Atrophic Rhinitis (AR) is a nasal pathology characterised by nasal mucosal atrophy and the atrophy of the underlying bones [1]. This is characterised by the formation of abnormally roomy nasal cavities, anosmia, foul smelling greenish crusts, epistaxis and occasionally maggot infestation of the nose [2]. This condition can be primary or secondary. The cause of primary atrophic rhinitis is not known while the secondary form is caused by an underlying disease such as tuberculosis, leprosy, syphilis affecting the nose. It is seen more commonly in tropical countries with women being more prone than men (5.6:1) [2] Also, it is more likely to affect young and middle aged adults. Various theories have been proposed for the aetiology of primary atrophic rhinitis including chronic infection of the nose and paranasal sinuses by Klebsiella ozaenae, nutritional deficiency of iron, fat soluble vitamins and proteins, lower socioeconomic status and poor hygiene. Hormonal, genetic and autoimmune theories have also been proposed [3].
Atrophic rhinitis may be a common condition but cases with maggot infestation are relatively rare. Studies focusing on nasal myiasis are also difficult to find. Our study, by profiling the incidence of maggot infestation in patients with atrophic rhinitis would contribute significantly to the literature.
To study the demographic features of atrophic rhinitis cases with maggot infestation (nasal myiasis) among the population in North Karnataka with respect to age and sex distribution, anaemia association, clinical presentation (unilaterality/bilaterality) and seasonal variation.
Materials and Methods
This retrospective study was conducted in the Department of ENT, Bidar Institute of Medical Sciences, Bidar. As per the records maintained by OPD of ENT Department, between 2006 and 2015, there were 190 reported cases of atrophic rhinitis. Of these, 33 cases showed maggot infestation and were admitted for treatment. The detailed records of these patients were available and collected. These formed our study group. The patients of atrophic rhinitis without nasal myiasis were treated on outpatient basis.
Inclusion criteria: All the patients of atrophic rhinitis with nasal myiasis admitted between 2006 and 2015.
Exclusion criteria: The patients of atrophic rhinitis without nasal myiasis were excluded from the study.
Details of age, sex, unilaterality, bilaterality, association with anaemia, seasons, were noted and discussed. The patients were grouped into five age groups; below 15, 16-24, 25-44, 45-64, and 65 and above.
Results
Out of 190 cases of atrophic rhinitis, 33 (17.4%) cases showed maggot infestation. These cases form our study group. Age for these 33 patients ranged between 12 and 90 years with a mean age of 56.76±17.68 years. The most affected age group was 45 to 64 years, with 16 (48.5%) cases, followed by the 65 year and above age group, with 11 (33.3%) cases. The age group below 15 years showed least number with two cases (6.1%). The female to male ratio was found to be 3.1:1 [Table/Fig-1]. Overall, the study group showed presence of 25 (75.8%) female patients and 8 (24.2%) male patients.
Age (years), sex and anaemia (number of patients) distribution of atrophic rhinitis cases with maggot infestation.
| Age | Sex | Anaemia |
|---|
| Male | Female | Present | Absent |
|---|
| Below 15 | 0 | 2 | 1 | 1 |
| 16-24 | 0 | 0 | 0 | 0 |
| 25-44 | 1 | 3 | 3 | 1 |
| 45-64 | 4 | 12 | 16 | 0 |
| 65 and above | 3 | 8 | 11 | 0 |
Most of the patients, i.e., 31 (93.9%) were anaemic with older age groups registering 100% anaemic cases [Table/Fig-1]. Identical number of cases i.e., 31 (93.9%) showed bilateral involvement and only 2 (6.1%) showed unilateral involvement.
The years 2007 and 2008 registered maximum number of cases with 6 (18.2%) and only 1 (3%) case was reported in the years 2014 and 2015 [Table/Fig-2]. Overall there has been a steady decline in number of cases in recent years [Table/Fig-2] With respect to seasonal variation, more number of maggot infested atrophic rhinitis cases were clustered around the months of October, November and December [Table/Fig-3].
Year wise distribution of atrophic rhinitis cases with maggot infestation. (x-axis: year wise distribution of atrophic rhinitis; y-axis: number of registred cases of atrophic rhinitis
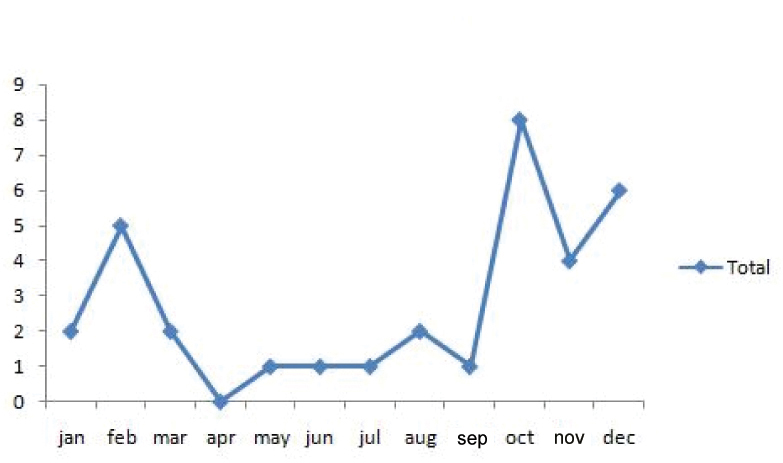
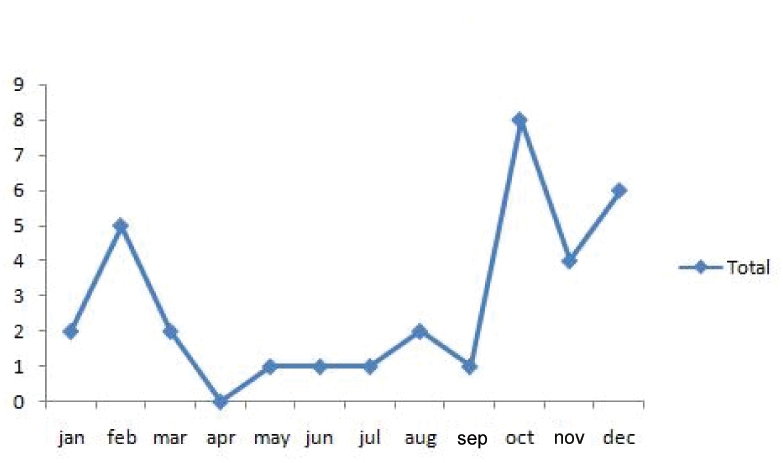
Seasonal variation: based on month wise distribution. (x-axis: month wise distribution of atrophic rhinitis; y-axis: number of registred cases of atrophic rhinitis)
Discussion
Spenser Watson of London was first to describe clinical features of this disease and called it Ozaenae [1]. Rhinitis sicca, Dry rhinitis, Open Nose Syndrome and Empty Nose Syndrome are the various names given to this chronic embarrassing debilitating disease involving nasal cavity and paranasal sinuses. Fraenkel first described the classic triad of symptoms which was virtually diagnostic of this disorder [1]. In his honor Fetor, Crusting and Atrophy of nasal structures is known as Fraenkel’s triad. Frank Bosworth in 1881 noted that ‘Breath from these patients was not only unpleasant but virtually unbearable. The sufferer per se was mercifully unaware because of the presence of anosmia [1].
There are foul smelling crusts formed due to drying up of viscid secretion. This foul odour is known as Ozaenae [4]. The nasal cavity is abnormally roomy. The associated anosmia makes patients unaware of the stench emanating from the nose [5].
The number of cases of atrophic rhinitis with maggot infestation that we observed in our outpatient department persuaded us to take up this demographic study. Moreover, though atrophic rhinitis is common in India, there are no published reports about nasal myiasis in atrophic rhinitis from our part of the country namely Northern Karnataka. Author’s objective is to throw light on this condition with respect to age and sex distribution, it’s possible association with general health and socioeconomic status of the patients and any association with seasons.
In our study, we had 190 cases of atrophic rhinitis over a nine year time period. Out of these, 33 presented with maggots in the nose which accounted for 17.4% of total atrophic rhinitis cases. Our report is comparable with the study by Bist SS et al., with an incidence of nasal myiasis of 26.6% [3]. Our literature search also revealed that there are not many studies about atrophic rhinitis cases with maggot infestation.
The higher incidence seen in our study and the study by Bist SS et al., could be due to the fact that both these studies were conducted in India, with most of the patients belonging to lower socioeconomic strata and rural area [3]. The lack of hygiene in these patients could have resulted in higher maggot infestation compared to the studies conducted in developed countries. This disease is rather rare in developed countries [6,7].
Also, these studies were conducted in tertiary care centres where the more advanced cases are referred for treatment. This could have resulted in the proportion of maggot infestation case being on the higher side in our study. This observation needs authentication with future studies.
Atrophic rhinitis has been described as a disease of the young with a predilection for the third and fourth decade of life [1] and a disease of middle aged with age of occurrence between 41 and 50 years [3]. In another study with a clinical profile of 62 cases of atrophic rhinitis maximum cases were in age group of 11-20 years [8]. Similar to this were the reports of Shreedharan SS et al., with 67% of atrophic rhinitis cases in the age group of 11-30 years [9]. On the other hand, our study shows that nasal myiasis due to atrophic rhinitis is seen more in the older age group (45-64 and >64). The reasons for this could be varied. Firstly, the presence of a more advanced form of the disease as the patients reach the older age group may predispose them to infestation by maggots. Secondly, the neglect in care of these older individuals by the caretakers in the family and the inability to maintain proper hygiene themselves due to infirmity also contributes. Lastly, the lack of immunity as the age progresses may predispose them to maggot infestation.
In our study, there was a female predominance in the maggot infestation cases due to atrophic rhinitis with the female to male ratio being 3.1:1. This was in accordance with the female predilection of atrophic rhinitis seen in other studies. In a study by Bunnag C et al., female to male ratio was 5.6:1 [2] and in the study by Bist SS et al., it was 2.5:1 [3].
The possible explanation for female gender being the commonly affected one is oestrogen deficiency. The fact that this disease manifests in prepubertal girls and aggravates during menstruation and pregnancy support this theory. There is also evidence that symptoms improves with oestrogen therapy [4,10]. Same explanation may hold good for atrophic rhinitis with maggot infestation.
When age and sex distribution of atrophic rhinitis cases with maggot infestation was observed it was seen that maximum number of female patients were seen in two age groups, that is 45-64 (n=16) and 65 and above (n=11) [Table/Fig-1]. However, there is no literature supporting our data.
Nutritional deficiencies including Vitamin A deficiency and iron deficiency have also been reported as possible causes of atrophic rhinitis by many authors [11-15]. However, a study from Norway reported a high incidence of iron deficiency anaemia without a relatively high incidence of atrophic rhinitis [16]. The study on Thai patients also did not confirm the significance of a nutritional factor [3].
Bist SS et al., in their study had observed a low haemoglobin level in 46.6% cases of atrophic rhinitis confirming the significance of a nutritional Factor in the aetiology of atrophic rhinitis [3]. In our study, 31 out of 33 patients with nasal myiasis (93.9%) were anaemic. Further studies on large sample size are needed to support the aetiological role of nutritional deficiency, especially anaemia, in the causation of atrophic rhinitis.
When age and anaemia association of atrophic rhinitis cases with maggot infestation were seen, we observed that maximum cases were in 45-64 age group (16) and 65 and above age groups (11) [Table/Fig-1]. However, even for this observation there is no literature support.
All the patients in our study resided in rural areas lending credence to the theory that the rural population is more susceptible to atrophic rhinitis and consequently to nasal myiasis. Their poor socioeconomic status, poor hygiene and cooking practices using open stoves with wood, cow dung cakes and coal with kerosene oil may be also contributing to this disease process. This theory is supported by Bunnag C et al., in their study on Thai population, 70% of which was from rural areas [2].
In our study, 93.9% cases had bilateral presentation. Literature review also substantiates the fact that unilateral cases are rare and seen mainly in cases with severe deviated nasal septum [17]. In a study by Shreedharan SS et al., out of 82 cases of atrophic rhinitis, 96% showed bilateral presentation [9].
Year wise distribution of atrophic rhinitis cases with maggot infestation showed an upward trend from 2006 to 2008 with 5-6 cases per year. Subsequent years have shown a decline with both 2014 and 2015 registering one case each [Table/Fig-2]. This decline might be due to the improved socioeconomic status, increased awareness about health and hygiene practices of this population. Follow up studies will be needed in this regard [9].
A study reveals that nasal myiasis is seen mostly in the months from August to October [18]. In our study, the maximum number of nasal myiasis cases were clustered around the months of October (8 cases), November (4 cases) and December (6 cases). The month of February also showed a peak with 6 cases [Table/Fig-3]. This may be due to the relatively cooler and moist climate prevailing in India during these months which is favourable for the breeding of the flies. This observation needs further authentication by studying seasonal variations in a larger sample from various places.
The management of nasal myiasis involves manual removal of the maggots after instilling chloroform and turpentine drops into the nose [19]. The management of atrophic rhinitis ranges from conservative to the surgical treatment. The conservative management consists of alkaline nasal douching, 25% glucose in glycerine nose drops, kimecitine nasal drops [20]. Surgeries for atrophic rhinitis aim at reducing the size of the wide roomy nasal cavity by submucoasal placement of various materials. Young’s operation and modified young’s operation close the nasal cavity and help in keeping it moist [7].
Limitation
Limitation of our study is that we couldn’t compare the demographic parameters of atrophic Rhinitis cases with and without maggot infestation because of lack of data.
Conclusion
Atrophic rhinitis may be a common condition but cases with maggot infestation are rare. Our study, by profiling incidence of maggot infestation contributes significantly to the literature. Atrophic rhinitis with nasal myiasis is multifactorial having a Female predilection, association with older age group, poor nutrition and anaemia. Patients from rural area are more prone for nasal myiasis. It also shows a seasonal variation with more incidence in the relatively cooler months of October, November and December.