Application of C-Arm for Intra Operative Radiographic Support in Oral and Maxillofacial Surgical Procedures Under General Anaesthesia
L K Surej Kumar1, Mathew Tharakan2, Johna S Peranthodi3, Deepa S Divakaran4
1 Senior Consultant, Department of Oral and Maxillofacial Surgery, KIMS Hospital, Trivandrum, Kerala, India.
2 Consultant Orthodontist, Department of Oral and Maxillofacial Surgery, KIMS Hospital, Thrissur, Kerala, India.
3 Postgraduate Student, Department of Oral and Maxillofacial Surgery, KIMS Hospital, Trivandrum, Kerala, India.
4 Postgraduate Student, Department of Oral and Maxillofacial Surgery, KIMS Hospital, Trivandrum, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mathew Tharakan, Consultant Orthodontist, Department of Oral and Maxillofacial Surgery, Tharakans House, Big Bazzar Aranattukara, Thrissur-680618, Kerala, India.
E-mail: drcamt@gmail.com
C-arm fluoroscope, Maxillofacial region, Odontogenic implications
Dear Editor,
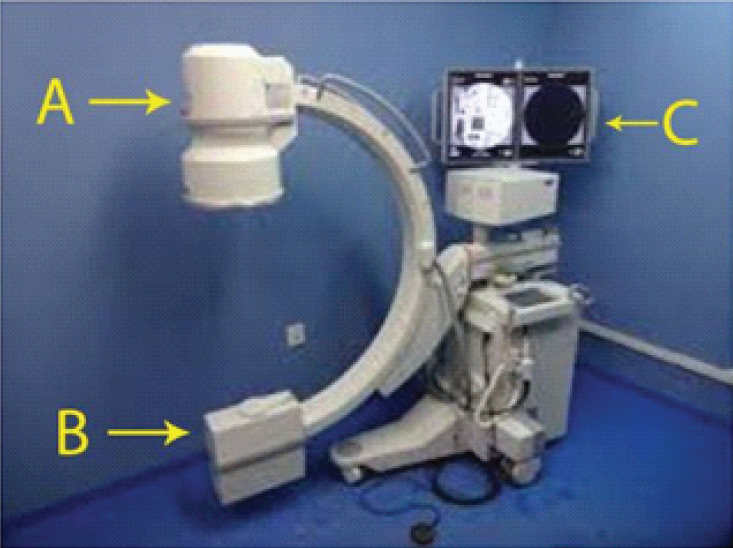
The scenario of a surgeon where he cannot confidently complete a general anaesthetic procedure, due to some missing finer details is pathetic. Oral and Maxillofacial surgeons often come across such situations as most of the intraoral surgical procedures are attempted through limited access incisions because of the close proximity of multiple vital structures in that region [1]. A radiographic support is a saviour in such situations. But conventional radiographs for the maxillofacial region are not feasible in the operating room due to difficulties in the patient positioning, processing delays and aseptic protocols. The C-arm fluoroscope, which is an integral part of most of the modern day operating rooms, can be effectively utilized for intraoperative radiographic support in the Oral Maxillofacial region. C-arm is an innovative imaging device which uses a two dimensional radiograph to acquire radiographic images in real time, making it easier for physicians to monitor progress. This device which is in the form of a half-moon applies stereotaxic method put forward by Ariyan S for removing foreign bodies from the extremities [2,3] [Table/fig-1]. They are primarily used during surgical and orthopaedic procedures. This C-arm device based on X-ray technology could be used flexibly in confined spaces. The C-shaped arm is used to connect X-ray source and X-ray detector to one another therefore, it is known as a C-arm. Since the radiation source and the sensor could be moved without disturbing the patient’s position on the operating table [Table/Fig-2,3], with minor adjustments in the patient’s head position, quality images of the maxillofacial region could be captured on the monitor. C-arm systems offer both spot and fluoroscopic imaging modes which allows the generation of continuous real time moving images [4].
C-Arm Machine, G.E Electronics, Flurostar 7900 series (Power – 2.2 kW, Resolution 1k x 1k, II format: 9" or 23 cm).
A: X-ray source, B: X-ray detector, C: Monitor
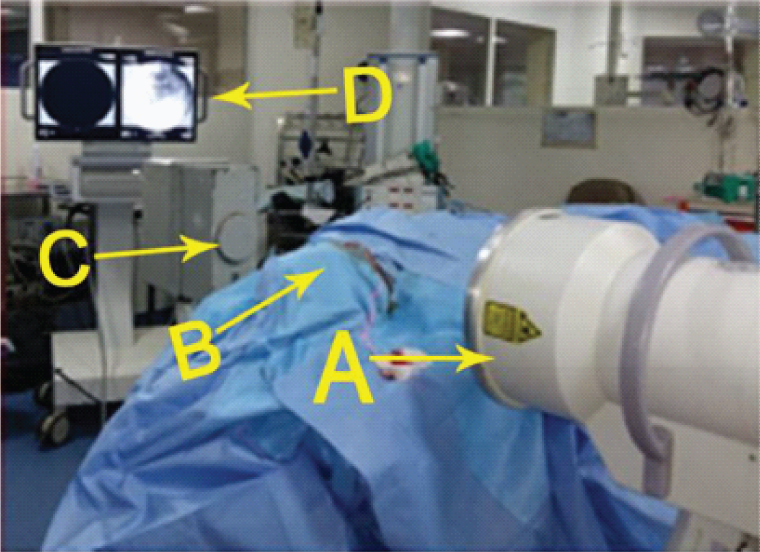
Positioning of C-arm with patient on operating table.

C-arm setup with real time image on the monitor; A: X-ray source, B: Patient on operating table, C: X-ray detector, D: Monitor with Image.
Though the radiation dose of C-arm (36.3-39 micro Sv) is more compared to other common radiographic techniques such as Intraoral periapical radiographs, orthopantomogram and other conventional radiographs (4.9-14.9 micro Sv) it is far less than that of computed tomography which is considered as the gold standard of all radiographic techniques [5]. We have found that under circumstances where a radiographic support becomes mandatory during a maxillofacial surgical procedure under general anaesthesia, like accidental displacement of metallic or other radiographically detectable fragments into the surrounding tissue spaces, checking for doubtful remnants and final detailing in areas of poor access, where the conventional techniques are practically inconvenient, the C-arm could be effectively utilized [6]. Though the C-arm imaging has few disadvantages like pausing the surgical procedure, lead shield for the operator and slightly increased radiation than the conventional radiographs, its timely utilization to avoid intraoperative dilemmas and possible post-operative complications nullifies the minor disadvantages.
Conclusion
Though the C-arm is an integral component in an operating room, its implications in the oral and maxillofacial region is currently overlooked. Apt utilization of this equipment in the oral and maxillofacial region allows the surgeon to complete the procedure with confidence.
[1]. Chen X, Xu L, Sun Y, Politis C, A review of computer-aided oral and maxillofacial surgery: planning, simulation and navigationExpert Rev Med Devices 2016 Nov 1 13(11):1043-51. [Google Scholar]
[2]. Nezafati S, Shahi S, Removal of broken dental needle using mobile digital C-armJ Oral Sci 2008 50(3):351-3. [Google Scholar]
[3]. Ariyan S, A simple stereotactic method to isolate and remove foreign bodiesArch Surg 1977 112(7):857-9. [Google Scholar]
[4]. Bott OJ, Dresing K, Wagner M, Raab BW, Teistler M, Informatics in radiology: use of a C-arm fluoroscopy simulator to support training in intraoperative radiographyRadiographics 2011 31(3):E65-75. [Google Scholar]
[5]. Kim AN, Chang YJ, Cheon BK, Kim JH, How effective are radiation reducing gloves in C-arm fluoroscopy-guided pain interventions?Korean J Pain 2014 27(2):145-51. [Google Scholar]
[6]. Mohan AP, Bindra S, Dendukuri G, An unusual approach to retrieve right mandibular canine tooth, displaced into submandibular space following fracture mandible, using c-armJ Maxillofac Oral Surg 2010 9(1):78-9. [Google Scholar]