Effect of Visual Cue Training on Balance and Walking in Elderly: A Single Blind Randomized Controlled Trial
Sumam Sunny1, Suchetha PS Bhat2
1 Assistant Professor, Nitte Institute of Physiotherapy, Nitte University, Mangaluru, Karnataka, India.
2 Assistant Professor, Nitte Institute of Physiotherapy, Nitte University, Mangaluru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sumam Sunny, Nitte Girls Hostel, Opposite Shagil Precision, Deralakatte, Mangaluru-575018, Karnataka, India.
E-mail: sumam3291@gmail.com
Introduction
Balance disorders emblematize as a sprouting area of public health concern, due to its conjunction with falls amidst the elderly dwellers in the community. As age increases there is a marked reduction in functioning of visual system and gaze behaviour which adversely affects balance and gait in elderly. Balance and gait training methods aided by visual cues are technology based so the study was initiated to find about a visual cue training method which is feasible and can be used in rural settings easily amongst the elderly veterans of the community.
Aim
To determine the effect of visual cue training on balance and walking in elderly population.
Materials and Methods
The study was a single blind randomized controlled trial carried out in Abhaya Ashraya old age home, Assaigoli, Mangalore. A total of 55 patients were screened out of which 40 patients who met the inclusion criteria were enrolled in the study. All participants receive balance training for 30 minutes. In addition, the experimental group received visual cues along with balance training. Berg Balance Scale (BBS) and Dynamic Gait Index (DGI) scores were taken pre and post-treatment in both the groups. Paired and independent t-test was used for comparing within and between group difference respectively of the experimental and control group of BBS and DGI scores.
Results
There was a significant improvement in the Berg balance and Dynamic gait index scores before and after the intervention within the groups and between the groups with a p-value<0.001 in both experimental and control group but more marked improvement was found in experimental group with mean difference of 4.9 and 2.2 for BBS and DGI respectively.
Conclusion
The present study concludes that visual cue training can be utilized as a simple and effective tool for training in clinical settings to address sprouting public health issue of balance and gait disorders which is cohesively coupled with catastrophe of falls admist elderly residents in the community.
Accidental falls, Feedback, Gait, Geriatrics, Neuronal plasticity, Vision
Introduction
The process of ageing is conjoined with histological and functional mutations amongst the various systems inside the body along with decline in the physiological capacity which further heightens susceptibility to disease and lethality [1].
Elderly population can be classified as young old (60-69), the old (70-79) and the oldest old (80+) [2]. Indian population includes approximately 103.9 million elderly people, which constitutes about 8.6 percent of the total population according to the “2016 report of elderly in India” [3].
Balance is the core element required to execute functional activities in elderly population. Shkuratova N et al., assessed the variations in responses to perturbations between young and elderly adults while walking and reported that decreased stride and step length was observed amongst elderly in an attempt to guard stability when compared with young adults [4]. As age progresses there is a marked decline in functioning of visual, vestibular, proprioceptory and motor system which contributes to balance deficits in elderly. These alterations in balance expose the elderly dwellers in the community to the catastrophe of falls [5].
Vision aids walking as the information obtained through optic flow is used to place feet in accurate position while walking in various terrains [6]. As age increases, there is a decrease in contrast and glare sensitivity, dark accommodation, altered depth perception which further lowers the ability of the elderly to maintain balance and skip obstacles while walking.
Visual cues are extrinsic feedback mechanisms used to enhance motor learning [7]. Visual cue training is an intervention which provides visual cues while training balance and walking in the elderly during therapy session. Visual cues are bright contrast coloured markings used to facilitate balance and gait.
Falls betide at the interim of dynamic ambulatory activities in the elderly veterans but most of the studies in the vicinity are clogged as it is bordered to provide visual feedback training in standing hence, scarce is known regarding the impact of visual feedback training in walking. [8]. The task of walking to visual cues is extra attentionally onerous analogously with other cueing techniques. Most of the visually guided training methods are expensive hence, there is a need to find a cost-effective and feasible technique that can be used in rural settings [9].
There is exigeous evidence on the singular effect of visual cue training on balance and gait in elderly; hence, the study was undertaken with an objective to find the effect of visual cue training in elderly.
Materials and Methods
The study is a single blind randomized control trial in which subjects were blinded. Subjects were recruited from Assaigoli Abhaya Ashraya old age home, Mangaluru. The study was conducted from May 2014-June2016. The experimental hypothesis of the study was that visual cue training may be effective in training balance and gait in the elderly whereas, the null hypothesis was that visual cue training may not be effective in training balance and gait in elderly population. The Ethical clearance for the study was obtained from Central Ethical Committee of Nitte University. Participant information form was provided to the subjects before recruitment in the study in which purpose, procedure, risks as well as right of the patient to withdraw at any time and claims for any discomfort following participation in the study was mentioned clearly. Informed consent form was also taken before start of the intervention in both experimental and control groups. The sample size for the study was 40 subjects which were calculated using technique of estimation of paired t-test where the level of significance was 5%, power was 80%, effect size was 0.5, anticipated drop out was 20%. The pretest and post-test mean was 80 and 83 respectively [10]. The formula used was N= (Z1-α/2+Z1-β)2/ Δ2 + Z1-α/2/2 where Δ is effect size, α is significance level, 1- β is the power of the test. The minimum sample size obtained to conduct the study was 40 subjects.
The inclusion criteria was subjects with age group 65-74, both gender, berg balance scale score range between 40-50 [11] and mini mental status examination score between range 21-30 [12]. The study excluded subjects with orthopaedic complications like lower limb fracture preventing mobilization and arthritic disorders interfering with gait as well as subjects with cardiovascular complications and past history of any neurological disorders. People with uncorrected visual impairments preventing use of visual cue training were also excluded.
The subjects were allocated into experimental and control group using random number generator and were enclosed in sealed envelopes. Randomised block method was used wherein 40 subjects were divided in groups of 20 each. Out of 20 in each group they were further divided in groups of 10 in experimental and control group. The generation of random sequence and enrolment of participants was done by investigator but the subjects were blinded to group allocated.
All the participants received balance training for 30 minutes. In addition, the intervention group received training using visual cues. The treatment was given once for three days in a week for consecutively four weeks for 30 minutes [13]. A black chart paper 5m x 35cm consisting of bright fluorescent tapes 9 cm apart and bright fluorescent coloured cones and spherical balls were used. The exercises included:
Walking on the fluorescent marks on floor [Table/Fig-1];
Experimental group participants walking on the fluorescent marks on the floor.

Walking in a circle around cones placed;
Tandem walking on bright coloured lines on floor;
Marching on coloured lines;
Reaching forward and sideways to take the bright coloured ball in standing [Table/Fig-2];
Participant reaching forward to take the bright coloured ball in front.

Single leg standing on lines placed on floor [14].
The above mentioned exercises were given for initially five repetitions each. Progression was made by increasing the number of repetitions to 10 and the distance of reaching forward from 25 cm to 35 cm and walking time was increased in the consecutive weeks. Competitions were held amongst the members of the group to find out the subjects with maximum speed in lesser time to motivate the patients.
The safety of the members in the group was ensured by adequate lighting, maintaining clean and non-slippery floor. Bed rails were present on either side of the walking areas to prevent falls. Two physiotherapists were also present at the group session area to supervise the exercise.
Outcome Measures
Berg balance scale and dynamic gait index were used to evaluate balance and dynamic gait respectively. Baseline scores were taken of BBS and DGI before the start of intervention. After a period of four weeks BBS and DGI scores were measured again for the participants in the study. The total duration of the study is one year. The berg balance scale is a reliable and valid gold standard tool used to measure balance in elderly [15]. Total Score of Berg balance scale is 56. The berg balance scale comprises of 14 functional components. The time taken to conduct the test is approximately 15 minutes. It is a five-point scale, ranging from 0-4 wherein 0 and 4 represent lowest and highest functioning level respectively. The Dynamic Gait Index is a standardized clinical assessment tool that assists in assessing a person’s ability to alter gait in response to changing gait task demands. The DGI rates performance from 0 (severe impairment) to three (normal) on eight different gait tasks. Scores on the DGI vary from 0 to 24. A score of 19 or less, out of 24, indicates an increased risk of falling in older adults. It is considered as a reliable and valid tool to measure gait in community dwelling older adults [16].
Statistical Analysis
Statistical analysis was done using SPSS 16.00. Descriptive statistics including mean, standard deviation, percentages were done for basic characteristics of elderly subjects. Chi-square was used to calculate the significance between the sex. Paired t-test was used to compare within group difference of the intervention group and control group of BBS and DGI. The independent sample t-test was used to compare between group difference of experimental and control group after and before the treatment for BBS and DGI. A p-value less than 0.05% probability was considered to be statistically significant.
Results
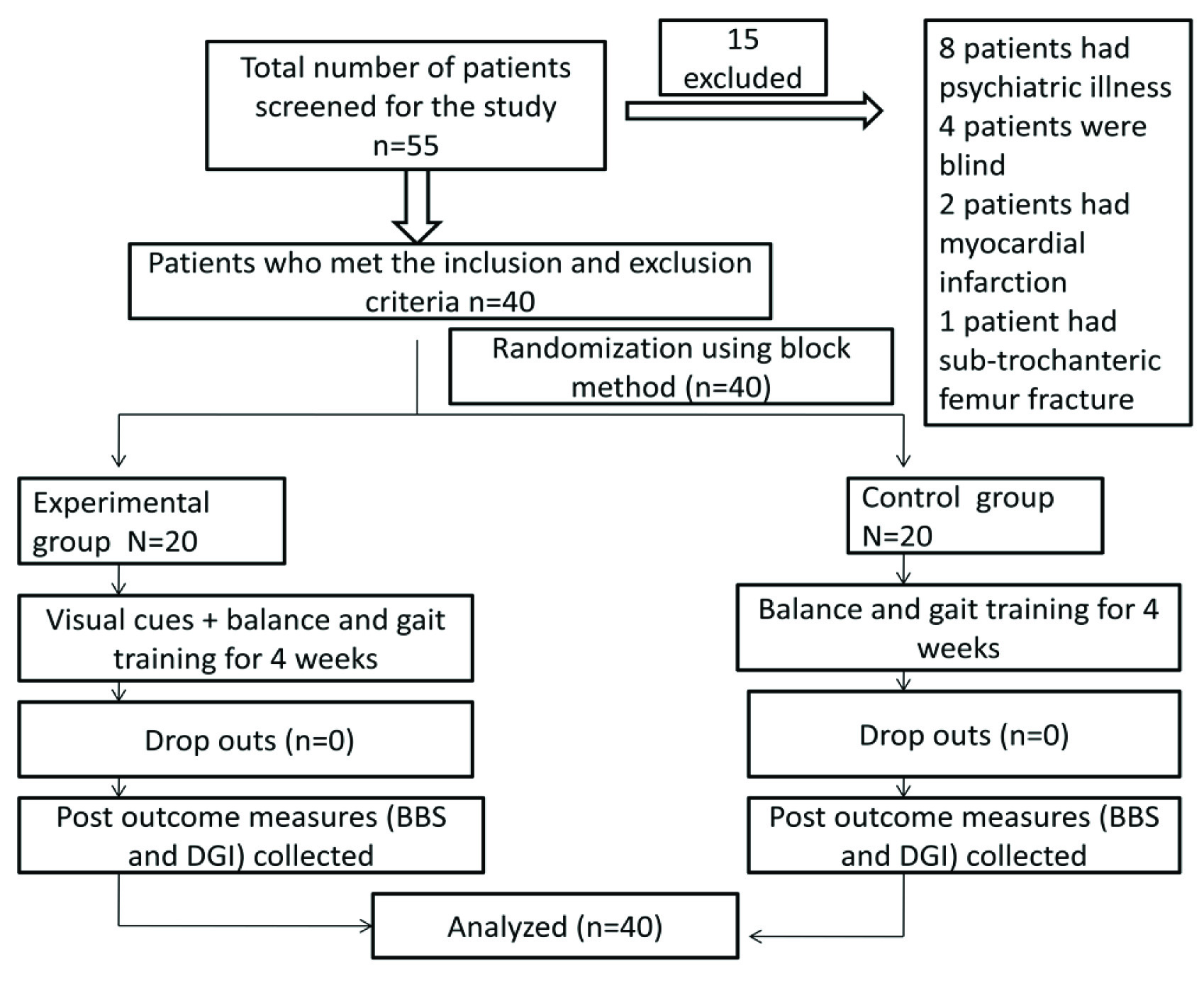
A 55 elderly subjects were screened for eligibility. A total of 40 patients who fulfilled the inclusion criteria requirements were enrolled in the study. The flow chart is shown in [Table/Fig-3]. There were no drop outs in the study. Demographics showed groups mean and standard deviations for age and frequency counts for gender of the recruited elderly subjects. The mean age in the experimental and control group is 68.35. The number of females was found to be more in both experimental and control group. The demographic data was analysed using independent t-test and chi-square test and no statistically significant differences were found between two groups [Table/Fig-4].
CONSORT (consolidated standards of reporting trials) diagram showing the flowchart of participants through each stage of the study.
BBS- Berg balance scale, DGI- Dynamic gait index
Demographic characteristics of the participants.
| Sr No | Characteristics | Intervention(n=20) n (%) | Control(n=20) n (%) | p-value |
|---|
| 1 | AgeMean (SD) | 68.35 (3.29) | 68.5 (3.67) | 0.89 (t) |
| 2 | Sex | Male | 9 (45) | 4 (20) | 0.176 (χ2) |
| Female | 11 (55) | 16 (80) |
χ2 - chi-square test, t- independent sample t-test, SD- Standard Deviation
A significant improvement has been observed in Berg balance and dynamic gait index scores in both experimental and control groups but more marked improvement has been observed in experimental group both within and between groups as shown in [Table/Fig-5,6 and 7].
Paired t-test used to compare within group difference of experimental group of BBS and DGI.
| Pairs | Outcome measure | N | Mean | (±) S.D | Pairedmeandifference | 95% CI for the the difference | t-value | p-value |
|---|
| Lower | Upper |
|---|
| Pair 1 | BBS after | 20 | 52.5 | 2.74 | 7.2 | 8.87 | 5.62 | 9.32 | <0.001* |
| BBS before | 45.3 | 3.26 |
| Pair 2 | DGI after | 20 | 19.70 | 2.15 | 2.9 | 3.85 | 2.04 | 6.82 | <0.001* |
| DGI before | 16.75 | 3.35 |
* p-value< 0.001
BBS- berg balance scale, DGI- dynamic gait index, CI- confidence interval
Paired t-test used to compare within group difference of control group for BBS and DGI
| Pairs | Outcome measure | N | Mean | (±) S.D | Pairedmean difference | 95% CI of the difference | t-value | p-value |
|---|
| Lower | Upper |
|---|
| Pair 1 | BBS after | 20 | 47.65 | 2.87 | 2.85 | 3.40 | 2.29 | 10.78 | <0.001* |
| BBS before | 44.80 | 2.72 |
| Pair 2 | DGI after | 20 | 17.95 | 2.76 | 0.75 | 1.08 | 0.41 | 4.68 | <0.001* |
| DGI before | 17.20 | 2.76 |
*- p-value< 0.001
BBS- berg balance scale, DGI- dynamic gait index, CI- confidence interval
Independent sample t-test used to compare between the group differences of experimental and control group.
| Difference(after–before) | Group | N | Mean | (±) SD | Meandifference | 95% CI of the difference | t-value | p-value |
|---|
| Lower | Upper |
|---|
| BBSDifference(after-before) | Experimental | 20 | 7.75 | 2.51 | 4.9 | 3.64 | 6.15 | 7.89 | <0.001* |
| Control | 20 | 2.85 | 1.18 |
| DGIDifference(after-before) | Experimental | 20 | 2.95 | 1.93 | 2.2 | 1.26 | 3.13 | 4.77 | <0.001* |
| Control | 20 | 0.75 | 0.71 |
*p-value< 0.001
BBS- Berg balance scale, DGI- Dynamic gait index, CI- confidence interval
Discussion
The results of the current study demonstrate that visual cueing techniques were effective in achieving augmented improvements in balance and gait in the elderly dwellers in community hence, we accept the experimental hypothesis. This present study braces the studies of Bank PJM et al., wherein suggestions were laid to utilize visual cueing techniques to achieve optimum gains in training gait in elderly [10]. The present study has incorporated the views of Devis Rl et al., who had recommended for the explicit need of describing cues that aid learning in geriatric community [17]. It was proposed that colourful visual cues facilitate learning in elderly but less is known about the type of cues that aid learning. An outline of the intensity, duration and type of cues that can facilitate learning in elderly subjects has been described in the present study.
The evidence on the practical applicability of biofeedback methods is constrained according to a systematic review reported by Zijlstra A et al., [9]. An exigency was expressed in the previous study to shift the focus on biofeedback methods that can be utilized in daily clinical setting which would enable elderly to practice tasks that are similar to the accustomed daily life challenges which would make transfer of training in real life situations more effective. Insufficient evidence on the use of biofeedback methods in older adults was reported because most studies did not report participation rates and frequency of dropouts. The present study thus, provides with a feasible robust method in training balance and gait in elderly population which can be conveniently utilized in clinical settings.
Previous on left side studies by Hatzitaki V has found visual cue guided weight shift training improved visuo motor processing while avoiding obstacles in the elderly population [18]. The results of the present study coincides with the erstwhile studies on visual cue training carried by Sihvonen SE [19], wherein it was found that berg balance scale scores and dynamic gait scores improved by 6.9% and 35.9% respectively in experimental group compared to 0.6% and 0.7% respectively in the control group. In the present study, the berg balance scale scores and dynamic gait index improved by mean and standard deviation of 7.75±2.51 and 2.95±1.93 respectively in the experimental group compared to mean and standard deviation of 2.85±1.18 and 0.75±0.71 in the control group.
The rationale for the significant improvement in balance and gait in the elderly in the experimental group could be attributed to the potential of visual cues in improving gaze behaviour. The innate gaze ability is often diminished in elderly who are at increased risk of falls which further results in inaccurate placement of foot. Elderly prefer to plan the forthcoming steps over the precise execution of ongoing steps which may result to trips and falls admist cluttered terrains. Visual cues, thus aid in seasoning effective and safe gaze behaviour in elderly subjects.
The auxiliary gains in balance and gait in elderly in the present study can be attributed to the utilization of group therapy method during training sessions. Group therapy fosters social interaction amongst the elderly flocks, provides motivation, deminutes boredom, and improves mental well being in the elderly population. Rubenstein LZ in his study had utilised group therapy method wherein gait training was progressed from five to 15 minutes for 12 weeks. The results showed an improvement in gait scores with paired mean difference of 1.3 when compared to present study which shows paired mean difference of 2.9. Hence, both the studies brace the use of group therapy sessions for gait training [20].
Peper CL had reported that guided ambulation by visual cues augmented participant’s attention towards task oriented information and it was farther more challenging compared to other cues. The rationale behind this was attributed to the indigenous reliance of gait on visual information [6]. Hence, the present study used visual cues to train balance and gait. Visual cue training stimulates the visual motor pathway and amelioration observed in activities of daily living following training sessions can be accredited to brains compensation and prevention strategies.
Limitation
Lack of long-term follow up of the elderly subjects. The history and number of falls were not scrutinized and documented in the present study. The current study was conducted in a single old age centre hence in future, double blinded multi-centred randomised control trials with long term follow up should be ventured in the elderly population to bridge the lacunae’s in the present study.
Conclusion
The present study concludes that visual cue training is capable of enhancing balance and gait among the broad segment of elderly veterans in the community. Visual cue training can also be utilized as a simple and feasible method in clinical settings to address sprouting public health issue of balance and gait disorders which is cohesively coupled with catastrophe of falls admist elderly residents in the community.
Abbreviations
BBS = Berg balance scale
DGI = Dynamic gait index
SPSS = Statistical package for the social sciences
S.D = Standard Deviation
CI = Confidence Interval
t = test significance
p = probability
M =Male
F =Female
χ2 - chi-square test, t- independent sample t-test, SD- Standard Deviation
* p-value< 0.001
BBS- berg balance scale, DGI- dynamic gait index, CI- confidence interval
*- p-value< 0.001
BBS- berg balance scale, DGI- dynamic gait index, CI- confidence interval
*p-value< 0.001
BBS- Berg balance scale, DGI- Dynamic gait index, CI- confidence interval
[1]. Dharmarajan TS, Ugalino JT, The aging processGeriatric Medicine 2000 1(1):2-3. [Google Scholar]
[2]. Forman DE, Berman AD, Cobe CH, PTCA in the elderly: The young-old versus the old-oldJ Am Geriatr Soc 1992 40(1):19-22. [Google Scholar]
[3]. Borah H, Shukla P, Elderly in India profile and programs February 2016 New DelhiCentral Statistics office [Google Scholar]
[4]. Nataliya S, Meg EM, Frances H, Effects of age on balance control during walkingArch Phys Med Rehabil 2004 85(4):582-88. [Google Scholar]
[5]. Sturnieks DL, George RSt, Lord SR, Balance disorders in elderlyClin Neurophysiol 2008 38(6):467-78. [Google Scholar]
[6]. Peper CL, Oorthuizen JK, Roerdink M, Attentional demands of cued walking in healthy young and elderly adultsGait Posture 2012 36(3):378-82. [Google Scholar]
[7]. Susan BOS, Thomas JS, Physical Rehabilitation 2007 5th edNew DelhiJaypee Brothers Medical Publishers [Google Scholar]
[8]. Eric A, Russell R, Peter A, Does visual feedback during walking result in similar improvements in trunk control for young and older healthy adultsJ Neuroeng Rehabil 2013 10:110 [Google Scholar]
[9]. Agnes Z, Martina M, Lorenzo C, Wiebren Z, Biofeedback for training balance and mobility tasks in older populations: a systematic reviewJ Neuroeng Rehabil 2010 7(58):1-15. [Google Scholar]
[10]. Paulina JMB, Melvyn R, Peper CE, Comparing the efficacy of metronome beats and stepping stones to adjust gait: steps to followExp Brain Res 2011 209:159-69. [Google Scholar]
[11]. Shumway CA, Baldwin M, Polissar NL, Gruber W, Predicting the probablity for falls in community dwelling older adultsPhys Ther 1997 77(8):812-19. [Google Scholar]
[12]. Daniella RBS, Robert CW, Johanna B, Kathleen O, Kyriakos M, David V, Mini-mental state exam domains predict falls in an elderly population: follow-up from the hispanic established populations for epidemiologic studies of the elderly (h-epese) studyEthn Dis 2010 20:48-52. [Google Scholar]
[13]. Divya RS, Mallikarjunaiah Maheshwari P, Effectiveness of a four weeks exercise program using elastic tubing as perturbation force on balance in elderly subjectsInt J Physioth Res 2013 (3):88-92. [Google Scholar]
[14]. Kristen LH, Trudy P, Andrew W, Diane W, Sue J, Catherine S, Visual cue training to improve walking and turning after stroke: a study protocol for a multi-centre, single blind randomised pilot trialTrials 2013 14:276 [Google Scholar]
[15]. Felicity AL, Shyle FH, Mackintosh Functional balance assessment of older community dwelling adultJ Allied Health 2007 5(4):5 [Google Scholar]
[16]. YiPo C, Stacy LF, Kathye EL, Craig AV, Use of item response analysis to investigate measurement properties and clinical validity of data for the dynamic gait indexPhys Ther 2006 86:778-87. [Google Scholar]
[17]. Devis RL, Therrien BA, Cue colour and familiarity in place learning for older adultsRes Gerontol Nurs 2012 5(2):138-48. [Google Scholar]
[18]. Hatzitaki V, Amiridis IG, Nikodelis T, Spiliopoulou S, Direction induced effects of visually guided weight shifting training on standing balance in the elderlyGerontology 2009 55(2):145-52. [Google Scholar]
[19]. Sihvonen S, Sipila S, Era P, Changes in postural balance in frail elderly women during a four week visual feedback training: a randomised controlled trialGerontology 2004 50(2):87-95. [Google Scholar]
[20]. Laurence ZR, Karen R, Josephson Peggy RT, Effects of a group exercise program on strength, mobility, and falls among fall-prone elderly menJ. Gerontol. A Biol Sci Med Sci 2000 55(6):317-21. [Google Scholar]