Mechanical and Adhesive Retention for Bilateral Ear Prosthesis
Mayara De Freitas Paiva1, Célia Regina Moreira Lanza2, Marcelo Coelho Goiato3, Maria Fernanda Lopes Fonseca4, Amália Moreno5
1 Dentist, Private Dental Clinic, Belo Horizonte, Brazil.
2 Professor, Department of Oral Surgery, Pathology and Dental Clinical, School of Dentistry, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, Minas Gerais, Brazil.
3 Professor, Department of Dental Materials and Prosthodontics, Aracatuba Dental School, Sao Paulo State University (UNESP), Aracatuba, Sao Paulo, Brazil.
4 Graduate Student, Department of Oral Surgery, Pathology and Dental Clinical, School of Dentistry, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, Minas Gerais, Brazil.
5 Professor, Department of Oral Surgery, Pathology and Dental Clinical, School of Dentistry, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, Minas Gerais, Brazil.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amália Moreno, Professor, Department of Oral Surgery, Pathology and Dental Clinical, School of Dentistry, Universidade Federal De Minas Gerais (UFMG), Belo Horizonte-31.270-010, Minas Gerais, Brazil.
E-mail: amalia_moreno@yahoo.com.br
Ear auricle, Maxillofacial prosthesis, Prosthesis retention, Rehabilitation
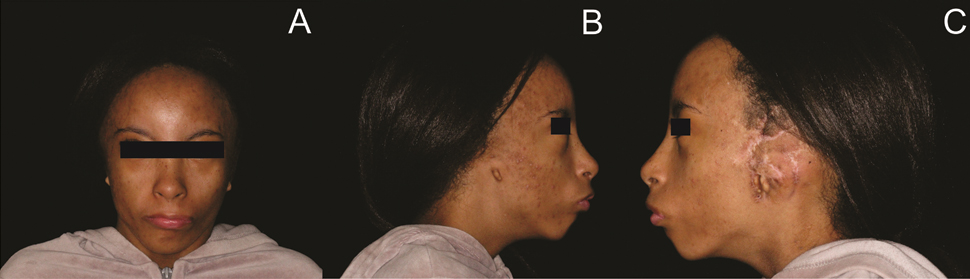
A 12-year-old female patient sought facial rehabilitation at the Maxillofacial Prosthesis Clinic of the School of Dentistry. During physical examination, absence of the outer ear was observed on both sides of the face, but with the presence of a tragus [Table/Fig-1]. The consent was obtained from the patients parents.
View of the patient without an outer ear on both sides of the face: (A) front; (B) right profile; and (C) left profile.
The steps involved in the fabrication of the ear prosthesis were: (a) a facial impression was made with the patient in a supine position. Once the impression had been checked, it was poured into dental stone; (b) To obtain wax patterns, indirect modeling was performed through the prior modeling of the auricular area of a classmate with the same biotype [1]; (c) Once four wax patterns had been created [Table/Fig-2], they were adapted and recontoured to the defect on the patient’s plaster models; (d) A clinical aesthetic trial was performed on the patient which verifies the functional soft tissue mobility to prevent gapping and allows a more intimate prosthetic fit in the condylar area [1]; (e) The wax patterns were included in manufacturing plaster muffle to eliminate wax and obtain the ear impression; and (f) The facial silicone elastomer (A-2000, Factor II Inc., USA) was inserted into this impression, including intrinsic coloration. Extrinsic coloration was performed on the installation [2].
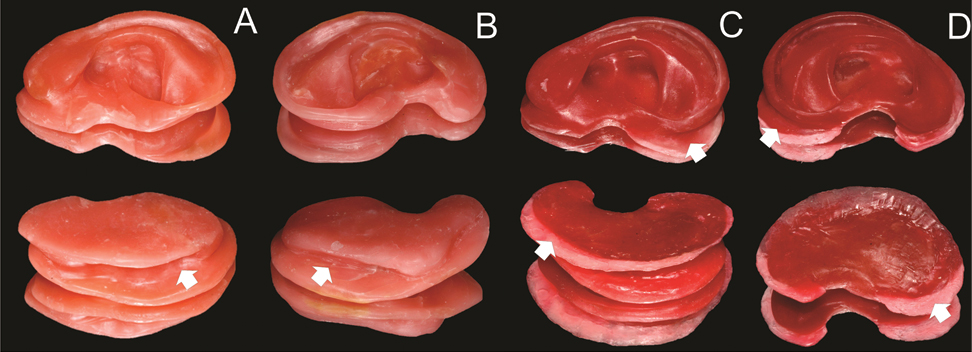
Wax modeling and sculpting of the patterns obtained by indirect modeling: (A) for the right side through mechanical retention; (B) for the left side through mechanical retention; (C) for the right side through adhesive retention; and (D) for the left side through adhesive retention.
The arrows in (A/B) indicate the space left in the wax patterns for mechanical retention placement. The (C/D) arrows indicate the extension provided in the wax patterns to facilitate placement of the adhesive and allow the best contact with the remaining tissue.
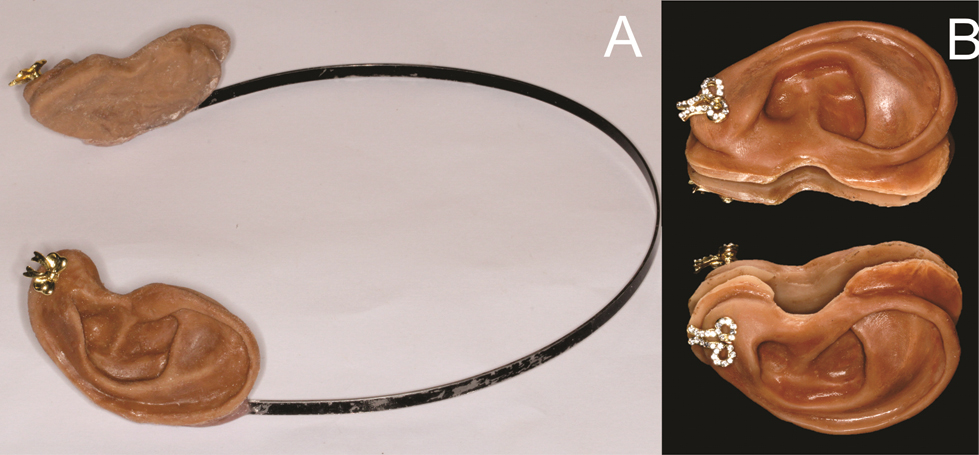
Facial acrylic resin (Rapidaflex, Artigos Odontológicos Clássico Ltda., SP, Brazil) was added to the pair of ear prosthesis geared towards mechanical retention in a space that had been left in the posterior portion of the silicone prosthesis. Adhesive retention was obtained by attaching the facial prosthesis using a specific adhesive substance (Pros Aide, Factor II Inc., USA) [Table/Fig-3,4]. After the prosthesis had been installed, the patient was taught how to use it properly and instructed to remove the prosthesis when sleeping and clean the mutilated area with a gauze and cotton swab soaked in saline solution. The use 0.12% chlorhexidine digluconate was recommended once a month to disinfect the ear prosthesis [3].
Pairs of finalized ear prosthesis.
Views of the patient with installed ear prosthesis: (A) frontal view with a pair of ear prostheses through mechanical retention, (B) right profile – adhesive retention, and (C) left profile – adhesive retention.

The goal of facial prosthesis is to reconstruct losses of facial structures, return aesthetics, and protect remaining tissues [1]. These prosthesis are intended for patients with congenital defects or mutilating traumatic injuries in the head and neck [1,4]. In cases of agenesis of this organ, modeling can represent a challenge, since the maxillofacial prosthetist does not have a prior reference.
It is well known that the wax pattern, through indirect modeling, is obtained by modeling a close relative who presents as similar a biotype as possible to the patient [1]. Indirect modeling was applied as an artistic and prosthetic resource to obtain the model of the outer ear. What could be observed were the advantage of the applied modeling technique, the ease of adapting the wax to the remaining tissue and most importantly, the time saved in the piece’s sculpting and wax modeling before obtaining the processed mould.
The retention of the ear prosthesis can be mechanical by means of eyeglass frames however, hair bands can also be used [4]. Moreover, there is adhesive retention or osseointegrated implants [1,4]. Previous studies have reported a wide range of techniques and retention for the manufacture of facial prosthesis [1,4]. In some cases, anatomical retention can be achieved on the outer ear itself, which was impossible in this case. One of the pairs of prosthesis used in the present case was mechanically attached to a hair band with specific self-polymerized facial acrylic resin, keeping the prosthesis in an anatomical position. The hair band proved to be an effective restraint system, providing an excellent fit on the remaining facial portion of the outer ear, with no complaints of tissue compression or recurrent destruction [4] of the prosthesis when the patient was in motion. The patient reported that mechanical retention was effective when used in situations with continuous movement including low impact activities. Contrariwise, the adhesive retention offered greater stability of the prosthesis, allowing sudden movement.
When installing the ear prosthesis, one could see that the extrinsic coloration of the outer ear allowed for the mimicking of the color of the adjacent skin [2]. The option of making two pairs of auricular prosthesis with different retention systems alternatively allows a choice for the best daily situation. In addition, opting for the mechanically retained auricular prosthesis lets the remaining tissue rest in relation to intense use of adhesive. Some limitations regarding mechanical or adhesive retentions include the possibility of total displacement of the prosthesis, resulting in embarrassment. The patient and her family reported satisfaction with the result obtained and the two year follow up has been successful.
[1]. Mantra SS, Thombre RU, Prosthetic rehabilitation of a patient with bilateral auricular deformityJ Adv Prosthodont 2011 3:101-05. [Google Scholar]
[2]. Kiat-amnuay S, Beerbower M, Powers JM, Paravina RD, Influence of pigments and opacifiers on color stability of silicone maxillofacial elastomerJ Dent 2009 37:45-50. [Google Scholar]
[3]. Goiato MC, Zucolotti BC, Mancuso DN, dos Santos DM, Pellizzer EP, Verri FR, Care and cleaning of maxillofacial prosthesesJ Craniofac Surg 2010 21:1270-73. [Google Scholar]
[4]. Kumar P, Shubha J, Sowjanya P, Shalini BN, Jesudass G, An silicone auricular prosthesis along with retentive AIDS-a case reportJ Clin Diagn Res 2014 8:ZD18-ZD19. [Google Scholar]