was one case in the present study with varus collapse (neck shaft angle <120°). This can be attributed to the fact that the entry point was more medial in this case which led to this deformity. Although, the fracture had malunion, there was minimal restriction of movements at the last follow up.
A study by Lopiz et al., Dilisio et al., and Hao et al., showed good outcome with MultiLoc nailing with a constant score of 61, 66 and 75.5±12.1 respectively [14,19,24]. The constant score in the present study of 61±12.4 can be compared to these a forementioned studies.
Smaller sample size and less duration of follow-up remains the limitations of the present study. We believe that the late complications like a vascular necrosis are evident at a later stage after four to five years and thus, longer duration of follow-up is required to see this delayed complication.
Conclusion
Straight MultiLoc humerus nail gives a benefit of better angular stability even in severely communited fractures with better preservation of the fracture anatomy and maintaining the biomechanics. This nail gives a better functional and radiological outcome. However, further systematic reviews and RCT’s needs to be done to come to a proper consensus.
[1]. Calvo E, Morcillo D, Foruria AM, Redondo-santamaria E, Osorio-picorne F, Careiro JR, Non displaced proximal humerus fractures: High incidence among outpatient-treated osteoporotic fractures and severe impact on upper extremity function and patient subjective health perceptionJ Shoulder Elbow Surg 2011 20(5):795-801. [Google Scholar]
[2]. Court-Brown CM, Caesar B, Epidemiology of adult fractures: a reviewInjury 2006 37(8):691-97. [Google Scholar]
[3]. Bell JE, Leung BC, Spratt KF, Koval KJ, Weinstein JD, Goodman DC, Tosteson AN, Trends and variation of incidence, surgical treatment and repeat surgery of proximal humerus factures in the elderlyJ Bone Jt Surg 2011 93(2):121-31. [Google Scholar]
[4]. Maier D, Jager M, Strohm PC, Sudkamp NP, Treatment of proximal humerus fractures- a review of current concepts enlightened by basic principlesActa Chair Orthop Traumatol Cech 2012 79(4):307-16. [Google Scholar]
[5]. Konard G, Audige L, Lambert S, Hertel R, Sudkamp NP, Similar outcome for nail versus plate fixation of three-part proximal humerus fracturesClin Orthop Relat Res 2012 47(2):602-09. [Google Scholar]
[6]. Helfen T, Siebenburger G, Mayer M, Bocker W, Ockert B, Haasters F, Operative treatment of two-part surgical neck fractures of the proximal humerus in the elderly: Cement augmented locking plate philos vs. proximal humerus nail MultilocBMC Musculoskelet Disord 2016 17(1):448 [Google Scholar]
[7]. Neer CS 2nd, Displaced proximal humerus fractures. I. Classification and evaluationJ Bone Joint Surg Am 1970 52(6):1077-89. [Google Scholar]
[8]. Constant CR, Murley AH, A clinical method of functional assessment of the shoulderClin Orthop Relat Res 1987 214(4):160-64. [Google Scholar]
[9]. Constant CR, Gerber C, Emery RJ, Sojberg JO, Gohlke F, Boileau P, A Review of the constant score: modifications and guidelines for its useJ Shoulder and Elbow Surg 2008 17(2):355-61. [Google Scholar]
[10]. Katolik LI, Romeo AA, Cole BJ, Verma NN, Hayden JK, Bach BR, Normalization of the constant scoreJ Shoulder Elbow Surg 2005 14(3):279-85. [Google Scholar]
[11]. Ockert B, Siebenburger G, Kettler M, Braunstein V, Mutschler W, Long term functional outcomes (median 10 years) after locked plating for displaced fractures of the proximal humerusJ Shoulder Elbow Surg 2014 23(8):1223-31. [Google Scholar]
[12]. Foruria AM, Carrascal MT, Revilla C, Munera L, Sanchez-Sotelo J, Proximal humerus fracture rotational stability after using a locking plate or a fixed angle locked nail: the role of implant stiffnessClin Biomech 2010 25(4):307-11. [Google Scholar]
[13]. Lekic N, Montero NM, Takemoto RC, Davidovitch RI, Egol KA, Treatment of two part proximal humerus fractures: intramedullary nail compared to locked platingHSS J 2012 8(2):86-91. [Google Scholar]
[14]. Lopiz Y, Garcia-Coiradas J, Garcia-Fernandez C, Marco F, Proximal humerus nailing: a randomized clinical trial between curvilinear and straight nailsJ Shoulder Elbow Surg 2014 23(3):369-76. [Google Scholar]
[15]. Falker JK, Hogan C, Heyde CE, John T, Current concepts in the treatment of proximal humerus fracturesOrthopaedics 2008 31(1):42-51. [Google Scholar]
[16]. Murray IR, Amin AK, White TO, Robinson CM, Proximal humeral fractures: Current concepts in classification, treatment and outcomesJ Bone Joint Surg Br 2011 93(1):1-11. [Google Scholar]
[17]. Rajasekhar C, Ray PS, Bhamra MS, Fixation of proximal humeral fractures with polarus nailJ Shoulder Elbow Surg 2001 10(1):7-10. [Google Scholar]
[18]. Nolan BM, Kippe MA, Wiater JM, Nowinski GP, Surgical treatment of displaced proximal humerus fractures with short intramedullary nailJ Shoulder Elbow Surg 2011 20(8):1241-47. [Google Scholar]
[19]. Dilisio MF, Nowinski RJ, Hatzidakis AM, Fehringer EV, Intramedullary nailing of the proximal humerus: evolution, technique and resultsJ Shoulder Elbow Surg 2016 25(5):e130-38. [Google Scholar]
[20]. Hessmann MH, Nijs S, Mittlmeier T, Kloub M, Segers MJ, Winkelbech V, Blauth M, Internal fixation of fractures of proximal humerus with the Multiloc nailOper Orthop Traumatol 2012 24(4-5):418-31. [Google Scholar]
[21]. Brianza S, Roderer G, Schiuma D, Schwyn R, Scola A, Gebhard F, Tami AE, Where do locking screws purchase in humeral head?Injury 2012 43(6):850-55. [Google Scholar]
[22]. Agel J, Jones CB, Sanzone AG, Camuso M, Henley MB, Treatment of proximal humerus fractures with polarus nail fixationJ Shoulder Elbow Surg 2004 13(2):191-95. [Google Scholar]
[23]. Garcia Coiradas J, Rodriguez-Niedenfuhr M, Lopiz Y, Garcia-Fernandez C, Sanudo JR, Vazquez T, A new straight proximal humerus nail: a cadaveric study of its anatomical relationshipsEur J Anat 2012 16(3):184-89. [Google Scholar]
[24]. Hao TD, Huat AWT, Surgical technique and early outcomes of intramedullary nailing of displaced proximal humeral fractures in an Asian population using a contemporary straight nail designJ Orthop Surg (Hong Kong) 2017 25(2):1-9. [Google Scholar]