Psoriasis is an inflammatory T-cell mediated disease affecting 125 million people throughout the world. According to published reports, prevalence in different populations varies from 0.1% to 11.8%. In India, the prevalence of psoriasis varies from 0.44% to 2.8% [1-3]. The most common form of psoriasis is psoriasis vulgaris, which is characterized by sharply demarcated, red, and scaly symmetrical plaques on the elbows, knees or scalp. The precise pathologic mechanism of psoriasis is still unknown. Increased levels of proinflammatory cytokines (e.g., TNF-α, IL-1β, IFN-γ, IL-2, and IL-12) have already been demonstrated by many authors [4-9]. Few studies have reported increased expression of numerous adhesion molecules (ICAM-1, ICAM-3, sE-selectin) in the psoriatic skin [10]. But it is still not clear if it can be used as a marker of disease severity [11-13]. Thus, we aim to study the levels of sE-selectin in patients of psoriasis, see their correlation with disease severity and then finally see the effect of therapy on sE-selectin levels.
Materials and Methods
A descriptive cross-sectional hospital based study was conducted in the Department of Pathology in collaboration with the Department of Dermatology, Lady Hardinge Medical College and Associated Hospitals, New Delhi from November 2011 to March 2013. Ethical clearance was taken from the Institutional Ethical Committee. A total of 52 newly diagnosed cases of psoriasis of age group ranging from four years to 80 years, attending the Dermatology OPD of Smt Sucheta Kriplani Hospital were included in the study group. Patients not giving consent and known cases of any other acute or chronic inflammatory conditions, hypertension, diabetes mellitus, allergies, SLE, rheumatoid arthritis or liver disease were excluded from the study. Clinical features and demographic characteristics were assessed in all cases.
The severity of psoriasis was assessed by the PASI for each patient. Disease severity was scored on the basis of PASI (0-72) and further classified into mild (0-7), moderate (7-12) and severe (>12) [14]. Venous blood sample was taken from 52 patients and 30 age and sex matched controls comprising of healthy, non psoriatic volunteers with no family history of psoriasis. Levels of sE-selectin were determined by ELISA kit method.
Skin biopsy was taken from the affected site. A signed informed consent was taken and each patient was subject to detailed history and thorough clinical examination.
Of the 52 patients, both pre therapy and post therapy assays were done in six cases. Rest of the patients either had poor compliance to treatment or were lost to follow up. The patients were given topical therapy using coal tar (6%) and salicylic acid (3%) combination ointment to be applied on the affected areas at night daily and dithranol to be applied every alternate day on the affected areas. The patients were followed up every three weeks and then the serum sE-selectin assays were done after six months of start of therapy.
Results
Majority of cases (38.5%) were in the age group 31-40 years. Mean age of affliction was 35.96±4.78 years which predominantly were males (M:F ratio was 1.89:1). Females had a slightly earlier age of onset of psoriasis as compared to males. The age of patients with psoriasis Vulgaris ranged from 6 to 80 years (mean 39.62), guttate psoriasis ranged from 5 to 33 years (mean 20.4 years) and ranged from eight years to 56 years in palmoplantar psoriasis (mean 32.40). Two patients of Pustular Psoriasis were of age 4 and 17 years.
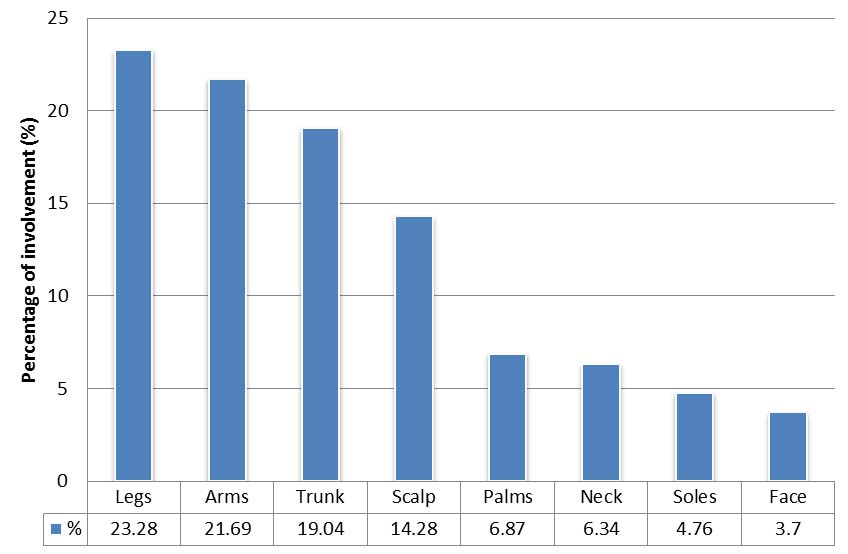
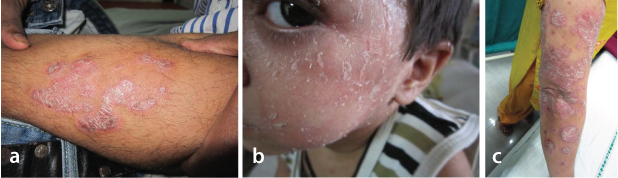
Extremities (44.97%) were the most common site involved of which legs were most common (23.28%). Face was the least common site to be affected (3.70%) [Table/Fig-1]. PASI score ranged from a minimum of 1.3 to a maximum score of 18.4 (Mean 5.58±4.17). There were 40 cases (76.92%) belonging to mild grade [Table/Fig-2a], 7 cases (13.46%) and 5 cases (9.61%) belonged to moderate [Table/Fig-2b] and severe grade [Table/Fig-2c] of disease respectively. The males were more in number as compared to females in all degrees of severity. Severe cases seemed to have a little earlier age of onset (29.80±17.32 years) as compared to moderate (42.85±10.12 years) and mild (35.52±15.02 years) cases. However, there was no statistically significant difference between them (p=0.303).
Percentage of different sites of involvement.
a) Mild psoriasis; b) Moderate psoriasis; c) Severe psoriasis.
Psoriasis vulgaris was the predominant type comprising of 40 (76.92%) cases. A total of 5 (9.61%) cases were of guttate psoriasis, 5 (9.61%) of palmoplantar psoriasis and 2 (3.88%) cases were of pustular psoriasis.
PASI score was highest in cases of pustular psoriasis (mean 11.10). It was lowest in cases of palmoplantar psoriasis (mean 2.92).
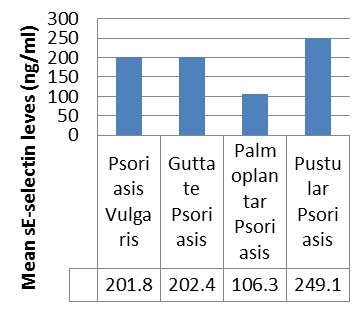
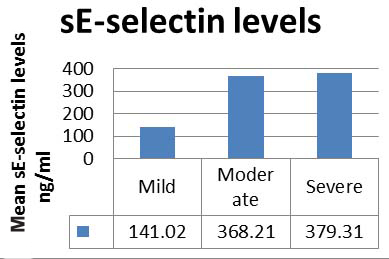
The serum level of sE-selectin was significantly higher in 52 cases as compared to controls (Student’s t-test, p<0.001). The sE-selectin levels in cases ranged from 47.1 ng/mL to 586.15 ng/mL with a mean of 194.52±133.35 ng/mL and in controls ranged from 8 ng/mL to 110 ng/mL with a mean of 30±55.77 ng/mL. There was no statistically significant difference between the PASI scores and serum sE-selectin levels in patients of psoriasis vulgaris, palmoplantar psoriasis and guttate psoriasis (p=0.127 and p=0.458) [Table/Fig-3]. There was significant correlation (p<0.001) between serum levels of sE-selectin in cases (mean 194.52 ng/mL) and PASI score. The serum levels of sE-selectin were significantly raised in all mild, moderate and severe cases as compared to controls (ANOVA p<0.001) [Table/Fig-4]. The serum levels of sE-selectin were raised in moderate and severe cases as compared to mild cases (p<0.001). The levels in moderate and severe cases were not significantly different when compared to each other (p=1.000).
sE-selectin levels in different types of psorasis.
sE-selectin levels in mild, moderate and severe cases.
On follow up of six patients, there was decrease in PASI and serum sE-selectin levels as compared to pre therapy levels, but not enough to reach statistical significance (paired t-test, p=0.279 and p=0.116 respectively). After topical therapy serum sE-selectin levels in cases although showed a decline, they remained significantly higher than controls (paired t-test, p<0.001) [Table/Fig-5].
PASI score and sE-selectin levels before and after therapy.
| Case no. | PASI Score | sE-selectin |
|---|
| before | after | before | after |
|---|
| 2 | 2.7 | 2.5 | 108.99 | 115.87 |
| 19 | 1.8 | 2.3 | 144.75 | 110.02 |
| 22 | 1.8 | 2 | 182.52 | 120.11 |
| 38 | 1.6 | 1.1 | 112.1 | 120.98 |
| 44 | 8.8 | 5.7 | 328.54 | 149.23 |
| 49 | 6 | 3 | 187.5 | 44.78 |
Discussion
Psoriasis is a chronic autoimmune disease that causes thick, reddened, scaly, itchy or sore areas. The importance of T-cell activation has already been demonstrated in the pathogenesis of psoriasis [15,16]. T-cells migrate to the skin vasculature and slow down, in a process called rolling. This involves Cutaneous Lymphocyte Antigen (CLA) on T-cells and E-selectin (ELAM, endothelial leukocyte adhesion molecule-1) on the endothelial cell which is expressed in response to cytokines like IL-1 and TNF-α by affected cells [17]. E-selectin in participates in the conversion of rolling to firm adhesion [18] and then via diapedesis T-lymphocytes enter the tissue.
Finally these activated T-cells induce hyperproliferation in keratinocytes and expression of adhesion molecules by endothelial cells. These activated keratinocytes produce growth factors stimulating neutrophil influx, vascular alterations, and keratinocyte hyperplasia which causes the characteristic skin lesions of psoriasis [16,19].
The present study included 52 cases of psoriasis. Majority of cases (38.5%) were in the age group 31-40 years, the age of patients ranging from 4-80 years. Mean age of affliction was 35.96±4.78 years. Mean age of males was slightly higher (37.76 years) as compared to females (32.55 years). The age groups in various studies ranged from 18 to 85 years [12,20-22]. Similar to the present study Czech W et al., and Ghalamkarpour F et al., reported the mean age of patients to be 31 years and 37.52±16.8 years respectively [12,13]. Whereas Kowalzick L et al., Long JW et al.,, and Yamamoto T et al., reported the mean age of patients as 46.0±9.8 years, 58.4 years and 36 years respectively [11,20,22]. In the present study, the age of patients with Psoriasis Vulgaris ranged from 6 to 80 years; mean age being 39.62 years, of those suffering from Guttate Psoriasis ranged from 5 to 33 years, mean age being 20.4 years. The age of patients varied from 8 years to 56 years in Palmoplantar Psoriasis mean age being 32.40 years. Two patients of Pustular Psoriasis were aged 4 and 17 years. There was a significant difference (p=0.002) between the age of patients with Psoriasis Vulgaris and of those with guttate psoriasis. This is in concordance with the already known increased prevalence of guttate psoriasis in children as compared to adults [23].
In the present study, majority of cases were males (65.4%) with the male: female ratio being 1.89:1. Similarly males predominated in the studies by various authors [12,13,21].
PASI score: Our cases had PASI score from a minimum of 1.3 to a maximum score of 18.4, mean PASI being 5.58±4.17. Yamamoto T et al., included patients of psoriasis vulgaris in their study who had a PASI of more than 20 [22]. Similarly, Kowalzick L et al., included patients of chronic plaque type psoriasis with PASI more than 10, mean PASI of the cases being 18.6±7.2 [11]. The patients in the study by Ghalamkarpour F et al., had PASI ranging from 0.9 to 55.8 and 9.9 to 50.2 respectively, mean PASI being 19.61 and 23.7 respectively [13].
The severe cases seemed to have a little earlier age of onset (29.80±17.32 years) as compared to moderate (42.85±10.12 years) and mild (35.52±15.02 years). But there was no statistically significant difference between them (p=.303). The males were more in number as compared to females in all degrees of severity, which was in concordance with the overall predominance of males over females. To the best of our knowledge, none of the previous studies on sE-selectin divided the psoriasis cases into mild, moderate and severe based on PASI score.
sE-SELECTIN levels in psoriasis: In the present study, serum levels of sE-selectin were significantly (p<.001) raised in cases (194.52 ng/mL) as compared to controls (55.77 ng/mL). Similar results were obtained in a study by Kowalzick et al [11] where he reported significantly higher levels (p<.001) in cases (111.9 ng/mL) as compared to controls (55.5 ng/mL). Yamamoto T et al., studied patients with generalised pustular psoriasis and psoriasis vulgaris and found significantly increased (p<0.005 and p<0.01 respectively) levels as compared to controls [22]. Other studies by Czech W et al., Long JW et al., Borska L et al., and Krasowska D et al., have also reported significantly higher levels of sE-selectin in psoriasis cases as compared to controls [12,20,21,24]. Similar results were quoted recently by Dowlatshahi EA et al., in a meta-analysis of 7852 individuals, he concluded that sE-selectin levels were twice as high in cases as compared to controls [25]. However, Ghalamkarpour et al., in 2010 reported higher levels of sE-selectin in cases of Psoriasis (34.63 ng/mL) as compared to controls (24.93 ng/mL) but the values were not statistically significant (p=0.240) [13]. Krasowska et al., divided the cases into acute (>2 months duration) and chronic (<2months duration) and found that levels in both acute and chronic cases were significantly higher than controls (p<0.001) [24].
In the present study, psoriasis vulgaris (chronic plaque type) was the predominant form of psoriasis comprising of 40/52 cases (76.9%). In the present study, higher levels of sE-selectin were seen in pustular psoriasis (249.06ng/mL) as compared to cases of psoriasis vulgaris (200.47 ng/mL) but they could not be statistically analysed as there were only 2 cases of the pustular psoriasis. Yamamoto T et al., compared levels of sE-selectin in patients of generalised pustular psoriasis and psoriasis vulgaris [22]. They observed that levels were higher in patients with generalised pustular psoriasis (106.2±32.8 ng/mL) as compared to psoriasis vulgaris patients (83.8±26.0 ng/mL) but there was no statistically significant difference between them.
The sE-selectin levels significantly correlated (p<0.001) with the severity of disease (PASI score) in the present study. Various studies have described the correlation between sE-selectin and PASI but there is no concurrence of results. Kowalzick L et al., reported significant positive correlation (p<0.002) with PASI [11]. Similar positive correlation has been obtained by Ghalamkarpour F et al., and Long TW et al., [13,20]. On the contrary, Czech W et al., and Borska L et al., did not show any significant correlation between sE-selectin levels in PASI [12,21]. Krasowska D et al., divided psoriasis cases into acute (duration >2 months) and chronic (duration <2 months) [24]. He found that the levels of sE-selectin in acute cases correlated significantly with PASI (p<0.05). However, there was no correlation between sE-selectin levels in chronic cases and PASI (p<0.97).
Post-topical therapy, the patients in the present study showed a reduction in PASI, although none had complete clearance of lesions. The reduction in PASI score was not statistically significant (p=0.279). We postulate that this could have been due to requirement of alternative therapy by the patient. Borska L et al., reported a significant (p<0.001) reduction in PASI after Goekerman’s therapy (crude coal tar and UV radiation) [21]. The mean PASI score before treatment was 22.2±6.9 and it reduced to 6.3±3.7 after therapy. Long T et al., also studied the effect of therapy (narrow band UV-B) on psoriasis patients [20]. He reported a significant reduction (p<.001) in PASI values of patients after UV-B therapy (mean PASI 6.02±2.07) as opposed to pretreatment values (mean PASI 23.70±10.14). Czech W et al., also reported a significant decrease (p<0.05) in PASI score of cases after treatment with dithranol and petrolatum for two to four weeks [12]. Kowalzick L et al., Czech W et al., and Krasowaska D et al., did not report any significant decrease in sE-selectin levels after topical therapy similar therapy [1,12,24]. On the Contrary, Borska L et al., reported significant decrease (p<0.05) in sE-selectin levels from 91.03±59.85 ng/mL to 85.36±49.83 ng/mL after 8 to 30 days (average 17 days) of Goekerman’s therapy (crude coal tar and UV radiation) [21]. Long JW et al., also studied serum sE-selectin levels after UV-B phototherapy [20]. The serum sE-selectin levels reduced from 88.82±19.72ng/mL to 79.96±17.50ng/mL. This decrease was statistically significant (p=0.000) as compared to pretreatment levels. Similar results were provided by Sorour N et al., in a recent study leading to significant reduction in E-selectin levels after UV-B phototherapy [26].
Meissner M et al., have studied dimethyl fumarate drug and recommend it in treatment of moderate to severe psoriasis [27]. Dimethyl fumarate also has anti-E-selectin properties which is a possible mechanism for disease remission. Similarly Egger J et al., mention that anti-selectin may be a promising starting point for the development of novel anti-inflammatory drugs [28].
Adhesion molecules provide attractive targets for immune-interaction strategies for several skin diseases including psoriasis. No treatment till date is successful in clearance of the disease. Immunotherapy in the form of e-selectin antagonists and a demonstration of their efficacy in a disorder such as psoriasis can provide compelling proof of concept evidence for novel treatments.
Limitation
Present study was limited by the number of cases as only newly diagnosed cases without any prior treatment were included. Only the patients to be treated with topical therapy were included for follow up for the uniformity of the treatment protocol.
Further wider studies are required to fully establish the role of this adhesion molecule as marker for severity or follow up of patients with psoriasis.
Conclusion
Thus, serum sE-selectin levels correlate with disease severity and fall down after therapy. Serum sE-selectin estimation has a role in predicting the course of disease and monitoring therapy. Hence, administration of specific immunotherapy at an early stage can prevent exacerbations in the patient, thus saving the patient from physical and psychological trauma.