The peripheral nervous system adapts mechanically and physiologically to movements of daily life [1]. Neural dysfunction can arise from alterations in neurophysiology and mobility of the peripheral nerves [1-4]. It may reflect as mechanosensitivity which is the sensitivity of a nerve to movement and can contribute to pain during movement and/or sustained postures [5]. Clinically, a specific series/sequence of joint movements are used to evaluate and manage disorders of the peripheral nervous system [2,6]. Among the neurodynamic provocative tests used for the upper quadrant disorders, Upper Limb Neurodynamic Test 1 (ULNT-1) is reported to be evaluating most roots of brachial plexus and nerves of upper limb, with more emphasis on the median nerve [3,7]. Authors have reported the presence of normal responses in asymptomatic participants to neurodynamic testing in terms of limitation in motion, sensory and nociceptive responses [4]. While performing ULNT-1, measurement of the EEROM has shown to be a reliable objective measure to quantify mechanosensitivity [8].
The physical and physiological integrity of the peripheral nerves is essential for normal sensory and motor functions. Among various sensations carried by nervous system, vibration sensibility is one of the important aspects. It is used to detect and monitor neural dysfunction [9]. VT testing is sensitive and an early indicator of minor nerve dysfunctions as the large Aβ fibers which carry this sensation are more susceptible to depletion of blood supply than the small fibers [2,10]. VT testing has shown to be a reliable and valid method of measuring nerve function [2].
Muscle performance (force generation) depends on nerve conduction, motor unit firing characteristics and the number of motor units. Altered nerve physiology can affect muscle function. Among various measures for motor function, hand grip strength is one of the important outcome [11]. It is a simple and reliable method to check the optimum functioning of the hand [12-14].
Neural Tissue Mobilization (NTM) techniques have shown to be beneficial in situations with altered neurodynamics. Improving blood supply to the nerves, restoration of the neural elasticity and thereby, restoring axoplasmic flow were the hypothesized mechanisms to bring in the benefits [15]. Improvements were observed in terms of reduction in pain, improved grip strength, better extensibility and quality of life.
The common symptoms with altered neurodynamics such as pain and paresthesia may cloud the vibration sensibility and reduce the muscle performance/force production. Reduction in these symptoms (pain and paresthesia) [6,15-18] associated with improved neural extensibility [5,6,8,19,20] with a multimodal treatment approach incorporating NTM may facilitate vibration sensibility, muscle performance [16], and quality of life [21,22]. NTM in asymptomatic subjects with reduced neural extensibility may highlight the actual physiological responses. However, there is a paucity in literature indicating the physiological effects in such a scenario.
Hence, the aim of this study was to investigate the role of structured NTM program on neural extensibility and neurophysiological properties of the nerve in asymptomatic participants with reduced neural extensibility.
Materials and Methods
A prospective outcome assessor blinded Randomized Controlled Trial (RCT) was conducted on healthy and physically active asymptomatic university students. Following Institutional Research Committee approval, Institutional Ethics Committee (IEC 79/2015) had approved the study protocol on 12/3/2015 for a duration of one year.
Convenience sampling was adapted for recruitment of the subjects. Asymptomatic individuals with a full active range of motion in upper limb joints and having EEROM ≥ 30° during the ULNT-1 procedure when performed as per the description of David Butler were considered to be eligible to participate in the study [8,23]. Participants with a history of recent injuries (in past 6 months) and neuro-musculoskeletal involvement of upper quadrant and sensory impairments were not considered for inclusion.
Eligible participants had signed a written informed consent prior to the commencement of the study. The study involved two groups: an intervention group which received neural tissue mobilization to the median and ulnar nerve and a control group with no intervention.
Group Allocation and Blinding
The sample size was calculated using comparison of means formula. The sample size provided 80% power to detect a change of 6.7 kg on hand grip strength with an alpha level of 0.05. With an attrition rate of 20%, the minimal sample for each arm was determined to be 20.
Block randomization was performed to ensure equal distribution of participants in both the groups. Four blocks of ten participants were prepared prior to the commencement of the study by a research expert who was not involved in the study. Every block ensured five participants in each group at the completion of a block. Sequentially numbered, opaque, sealed, and stapled envelopes were used for the allocation concealment [24]. Baseline outcome measurements were taken after the group allocation by the investigator who was blinded to groups, the same investigator also performed other consecutive measurements.
Intervention
Participants in the experimental group received neural mobilization of the median and ulnar nerves on the dominant side. Interventions were delivered using ULNT-1 position for median nerve and ULNT-3 position for ulnar nerve [23]. Elbow and wrist joints were used to mobilize the neural tissues. Interventions were started and ended with a neurodynamic sliding technique. This was found to impose less strain and greater longitudinal excursion of the nerves when compared to tensioning techniques, which were performed amid sliding techniques [8,18]. The technique was applied up to or just short of the point of first symptom report (P1) by the participant or first resistance (R1) encountered by the investigator, whichever occurred first. Often P1 and R1 occurred simultaneously in our participants as reported in existing literature [4,7,25]. About 15-20 oscillations for three minutes each (Slider-Tensioner-Slider) were applied with a rest period of 20 seconds between each technique. The same dosage was applied for both the nerves. Total duration for intervention was 20 minutes/session. Five sessions of neural mobilization were delivered on alternate days over a period of 10 days.
Participants in the control group did not receive any intervention. They underwent assessment for outcome measures for the same number of time points as in the intervention group.
Outcome Measures
The outcome measures in this study were hand grip strength, VT, and EEROM. Outcomes were recorded at three-time points. Time Point -1 (TP1) is at recruitment after group allocation and before the intervention was initiated. Time Point -2 (TP2) was after the first intervention for the intervention group and after 20-minute gap following the TP1 for the control group. Time Point-3 (TP3) was on the 12th day following recruitment for both control and intervention groups. All measurements were assessed by an investigator who was blinded to group allocation. TP1 and TP2 measures were used to analyse the immediate effect and the short-term effect was analysed by comparing TP1 with TP3.
Grip Strength
Hand grip strength was measured with JAMAR hand dynamometer (Sammons Preston, Inc) which records the strength in kilograms. Measurements were taken as per American Society of Hand Therapists, in a standardized arm position for hand grip testing [12]. The subject sat with back supported, neutral adduction and rotation at the shoulder, elbow flexed to 90°, forearm in neutral position and wrist in 20°-30° extension and 10°-15° ulnar deviation. All readings were taken in second handle position and repeated thrice. Mean of the three readings was taken for analysis.
Vibration Threshold (VT)
The participant was made to sit on a chair comfortably with forearm supported on a pillow in supinated position. Practice VT was obtained from the non-dominant side on the palmar surface of the base of the second metacarpal using a biothesiometer (VibrothermDx). On the dominant side, the probe was placed perpendicular to the palmar surface of the second metacarpal head for median nerve and on the fifth metacarpal head for ulnar nerve territories [15]. The subject was asked to close eyes while performing the procedure. The onset of vibration was measured by slowly increasing the vibration stimuli until the subject was just able to perceive the vibration (VPT). The stimuli was increased by 50% above the perceived value and then slowly reduced to disappearance i.e. until the patient could no longer feel the stimulus (VDT). The procedure was repeated thrice. Average of all values (3 VPT and 3 VDT) was considered as ‘Vibration Threshold’ (VT).
Elbow Extension Range of Motion (EEROM)
EEROM was measured with the patient in ULNT-1 position. Pressure biofeedback was placed over the cephalad end of the shoulder girdle and was inflated above 40 mm Hg. Investigator maintained firm pressure on the shoulder girdle through the inflated cuff maintaining a pressure of 40 mm Hg throughout the procedure of ULNT-1. Neurodynamic provocative testing procedure (ULNT-1) was performed sequentially. Universal Goniometer was used to record EEROM in degrees by the blinded investigator at the point of P1 or R1. Fulcrum was placed on medial epicondyle; fixed arm of the goniometer was placed along the long axis of the humerus and movable arm was placed along the long axis of the ulna [26].
Statistical Analysis
Statistical analysis was performed using SPSS version 15.0. Shapiro-Wilk test was used to test the normality wherein EEROM followed a normal distribution. A repeated measure ANOVA was used to compare the means of the EEROM, and was expressed in Mean and Standard Deviation (SD). For non-parametric data i.e., Grip strength, VTs of median and ulnar nerves, Friedman’s two-way ANOVA was used to assess between groups differences and Wilcoxon Signed Rank test was used to check within group differences. As a measure of central tendency, median and interquartile ranges were used for expressing variability. Descriptive statistics was used for summarizing demographic data. The level of significance was set at p≤0.05.
Results
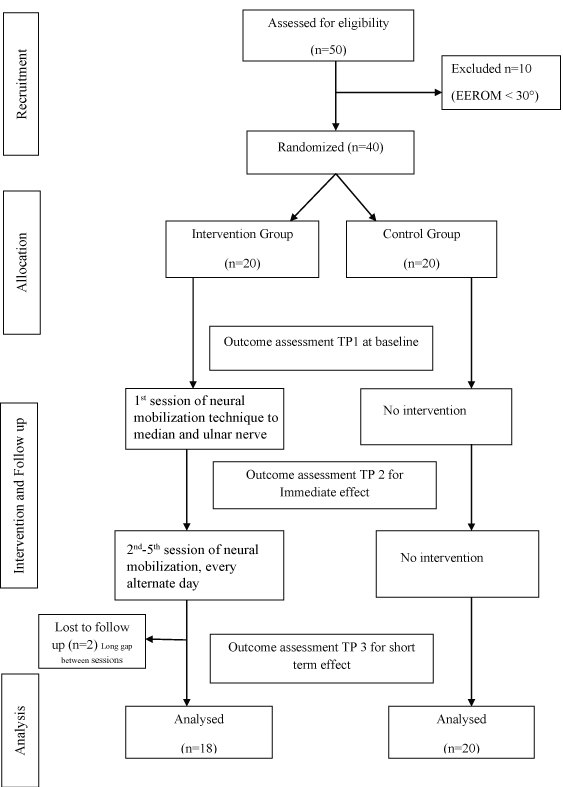
Fifty participants were screened initially out of which 40 fulfilled the inclusion criteria and were considered eligible for the study [Table/Fig-1]. Subjects were excluded (n=10) as they had EEROM < 30°. Included participants (n=40) were randomized into two groups i.e., intervention group (n=20) and a control group (n=20). Two from the intervention group failed to complete the study. Minimal differences were noted between the groups at baseline and none were statistically significant (p ≥0.05) [Table/Fig-2].
Flow diagram for participants.
Demographics and baseline characteristics for both groups.
| Parameter | Intervention group(n = 18) | Control group(n = 20) | p-value |
|---|
| Age (Years) | 22.67±1.91 | 22.40±1.98 | 0.67 |
| Sex (M/F) | 4/14 | 5/15 | |
| Height (Cm) | 160.05±9.94 | 159.06±8.00 | 0.73 |
| Weight (Kg) | 58.24±12.48 | 58.67±11.37 | 0.91 |
| EEROM (Degrees) | 46.89±10.02 | 44.70±6.77 | 0.49 |
| Grip strength (Kg) | 27 (22,36) | 27 (22,32) | 0.67 |
| VT for Median nerve (V) | 2.66 (2.12,3.33) | 2.91 (2.16,3.41) | 0.93 |
| VT for Ulnar nerve (V) | 2.74 (2.12,3.20) | 2.58 (2.00,3.00) | 0.31 |
Independent t-test for age, height, weight, EEROM and Mann-Whitney U test for grip strength, Vibration Threshold (VT) for median and ulnar nerve.
Results for comparison of grip strength between and within the groups are shown in [Table/Fig-3]. Grip strength values are expressed as median differences and interquartile range. The immediate and short-term effects have been analysed and not found to be significant. There were no statistically significant differences observed between the groups in grip strength.
Comparison of grip strength within (Wilcoxon Signed rank test) and between (Friedman’s two-way ANOVA) the groups.
| Grip strength | Within groups comparison | Between groups comparison |
|---|
| Intervention group | Control group |
|---|
| Time Point 1 | 27 (22,36) | 27 (22,32) | p=0.52 |
| Time Point 2 | 26.50 (22.75,36.70) | 27 (23,34) |
| Time Point 3 | 27 (25,35.50) | 25.5 (21,35) |
| p* | 0.72 | 0.44 |
| p’ | 0.48 | 0.81 |
p*comparison for immediate effect (TP1, TP2), p† comparison for short term effect (TP1, TP3)
Neural tissue extensibility/mechanosensitivity measured through the EEROM improved significantly in intervention group immediately (TP1, TP2) as well as in the short term (TP1, TP3). Control group also showed a significant increase, but only in short term (TP1, TP3). As reported in [Table/Fig-4], mean difference between time point 1 and 2, as well as between 1 and 3 indicate a definitive increase in EEROM.
Comparison of EEROM within and between the groups using Repeated measures ANOVA.
| EEROM | Within groups | Between groups |
|---|
| Intervention group | Control group |
|---|
| MD for immediate effect | 5.94 | 0.15 | p=0.52 |
| MD for short term effect | 12.44 | 6.35 |
| p* | 0.004 | 0.86 |
| p’ | 0.001 | 0.004 |
MD: Mean difference expressed in degrees.
p*Comparison for immediate effect (TP1, TP2), p’ Comparison for short term effect (TP1, TP3)
VT for both median and ulnar nerves reduced significantly in the intervention group after NTM (immediately as well as short term) [Table/Fig-5]. No statistically significant change was observed in VT’s of median nerve in control group. However, a significant decrease for ulnar nerve was observed only in short term (TP1, TP3). Intervention group demonstrated better improvements in VT in ulnar nerve territory compared to control group which was statistically significant.
Comparison of Vibration thresholds within (Wilcoxon Signed rank test) and between (Friedman’s two way ANOVA) the groups.
| Outcome | Within groups | Between groups |
|---|
| Intervention groupMedian (IQR) | Control groupMedian (IQR) |
|---|
| VT for Median nerve (V) | Time Point 1 | 2.66 (2.12,3.33) | 2.91 (2.16,3.14) | p=0.65 |
| Time Point 2 | 2.49 (2.00,3.00) | 2.66 (2.00,3.24) |
| Time Point 3 | 2.49 (2.00,2.54) | 2.16 (2.00,2.95) |
| p* | 0.01 | 0.15 |
| p’ | 0.02 | 0.06 |
| VT for Ulnar nerve (V) | Time Point 1 | 2.74 (2.12,3.33) | 2.58 (2.00,3.00) | p=0.009 |
| Time Point 2 | 2.41 (2.00,3.03) | 2.50 (2.16,2.95) |
| Time Point 3 | 2.16 (2.00,2.49) | 2.33 (2.00,2.95) |
| p* | 0.01 | 0.16 |
| p’ | 0.03 | 0.01 |
TP 1: Baseline, TP 2: Post 1st session, TP 3: Two days after the fifth session.
p*comparison for immediate effect, p’ comparison for short term effect
Discussion
This study aimed to investigate the effect of neural mobilization on hand grip strength, EEROM, and VT. Grip strength was not seen to be altered following five sessions of neural tissue mobilization. Previously, some studies have reported a positive effect of neural mobilization on grip strength in symptomatic individuals [27,28]. However, the baseline grip strength could have been reduced due to pain levels. The significant improvement in grip strength in those symptomatic individuals with intervention can be attributed to the reduction in pain levels. The subjects in this study being healthy individuals did not have any grip strength deficits at the baseline; hence, there would not have been much scope for increase in the readings.
Lundborg and Rydevik studied the detrimental effects on the physiology and mechanics of the neural tissue while stretching the nerve [29]. There can be autogenic inhibition and reduced contractile excitability of stretched muscle, resulting in reduced muscle strength [30]. In the present study, type of intervention delivered was mobilization of the nerves and not mere stretching. Hence, it did not show any significant detrimental effect on grip strength.
A significant decrease in EEROM in both groups was observed. This is an indicator of better extensibility of the nerves resulting from NTM [5]. This result is in line with a study performed by Mendes AC et al., where they found significant improvement in range of motion at hip joint after the treatment of neural mobilization compared with myofascial release and passive muscle stretching [31]. Similar results were also reported by Sharma S et al., who concluded that neural sliders and tensioners are effective in increasing hamstrings flexibility as an adjunct to passive hamstring stretching. Increased extensibility in the control group could have occurred due to repetitive testing to record the EEROM at three-time points resulting in NTM [5,7] leading to better extensibility. However, this change was not noticed as an immediate effect (TP1, TP2).
In the present study, VT for median nerve was reduced for the intervention group and for ulnar nerve it was reduced in both the groups. With the mobilization of the neural tissues, there could be a better reception and faster conduction of these impulses and hence, increasing the sensitivity of the nerve and reduction in thresholds. Ridehalgh C et al., found out the effect of straight leg raise examination and treatment on vibration threshold in lower limbs of asymptomatic individuals. They concluded that straight leg raise may not be detrimental to the function of large diameter vibration carrying fibers [2]. A previous research in current setting among asymptomatic individuals, identified an intersession variability of 0.23-0.52 volts. Time of the day was not found to have a significant influence on VT in the nerve territories [32]. The difference observed in the intervention group in the present study was more than the intersession variability. Hence, observed change can be considered to have occurred due to intervention.
Both groups underwent repeated testing for outcome assessment, which might have affected their values of vibration thresholds. Outcome assessment involved ULNT-1 which affects the median nerve predominantly, hence the VT in median nerve territory did not show a difference between groups. However, ulnar nerve VT demonstrated significant improvement in the intervention group. This could have resulted from NTM.
Limitation
Some limitations of this study can be listed. Activity levels of participants during the study were not controlled. Control group received indirect intervention in the form of repetitive testing (three-time points); hence, did not fulfill its role as a true reference group.
Conclusion
Neural tissue mobilization has no immediate or short-term effect on grip strength in asymptomatic subjects. However, it had improved extensibility and vibration sensibility.
Independent t-test for age, height, weight, EEROM and Mann-Whitney U test for grip strength, Vibration Threshold (VT) for median and ulnar nerve.
p*comparison for immediate effect (TP1, TP2), p† comparison for short term effect (TP1, TP3)
MD: Mean difference expressed in degrees.
p*Comparison for immediate effect (TP1, TP2), p’ Comparison for short term effect (TP1, TP3)
TP 1: Baseline, TP 2: Post 1st session, TP 3: Two days after the fifth session.
p*comparison for immediate effect, p’ comparison for short term effect