Surveillance systems play an important role in disease epidemiology. Retrospective evaluation of the surveillance data, are a scientific tool for suspecting impending outbreaks and also inform us about the available management logistics. These systems incorporate standards such as the syndrome approach for eliciting a disease, the probable clinical case definition and the approved diagnostic techniques [1]. Event based surveillance systems are an important source of epidemiological intelligence [2,3]. Most of the outbreaks reported and investigated by World Health Organization derive information from case studies and informal analysis [4]. The powerful surveillance capability of the disease surveillance programmes, complementing the traditional surveillance approaches, is of immense public health usage. The Centre for Disease Control and Prevention (CDC) surveillance system evaluation guidelines [5] and CDC evaluation guidelines for outbreak detection system assist in the methodology of the scientific applications of surveillance data which is reflecting the impacts of a disease on the human health [6].
Although, many areas of the world have not reported Dengue for continuous 20 or more years and several areas have no known history of the disease [7], still the epidemiological challenge and international response for prevention and control of Dengue found elsewhere in the world derive mileage from the various components of the different Dengue surveillance systems, functioning worldwide [8]. Retrospective data analysis of the dengue surveillance system identifies the potential triggers of imminent outbreak [9]. The study of surveillance systems reveal that the first clinically recognised dengue epidemics occurred almost simultaneously in Asia, Africa and North America in the 1780s [10,11]. Systematic analysis of surveillance data has been used to estimate burden of Dengue in south-East Asia [12]. India is a developing country with fast urbanisation and industrial growth rate has poor water resource management. This has caused many outbreaks of dengue across the country.
IDSP launched in 2004 captures, apart from the other diseases, the information on water borne diseases and outbreaks across the country [13]. In India, the first epidemic of clinical dengue-like illness was recorded by the surveillance system in Chennai in 1780 and the first viralogically proved epidemic of dengue fever occurred in Kolkata and Eastern Coast of Indian subcontinent in 1963-1964 [14]. The Dengue surveillance data collected under the domains of IDSP helped to predict the outbreaks of dengue in Tamil Nadu, a southern state of India and identified the gaps to recommend the strengthening of the surveillance system [15].
Today about 2.5 billion people, or 40% of the world’s population live in areas where there is a risk of dengue transmission and District Solan is one such area. Rapid industrialisation in the district involves the migrant population dynamics which contribute more to the disease epidemiology [16].
Outbreaks of Dengue had been reported in the adjoining areas of Chandigarh, Haryana and Punjab [17]. These areas border the Shivalik hill regions of Solan district. In these hill regions, the sporadic cases of the dengue had been reported in the recent years, especially in the highly industry dominated areas of Nalagarh, Baddi, Barotiwala and Parwanoo (an approximate elevation of 4000 feet above sea level), usually during the season when Aedes mosquito populations were high, often when rainfall was optimal for breeding. Occurrence of Dengue fever in association with traveling into the non-endemic hilly regions of the state has been assessed in the past [18]. However, outbreak of Dengue had not been reported from these hilly regions in the past. Henceforth the following study was proposed with the objectives to assess any impending outbreak of Dengue in the region by using IDSP surveillance data and to assess the need based mitigation measures.
Materials and Methods
It was a cross-sectional study. The routine epidemiological surveillance data of the year 2015, under the IDSP cell of the Solan district, was assessed at the office of the Chief Medical Officer Solan, the district headquarters. Weekly surveillance data was being sent routinely to the District Surveillance Unit by the 14 Primary Health Centres (PHCs) of these regions through e-mail. To investigate about any impending outbreak, the retrospective epidemiological surveillance data of the district was analysed. Thereafter, regular surveillance by the IDSP reporting portal was initiated for the year 2015 and daily reporting was made mandatory for the Public Health Institutes {14 PHCs, one First Referral Hospital (RH) and one Community Health Centre (CHC)} functioning in these regions. An epidemiological spot map was prepared. Thereafter, the standard case definition of Dengue, as formulated by the IDSP i.e., a probable case of Dengue is defined as one presenting with acute febrile illness of two to seven days duration with two or more of the manifestations such as headache, retro-orbital pain, arthralgia, myalgia, rash, haemorrhagic manifestations, leucopenia, being detected positive by the Rapid Diagnostic test, was circulated amongst all clinicians of the region. All the suspected patients of the different regions falling under Baddi, Barotiwala, Nalagarh and Parwanoo were thereafter evaluated for Dengue. The only available test i.e., Rapid diagnostic test/Card test, highlighting the probable Dengue cases, were started in the health facilities such as CHC Nalagarh, CHC Baddi, ESI Hospital Parwanoo, Regional Hospital Solan and PHC Barotiwala. An ELISA based diagnostic facility was set up at the State Medical College, about 100 kilometers away from the affected areas of Baddi, Barotiwala, Nalagarh and Parwanoo (the industrial regions of the district). A confirmed case was defined as the one found positive with either the NS1Ag or ELISA based IgM tests done at this Medical College testing centre.
Entomological survey of the suspected breeding sites of the vector was undertaken. Establishing laboratory evidence is an important criteria defined under the IDSP Dengue surveillance. Hence, an entomologist from another department (Department of Entomology, University of Horticulture and Forestry, Nauni, Solan) was roped in for eliciting the laboratory evidence of the suspected vector involved. . House Index (Number of houses infected per 100 houses visited), Container Index (Number of Water- holdingcontainers per 100 containers inspected) and Breteau Index (Number of positive containers per 100 houses inspected) were calculated. Sanitation and cleanliness drive was extensively taken up in the regions for cutting the chain of disease transmission by the local administrative units such as the Zila Parishad and the Municipality Department. The surveillance activities were carried out by the multi-purpose workers of the health blocks of Nalagarh and Dharampur in the identified spots/regions of the area between June and November, 2015.
Statistical Analysis
The Chi-square statistical tests were used and the p-value of less than 0.05 was considered as significant. The data was analysed in Microsoft Office Excel 2010 and Epi Info software Version 7.2.0.1.
Results
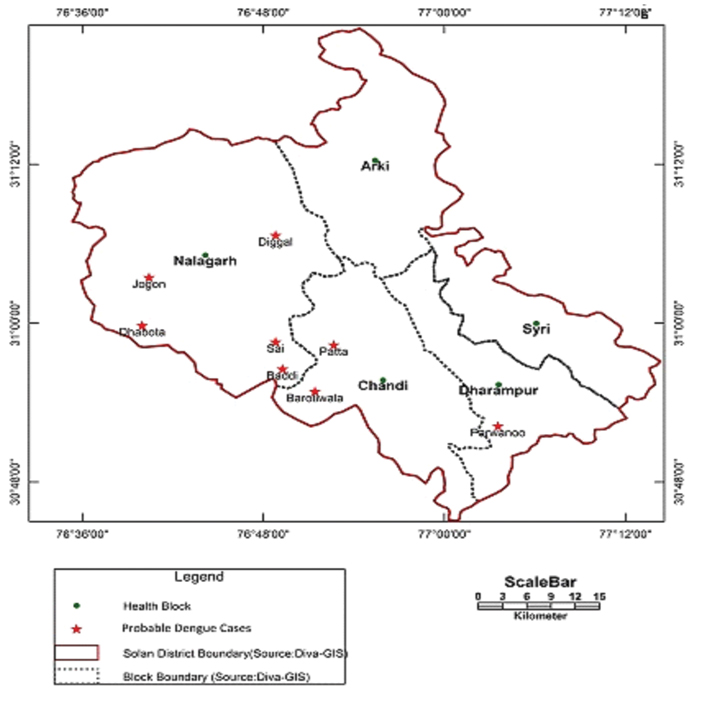
Routine surveillance data analysis revealed that the month of June, year 2015, witnessed a few cases of an illness similar in features resembling Dengue fever, amongst the masses in a densely populated area of about 2.7 lacs inhabitants in the industrial regions of the Solan district, Himachal Pradesh, India. Retrospective epidemiological data analyses showed that few cases of Dengue, being tested by the card test had been reported in these areas in the 2013 and 2014 also. The daily reporting in IDSP Portal by four main peripheral units led to the suspicion of an impending outbreak of Dengue in defined areas of Baddi, Barotiwala, Nalagarh and Parwanoo. The surveillance helped in identifying the early warning signals of impending Dengue outbreak in the regions of Baddi, Barotiwala, Nalagarh and Parwanoo. The epidemiological spot map showed the existence of probable cases in the industry dominated areas such as the villages Dhabota, Jogon, Diggal, Sai and Baddi of Block Nalagarh, Patta and Barotiwala towns of Block Chandi and Parwanoo town of the health block Dharampur [Table/Fig-1]. Warning signal report of Dengue outbreak (as envisaged in IDSP) was submitted to State Headquarters on 1st September. On 7th September, after analysing the data, the existing situation was declared as Dengue epidemic.
Spot map for epidemiological linkage of sporadic probable cases of Dengue.
The clinicians in the district followed the probable case definition for the identification of Dengue cases. [Table/Fig-2] showed the retrospective comparison and the rising trend of the positive cases detected by the rapid diagnostic test/card test from 15.6% positive cases in the year 2013 with no mortality to 25.11% positive cases with two deaths reported.
Year wise description of probable Dengue cases tested by Rapid diagnostic test/Card test.
| S. No | Year | Number of tests performed | No of positive Cases | No of Deaths reported |
|---|
| 1 | 2013 | 217 | 34 (15.6%) | 0 |
| 2 | 2014 | 90 | 2 (2.2%) | 0 |
| 3 | 2015 (as on 30/11/15) | 2732 | 686 (25.11%) | 2 |
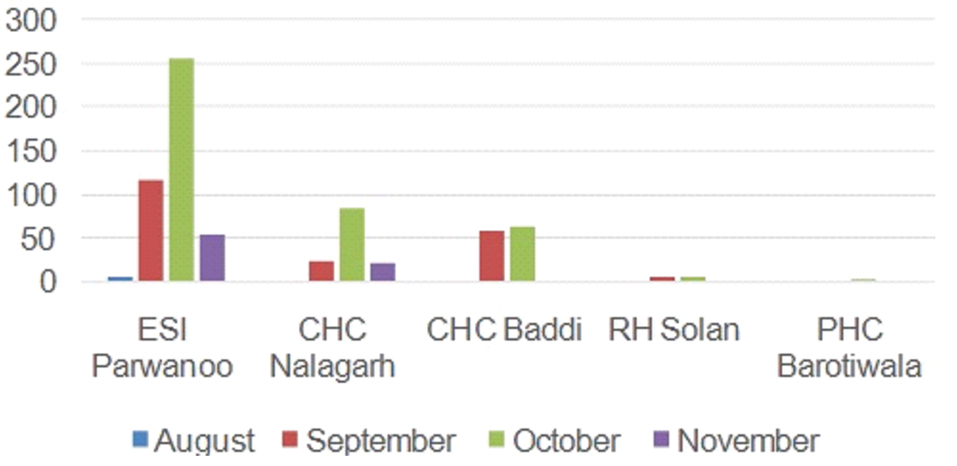
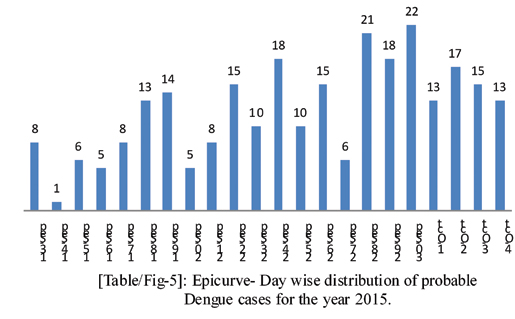
In the year 2015, the distribution of the cases diagnosed with regard to age and sex, was found statistically non-significant with p-value of 0.22 [Table/Fig-3]. A large number of probable cases were diagnosed in the first week of October at ESI hospital Parwanoo, CHC of Nalagarh and Baddi [Table/Fig-4]. The daily surveillance further revealed that a large number of cases were reported in the last and first week of September and October respectively. This Epicurve indicated a propagated source of infection in the region [Table/Fig-5].
Month wise probable cases of Dengue tested by card test.
| SN | Name of Testing Unit | 0-15 Y* | 16-30 Y | 31-45 Y | 46-60 Y | 61-75 Y | Total |
|---|
| M | F | M | F | M | F | M | F | M | F | M | F |
|---|
| 1 | ESI Parwanoo | 39 | 32 | 147 | 71 | 81 | 40 | 8 | 5 | 2 | 2 | 277 | 150 |
| 2 | CHC Nalagarh | 10 | 7 | 42 | 10 | 32 | 12 | 4 | 5 | 4 | 1 | 92 | 35 |
| 3 | CHC Baddi | 12 | 9 | 37 | 26 | 13 | 13 | 4 | 4 | 1 | - | 67 | 52 |
| 4 | RH Solan | - | - | 6 | - | 1 | - | - | - | 1 | - | 8 | 0 |
| 5 | PHC Barotiwala | - | - | - | - | - | 1 | - | 1 | - | - | 0 | 2 |
| Total | 61 | 48 | 232 | 107 | 127 | 66 | 16 | 15 | 8 | 3 | 444 | 239 |
Y*- age in years, ESI- Employees State Insurance Hospital
Month wise distribution of probable Dengue cases for the year 2015.
Epicurve- Day wise distribution of probable Dengue cases for the year 2015.
Entomological surveillance through intensive house to house search for the larvae of Dengue was conducted in the regions of Baddi, Nalagarh and Parwanoo. [Table/Fig-6] showed that House Index was higher in Nalagarh (37.5%) than Baddi (19.58%) and Parwanoo area (10.13%) and this difference was found to be statistically non significant with p-value of 0.27 (the area of Barotiwala was not included for the lack of manpower and the time constraint). The Container index was 1.35%, 4.48% and 10.34% and the Breteau Index was 10.13%, 23.33% and 48.33% respectively in Parwanoo, Baddi and Nalagarh region and the difference across the places was found non-significant with p-values for Container Index and Breteau Index being 0.32 and 0.35 respectively.
Larval density in Dengue affected area of Solan district.
| Parwanoo |
|---|
| Name of the area | Houses Checked | Positive | Container Checked | Positive | House Index | Container index | Breteau Index |
|---|
| PondSlumArea | 5 | 1 | 41 | 1 | 20 | 2.43 | 20 |
| Taksaal Area | 15 | 0 | 76 | 0 | 0 | 0 | 0 |
| EisherGateArea | 26 | 1 | 154 | 1 | 3.84 | 0.64 | 3.84 |
| SewagramArea | 12 | 2 | 86 | 2 | 16.66 | 2.32 | 16.66 |
| Total | 58 | 4 | 357 | 4 | 10.13% | 1.35% | 10.13% |
| Baddi |
| WardNo. 1Area | 10 | 2 | 72 | 2 | 20 | 2.77 | 20 |
| WardNo. 2Area | 16 | 3 | 93 | 4 | 18.75 | 5.47 | 25 |
| ChakkaSlumArea | 25 | 5 | 109 | 6 | 20 | 5.5 | 24 |
| Total | 51 | 10 | 274 | 12 | 19.58% | 4.48% | 23.33% |
| Nalagarh |
| PatelNagar | 12 | 3 | 44 | 5 | 25 | 11.36 | 41.66 |
| Bengali Colony | 20 | 10 | 118 | 11 | 50 | 9.32 | 55 |
| Total | 32 | 13 | 162 | 16 | 37.5% | 10.34% | 48.33% |
| Chi- Square | 14.5 | 18.0 | 15.37 |
| p-value | 0.27 | 0.32 | 0.35 |
The cleanliness drive was undertaken in 7.52 % (1535) houses out of the total 49396 houses surveyed and 49396 person were covered under the IEC activities to cut down the chain of transmission of Dengue [Table/Fig-7].
Sanitation and IEC Activities for the containment of Dengue outbreak.
| Name of affected area visited | Description of area visited | No. of House visited in the affected areas | No of houses where cleanliness drive done | Approximate Population where IEC activities done |
|---|
| Baddi | Residential colonies | 3494 | 249 (7.10) | 10092 |
| Baddi | Slum colonies | 9613 | 519 (5.32) | 22184 |
| Nalagarh | Residential colonies | 5235 | 531 (10.14) | 15920 |
| Parwanoo | Slum colonies | 2062 | 236 (11.45) | 1200 |
| Total | 20404 | 1535 (7.52) | 49396 |
The Entomological surveillance also included the examination of 12 adult mosquitoes. These were used for the identification of the genus with the help of the available mosquito key. The Genus Aedes was identified in three specimens. Other specimens were beyond recognition since these were deformed either during collection or in the process of rearing and thus could not be identified. This finding confirmed the existence of the Aedes mosquito in the regions of Baddi and Parwanoo. The testing facility for confirming the Dengue cases was started at Indira Gandhi Medical College (IGMC) in the month of October, 2015. The samples from the testing facilities were transported in cold chain to the lone testing facility the Microbiology Laboratory of the Medical College at Shimla, India. The samples were subjected to ELISA IgM testing and NS1 Ag testing on the basis of the availability of these respective kits at the testing laboratory. A total of 34 males and 23 females were positive for NS1Ag whereas 76 males and 33 females tested positive for IgM ELISA test [Table/Fig-8].
Confirmed cases of Dengue by NS1 Ag and ELISAIgM Tests done at IGMC, Shimla.
| S.No | NS1 Ag | IgM |
|---|
| Positive | Negative | Equivocal | Total | Positive | Negative | Equivocal | Total |
|---|
| Male | 34 | 113 | 12 | 159 | 76 | 22 | 1 | 99 |
| Female | 23 | 58 | 3 | 84 | 33 | 17 | 2 | 52 |
| Grand Total | 57 | 171 | 15 | 243 | 109 | 39 | 3 | 151 |
The surveillance feedback also led to intensive fogging with Pyrethrum, in 1135 and 262 households of Baddi and Nalagarh regions respectively [Table/Fig-9]. Simultaneously the fogging of insecticides was also undertaken by other Departments such as Municipal Committee and Zila Parishad at the areas of Baddi, Parwanoo and Nalagarh. Routine surveillance picked up the constraints in the fogging mechanisms. With a view point of having more extensive coverage in less time, the Department of Health and Family Welfare of district Solan, on the recommendations given by District Surveillance Unit, purchased and used a Vehicle Mounted Fogging Machine.
Anti-mosquito - pyrethrum fogging.
| Name of affected area covered Area | Number of Households | Number of Rooms |
|---|
| Baddi | 1135 | 1996 |
| Nalagarh | 262 | 407 |
The surveillance revealed that cleanliness and sanitation drive in the households by the health teams along with the fogging mechanism in the regions of Baddi, Nalagarh and Parwanoo drastically reduced the probable Dengue cases being diagnosed in the laboratories at Baddi, Nalagarh and Parwanoo.
Discussion
The epidemiologic surveillance is instrumental in determining the need for public health action and assessing the effectiveness of a programme. As per the guidelines prepared by Klaucke DN et al., surveillance should help in assessing whether a system or programme is serving a public health function and meeting its defined objectives or not [19]. The present study not only highlighted the utility of surveillance in eliciting the impending outbreak but also guided the mitigation activities. Administrative level meetings and training at various levels helped in evolving the management strategies for the containment of Dengue [Table/Fig-10].
Description of administrative level meetings by the stakeholders for the Dengue outbreak mitigation.
| S.No | Name of the activity | Resource person | Target audience | Remarks |
|---|
| 1 | IDSP report strengthening measures- review meeting | *CMO | BMOs, SMO I/C, MS Solan, MS Parwanoo | Strengthening of telephonic reporting and making it mandatory before onset of monsoon |
| 2 | IDSP- Hands on training for P form filling | DPO | MO, MPWs block Nalagarh, Rapid Response team members | Reporting mechanism sensitization based on probable case definition |
| 3 | Mosquito breeding -prevention measures | DPO, Under chairmanship of Deputy Commissioner Solan | Local administrative bodies like Zila Parshads and village Panchayat members | Sanitation maintenance by civic authorities |
| 4 | Mosquito borne disease sensitization workshop | DPO | All BMOs and MOs of 8 PHCs | Slot given in monthly review meeting for respective discussion of the strategic plans for breeding source reduction |
| 5 | Information education and communication | IEC Cell of NHM Solan | General public | 6000 pamphlets distributed to create awareness about malaria, dengue. |
| 6 | Preparedness review | CMO | BMOs, SMO I/C, MS Solan, MS Parwanoo | Monsoon preparedness review – vector borne disease measures control mechanisms review in the routine monthly meetings |
| 7 | Vector borne disease Sensitization | Respective BMOs | MPWs and ASHA, RRT members | Field activities to be strengthened regarding planning of fogging and temephos application areas. |
(*CMO- Chief Medical Officer, BMO- Block Medical Officer, MO- Medical Officer MS I/C- Medical Superintendent In charge, DPO- District Programme Officer, MPW- Multi Purpose Worker, ASHA- Accredited Social Health Activist.)
Graitcer PL and Burton AH in 1987 had documented in his study the usefulness of computer based surveillance systems in Epidemiologic Surveillance projects, in meeting the objectives of speed, efficiency and uniformity of reporting [20]. Our study also elicited the role of IDSP which had incorporated the electronic transmission of data as its methodology. The Epidemiological surveillance assessment report 2006 of Mozambique by WHO documents the importance of clinical identification of diseases, laboratory functioning and human resource, in outbreak management [21]. Similarly the present study exhibited how the IDSP helped in clinical case definition of probable dengue cases and the need based setting up of a laboratory centre for prompt and efficient management of the disease. Entomological surveillance in our study not only documented the existence of the vector in the region but also, by means of vector indices, guided the diagnosis and treatment apart from public health interventions such as fogging and cleanliness drive. In a similar study, Basker P et al., in 2013 has also documented the utility of entomological surveillance in prevention and control of dengue outbreak in a Southern state of India [22]. Although our study could not establish a quantifiable relationship between the vector indices calculated and the number of dengue cases, the vector indices did point out to the presence of the vector in the region and transmission of the disease Dengue. Similarly, Bowman LR et al., (2014) in a systematic review of the evidence for a relationship between the vector indices and the number of dengue cases, found that there was no quantifiable evidence to establish the relationship and had recommended for more standardized methods [23].
This study also highlights that the poorly managed and rapidly growing urbanisation has led to many water stagnation points which act as a source for the disease propagation. In a similar study by Shen SQ et al., (2015), it was shown that the rapid urbanization had led to poor water management and had led to a huge outbreak of Dengue in Guangdong, China [24].
Limitation
The cleanliness and sanitation drive suffered in Barotiwala region due to lack of manpower. Further confirmation for the species of Dengue could not be made because of the lack of a taxonomist.
Conclusion
The IDSP elicited an impending outbreak of Dengue. The routine feedback by the surveillance system did lead to early containment of the outbreak. The surveillance system also highlighted the urgent understanding of the environment dynamics which will help in the source reduction for the propagation of the vector.
It is reccomended that intensive awareness programmes for the prevention of Dengue to be undertaken, especially in the slum areas, were recommended to the District Health Department.
This study was later on made the basis for establishing ELISA based diagnostic facilities at the hospitals of Solan, Parwanoo and Nalagah. The health workers were assigned specific targets for organizing awareness camps in their respective areas.
Y*- age in years, ESI- Employees State Insurance Hospital
(*CMO- Chief Medical Officer, BMO- Block Medical Officer, MO- Medical Officer MS I/C- Medical Superintendent In charge, DPO- District Programme Officer, MPW- Multi Purpose Worker, ASHA- Accredited Social Health Activist.)