The Effect of Chamomile Flower Essence on Pain Severity after Elective Caesarean Section under Spinal Anaesthesia: A Randomized Clinical Trial
Bahareh Najafi1, Faraz Mojab2, Loghman Ghaderi3, Fariba Farhadifar4, Daem Roshani5, Jamal Seidi6
1 MSc. in Nursing, Besat Hospital, Kurdistan University of Medical Sciences, Sanandaj, Iran.
2 Full Professor, Pharmaceutical Sciences Research Centre (PSRC), Shahid Beheshti University of Medical Sciences, Tehran, Iran.
3 General Surgeon, Besat Hospital, Kurdistan University of Medical Sciences, Sanandaj, Iran.
4 Full Professor, Department of Obstetrics and Gynaecology, Kurdistan University of Medical Sciences, Sanandaj, Iran.
5 Associate Professor, Social Determinants of Health Care Center, Kurdistan University of Medical Sciences, Sanandaj, Iran.
6 Assistant Professor, Clinical Care Research Centre, Kurdistan University of Medical Sciences, Sanandaj, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jamal Seidi, Pasdaran St., Sanandaj, Kurdistan, Iran.
E-mail: jamal.seidi@muk.ac.ir
Introduction
Nowadays, herbal essence and aromatherapy are used as a form of complementary medicine and non-pharmacological interventions alongside modern medicine and pharmacological interventions.
Aim
To evaluate the effect of chamomile flower essence on pain severity following elective caesarean section under spinal anaesthesia.
Materials and Methods
This single-blind randomized clinical trial was conducted on 80 women referred to Besat hospital in Sanandaj, Iran in 2016. In total 80 patients who were candidates for elective caesarean section were selected for this study. Following caesarean section, patients were randomly divided into intervention and control groups. For patients in intervention group inhalation of two drops of chamomile flower essence was used. For patients in control group two drops of normal saline was used as placebo. All patients received a 100 mg sodium diclofenac rectal suppository in the recovery room. In case of pain six hours post caesarean section, intervention was performed. Pain intensity was measured by the Visual Analog Scale. Data were analysed using SPSS statistical software version 20. Independent t-test and chi-square test were also used.
Results
Pain intensity in the intervention group was significantly lower than the control group (p <0.001). The need for analgesics was also significantly lower in the intervention group than the control group (p <0.001).
Conclusion
The results of this study showed that the use of chamomile flower essence following caesarean section reduced pain and also the need for analgesics. Therefore, the use of aromatherapy alongside drug therapy to reduce pain is recommended.
Aromatherapy, Essential oils, Surgery
Introduction
The prevalence of caesarean section has increased globally, such that 20-25% of pregnant women give birth by caesarean section [1]. Cesarean section rate in Iran has been reported around 60% [2]. Prolonged pain after caesarean section unintentionally leads to increased duration of hospital stay and increased costs [3,4]. Faster pain relief following caesarean section would result in quicker breastfeeding of the baby, getting out of bed early, preventing atelectasis, prevention of deep vein thrombosis and early return of bowel function among others [5].
Postoperative pain management is a common problem following caesarean section. There are many interventions to reduce the pain that can be medicinal or non-medicinal [6]. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as sodium diclofenac are used for postoperative pain control particularly for caesarean section [7]. Because of various complications associated with the use of narcotic drugs such as respiratory depression, addiction, hypnotic effects and production of toxic metabolic by-products, the use of non-narcotic drugs are preferred [8].
Aromatherapy as a safe intervention alongside drug therapy is an option for reducing the consumption of analgesics [9]. In aromatherapy herbal essence are used, which are free of animal products, affordable, have no serious side effects and non-invasive. Also, they have no drug interactions, their performance is simple, and they are better accepted by patients; therefore aromatherapy is a good supplement for the treatment of postoperative pain [10]. Aromatherapy is one of the independent nursing interventions that can be used clinically as a complement to modern care [10].
Aromatherapy products like fumes and spray are spread in the air; these particles are inhaled and absorbed into the body [11]. With the advancement in technology, herbal essence extraction is easier than other forms of medicinal herbs [12]. The effectiveness of aromatherapy in some cases is more than other forms of medicinal herbs and inhalation of essential oils has given rise to olfactory aromatherapy [13]. Stea S et al., reported the effectiveness of inhalation of essential oils on pain after surgery [14]. One of the essential oil which is widely used in aromatherapy is chamomile flower essence [15,16]. Chamomile essential oil is obtained by steam distillation [16]. Chamomile has anti-inflammatory, antibacterial and anti-fungal effect and topically used for treating skin inflammation, hemorrhoids, ulcers of the leg, and cracked nipples. It also has an effective role in reducing the pain and repairing damaged tissues [17]. In literature, it has been used mostly as decoctions, ointments, and in other pharmaceutical forms [16]. Chamomile has rarely been used as an essence. The use of chamomile essential oil in phase I clinical trial was found to be safe in mice [18].
After caesarean section, reducing pain and preventing pain related complications are important. It should be considered as one of the most important duties of nurses to reduce consumption of chemical drugs to relieve pain [10]. Hence, this study was conducted to evaluate the effect of chamomile flower essence on pain severity following elective caesarean section under spinal anaesthesia.
Materials and Methods
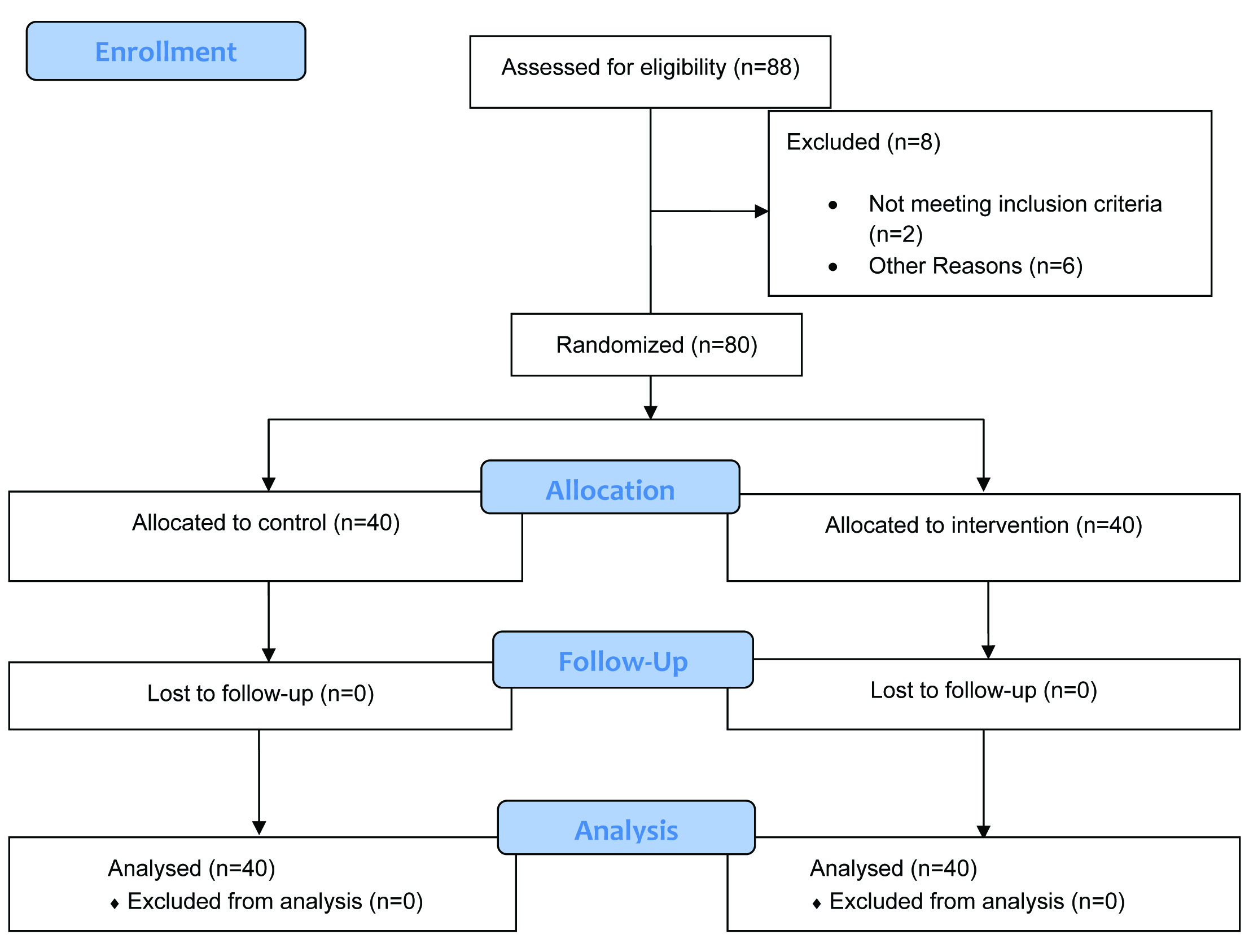
This single-blind randomized clinical trial was conducted on 80 women referred to Besat hospital in Sanandaj, Iran from August 2016 till the end of December 2016. Total of 88 patients who were candidates for elective caesarean section were selected for this study. Considering Type I error as 5% and Type II error as 20% and the average difference between the two methods in previous literature (20%) [17], the sample size was calculated as 40 patients in each group.
From 88 patients, two patients were excluded due to complications of spinal anaesthesia and therefore did not meet the inclusion criteria. Also, two other patients were excluded as the infant was critically ill, one more patient was excluded because of haemodynamic changes, another because of excessive bleeding and finally another two patients because of transfer to ward after delivery. Total of 80 patients using simple randomization were randomly allocated to intervention and control groups and evaluated [Table/Fig-1].
Flow diagram of the progress through the phases of the trial.
Inclusion criteria included candidates for elective caesarean section, who volunteered to participate in the study and to use spinal anaesthesia technique, no history of drug abuse and analgesic consumption. Exclusion criteria included patients with underlying diseases and patient unwilling to participate in the study.
Chamomile flower was purchased from Zardband Pharmaceuticals Co. After confirming its scientific name essential oil was extracted by distillation method, and diluted to 5% in base oil (sesame). All stages of preparing and diluting the essential oil were carried out in the Faculty of Pharmacy, Shahid Beheshti University of Medical Sciences, Tehran, Iran. As reported in literature, essential oils are diluted in vegetable oils [13], therefore in our study sesame oil was used. Sesame oil does not have any confounding effect on chamomile essential oil [19].
Spinal anaesthesia was performed for all patients with the same combination of drugs as described. Before anaesthesia all patients received half or one liter ringer lactate. Then, in a sitting position, using Quincke needle No. 25, through the third and fourth lumbar inter-vertebral space 2 to 3 mL, 5% bupivacaine was injected into the subarachnoid space. The patients were placed in supine position and monitored during anaesthesia.
All patients received 100 mg sodium diclofenac rectal suppository in the recovery room. Six hours after caesarean section in case of pain more than three based on Visual Analog Scale (VAS) the intervention was performed. For patients in intervention group inhalation of two drops of chamomile flower essence was used (Two drops of chamomile essential oil was shed on a cotton ball). For patients in control group two drops of normal saline was used as placebo (Two drops of normal saline was shed on a cotton ball). Patients were asked to inhale the cotton ball. Pain was recorded immediately after the first deep inhalation and exhalation. After fifteen minutes, pain was recorded again. The average of both the readings was taken. If pain continued (more than three based on visual analog scale) in each group after the intervention the patients were prescribed analgesic medication as ordered by physician. This study was single blind and patients were unaware whether receiving placebo or essential oil.
This study was approved by the Ethics Committee of Kurdistan University of Medical Sciences (IR.MUK.REC.94/122) and was also has been registered in Iranian Registry for Clinical Trials (IRCT2016081726861N2). Written consent was taken from the participants before the study.
Statistical Analysis
Data including demographic characteristics and intensity of pain were recorded in a check list. Data were analysed using SPSS statistical software version 20. Independent t-test and chi-square test were used. The level of significance was considered as 0.05.
Results
The results of this study showed that there were no significant differences between the two groups in terms of age, weight, haemodynamic status including: blood pressure, pulse rate, temperature and Peripheral Oxygen Saturation (SpO2) [Table/Fig-2].
Frequency distribution of variables and demographic characteristics in the two groups.
| Variables | Groups | Mean±SD | p-value* |
|---|
| Age (Years) | Intervention | 30.63±4.61 | 0.564 |
| Control | 31.53±5.42 |
| Weight (Kg) | Intervention | 70.28±4.22 | 0.480 |
| Control | 71.44±3.66 |
| Systolic blood pressure (mm/Hg) | Intervention | 105±11.5 | 0.462 |
| Control | 107±12.6 |
| Pulse rate | Intervention | 80±12 | 0.526 |
| Control | 78±14 |
| Temperature (Celsius) | Intervention | 36.8±0.8 | 0.426 |
| Control | 36.6±0.8 |
| Peripheral Oxygen Saturation (SpO2) (Percent) | Intervention | 94±4 | 0.372 |
| Control | 92±6 |
*Independent samples-T test
Comparing mean pain intensity before intervention showed no statistically significant difference between the two groups, but after the intervention pain intensity in the intervention group was significantly lower than the control group (p=0.001) [Table/Fig-3].
Comparing the mean pain intensity in the two groups.
| Pain Intensity | Groups | Mean | SD | p-value* |
|---|
| Before Intervention | Chamomile | 6.54 | 2.12 | 0.210 |
| Placebo | 6.10 | 1.98 |
| After Intervention | Chamomile | 4.10 | 1.68 | 0.001* |
| Placebo | 5.77 | 1.94 |
*Independent sample T-test
The need for analgesics was also lower in the intervention group than the control group significantly (p=0.001). [Table/Fig-4].
Comparison of frequency of analgesic consumption after intervention in the two groups.
| Groups | Analgesic consumption | No analgesic consumption | Total | p-value* |
|---|
| Number (%) | Number (%) | No.(%) |
|---|
| Chamomile Group | 21 (52.5) | 19 (47.5) | 40 (100) | 0.001 |
| Placebo Group | 36 (90) | 4 (10) | 40 (100) |
*chi square, df=2
Discussion
Chamomile flower belongs to Asteraceae family. The main components of chamomile are: alpha bisabolol, bisabolol oxide, kamazolen, and flavonoid [20]. Pharmacological and analgesic mechanism of chamomile is related to kamazolen [13].
The results of the present study showed that after intervention, pain intensity in the group that received chamomile essential oil (intervention group) was significantly less than placebo group (control group). In a study by Aradmehr H et al., the effect of chamomile cream on pain after episiotomy in primiparous women was evaluated. They confirmed the analgesic and anti-inflammatory effect of chamomile and concluded that chamomile cream reduced pain after episiotomy in primiparous women [17]. Sharifi F et al., found that consumption of chamomile extract was more effective than Mefenamic Acid in relieving the intensity of premenstrual syndrome associated symptomatic psychological pain [16]. Zargaran A et al., showed that topical application of chamomile oil as an analgesic was effective in reducing migraine headaches [21]. Lim EJ and Lee KY showed that inhalation aromatherapy for ten minutes after tonsillectomy with a mixture of Lavender and Chamomile oil reduced pain [22].
The results of our study also showed that the need for analgesics in the group that received chamomile essential oil (intervention group) was less than placebo group (control group). Therefore, the use of chamomile essential oil as a supplemental intervention alongside drug treatment can reduce the consumption of chemical analgesics. All patients in both intervention and control groups received sodium diclofenac suppositories before the intervention. But after intervention sodium diclofenac intake in the group that received chamomile essential oil (intervention group) was significantly less than placebo group (control group). Sharifi F et al., also showed that chamomile could reduce the need for analgesics [16]. Boehm K et al., in a study concluded that the use of diluted essential oils has minimal risks and could reduce the need for analgesics [23].
In previous studies chamomile essential oil has been used less for clinical care. Despite anti-inflammatory, analgesic and anti-anxiety effects of chamomile using it in the form of incense and ointment is not a conventional method, particularly for critically ill patients or after surgery. Use of these forms is more traditional. One advantage of this study as compared with previous studies was the use of chamomile essential oil instead of other forms. Moreover, its inhalation was very comfortable for patients. It can also be used as incense by nebulizer. Another difference between the present study and previous studies was that chamomile essential oil was used alone and separately from other non-pharmaceutical interventions. In some studies aromatherapy was used with other non-pharmacological interventions [24].
Limitation
The inhalation method of chamomile essential oil was a major limitation of this study. Two drops of chamomile essential oil was shed on a cotton ball and patients were asked to inhale the cotton ball. During this time, significant amount of essential oil could have evaporate or not enter the airways effectively. Another limitation was administration of a single dose due to short time of hospitalization and limited time of the study. Future studies to compare aromatherapy with other non-pharmacological analgesic interventions such as hypnotic therapeutic, relaxation, music therapy, acupressure, acupuncture, etc., is recommended.
Conclusion
In conclusion the results of this study showed that the use of chamomile flower essence following caesarean section reduced the pain and also the need for analgesics, therefore aromatherapy by inhalation of chamomile essential oil can be used as a safe and secure method as complementary medicine alongside medical and nursing interventions. Using the results of this study to develop further studies in the field of aromatherapy and preparing clinical guidelines is recommended.
*Independent samples-T test
*Independent sample T-test
*chi square, df=2
[1]. Seidy J, Farhadifar F, Ghadami N, Zandvakili F, Roshani D, Taifoori L, Effect of supplemental oxygen on the incidence and severity of nausea and vomiting in the patients after cesarean surgery under spinal anaesthesiaScientific Journal of Kurdistan University of Medical Sciences 2010 15(2):26-35. [Google Scholar]
[2]. Jouhari S, Bayati S, Poor Asadi Kheirabadi F, Moradi E, Cesarean section rate and its cause in fasa in the year 2011Journal of Fasa University of Medical Sciences 2014 4(3):295-300. [Google Scholar]
[3]. Sarin A, Litonius E, Naidu R, Yost C, Varma M, Chen L, Successful implementation of an enhanced recovery after surgery program shortens length of stay and improves postoperative pain, and bowel and bladder function after colorectal surgeryBMC Anaesthesiology 2016 16(1):55 [Google Scholar]
[4]. Suresh M, Preston RL, Fernando RC, LaToya Mason M, Shnider and Levinson’s anaesthesia for obstetrics 2012 Lippincott Williams & Wilkins [Google Scholar]
[5]. Darvish H, Memar Ardestani B, Mohammadkhani Shali S, Tajik A, Analgesic efficacy of diclofenac and paracetamol vs. meperidine in cesarean sectionAnaesthesiology and Pain Medicine 2014 4(1):e9997 [Google Scholar]
[6]. Vadivelu N, Kai AM, Kodumudi V, Berger JM, Challenges of pain control and the role of the ambulatory pain specialist in the outpatient surgery settingJournal of Pain Research 2016 9:425-35. [Google Scholar]
[7]. Bozkurt N, Kurdoglu M, Kurdoglu Z, Kutlusoy F, Biberoglu K, Postoperative pain control after cesarean section: Can diclofenac sodium be used instead of meperidine?J Matern Fetal Neonatal Med 2009 22(12):1144-50. [Google Scholar]
[8]. Olateju SO, Adenekan AT, Olufolabi AJ, Owojuyigbe AM, Adetoye AO, Ajenifuja KO, Pentazocine versus pentazocine with rectal diclofenac for postoperative pain relief after cesarean section: A double blind randomized placebo controlled trial in a low resource areaMiddle East Journal of Anaesthesiology 2016 23(4):443-48. [Google Scholar]
[9]. Singh P, Chaturvedi A, Complementary and alternative medicine in cancer pain management: A systematic reviewIndian Journal of Palliative Care 2015 21(1):105 [Google Scholar]
[10]. Johnson JR, Rivard RL, Griffin KH, Kolste AK, Joswiak D, Kinney ME, The effectiveness of nurse-delivered aromatherapy in an acute care settingComplementary Therapies in Medicine 2016 25:164-69. [Google Scholar]
[11]. Ueki S, Matsunaka E, Swa T, Ohashi K, Makimoto K, Effectiveness of inhalation of aromatherapy in reducing anxiety in patients before colonoscopy: a systematic review protocolJBI Database of Systematic Reviews and Implementation Reports 2015 13(9):40-50. [Google Scholar]
[12]. Cagliero C, Bicchi C, Cordero C, Liberto E, Rubiolo P, Sgorbini B, Analysis of essential oils and fragrances with a new generation of highly inert gas chromatographic columns coated with ionic liquidsJ Chromatogr A 2017 1495:64-75. [Google Scholar]
[13]. Ali B, Al-Wabel N, Shams S, Ahamad A, Khan S, Anwar F, Essential oils used in aromatherapy: A systemic reviewAsian Pacific Journal of Tropical Biomedicine 2015 5(8):601-11. [Google Scholar]
[14]. Stea S, Beraudi A, De Pasquale D, Essential oils for complementary treatment of surgical patients: state of the artEvidence-Based Complementary and Alternative Medicine 2014 2014:01-06. [Google Scholar]
[15]. Agatonovic-Kustrin S, Babazadeh Ortakand D, Morton DW, Yusof AP, Rapid evaluation and comparison of natural products and antioxidant activity in calendula, feverfew, and German chamomile extractsJ Chromatography A 2005 1385:103-10. [Google Scholar]
[16]. Sharifi F, Simbar M, Mojab F, Majd HA, Comparison of the effects of Matricaria chamomilla (Chamomile) extract and mefenamic acid on the intensity of premenstrual syndromeComplementary Therapies in Clinical Practice 2014 20(1):81-88. [Google Scholar]
[17]. Aradmehr M, Azhari S, Ahmadi S, Azmoude E, The effect of chamomile cream on episiotomy pain in primiparous women: A randomized clinical trialJournal of Caring Sciences 2017 6(1):19-28. [Google Scholar]
[18]. Can OD, Demir Ozkay U, Kiyan HT, Demirci B, Psychopharmacological profile of Chamomile (Matricaria recutita L.) essential oil in micePhytomedicine: International Journal of Phytotherapy and Phytopharmacology 2012 19(3-4):306-10. [Google Scholar]
[19]. Makedou KG, Iliadis S, Gogou M, Kara E, Papageorgiou G, Sesame oil: An ex vivo study of properties against oxidation of plasma low-density lipoproteins and total serum lipoproteinsHellenic Journal of Cardiology 2017 58(2):153-55. [Google Scholar]
[20]. Singh O, Khanam Z, Misra N, Srivastava M, Chamomile (Matricaria chamomilla L.): An overviewPharmacognosy Reviews 2011 5(9):82 [Google Scholar]
[21]. Zargaran A, Borhani-Haghighi A, Faridi P, Daneshamouz S, Kordafshari G, Mohagheghzadeh A, Potential effect and mechanism of action of topical chamomile (Matricaria chammomila L.) oil on migraine headache: A medical hypothesisMedical Hypotheses 2014 83(5):566-69. [Google Scholar]
[22]. Lim EJ, Lee KY, Effects of aroma inhalation therapy on pain in patients following a tonsillectomyJournal of Korean Academy of Fundamentals (KAFN) 2011 18(1):63-70. [Google Scholar]
[23]. Boehm K, Bussing A, Ostermann T, Aromatherapy as an adjuvant treatment in cancer care: A descriptive systematic reviewAfrican Journal of Traditional, Complementary, and Alternative Medicines/African Networks on Ethnomedicines 2012 9(4):503-18. [Google Scholar]
[24]. Ebrahimi Houshyar A, Hosein Rezaie H, Jahani Y, Kazemi M, Monfared S, Comparison of two methods of aromatherapy with lavender essence and Transcutaneous Electrical Nerve Stimulation (TENS) on cesarean postoperative painThe Iranian Journal of Obstetrics, Gynecology and Infertility 2015 18(146):06-12. [Google Scholar]