Posterior Right Sectoral Duct Downstream of the Cystic Ductal Opening: A Rare Variant
Zeineb Mzoughi1, Houcem Fadhl2, Achref Djebbi3, Ghofrane Talbi4, Mohamed Taher Khalfallah5
1 Assistant Professor, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
2 Resident, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
3 Resident, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
4 Assistant Professor, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
5 Professor, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Zeineb Mzoughi, Assistant Professor, Department of General and Digestive Surgery, CHU Mongi, Slim Sidi Daoued, Tunis, Tunisia.
E-mail: mzeineb@yahoo.com
The anatomical variants of the posterior right sectoral duct of the biliary tract are frequent. They have a surgical importance involvement. We report a case of 63-year-old female patient operated by laparoscopy for acute cholecystitis with an intraoperative cholangiography discovery of an insertion of the posterior right sectoral duct on the bile duct below the cystic duct. The insertion of the posterior segmental canal on the bile duct could represent type A6 of the Huang classification. This biliary variation should be known to avoid posterior segmental canal injury, during cholecystectomy.
Anatomy, Bile duct, Cholecystectomy, Laparoscopy
Case Report
A 63-year-old woman presented to the emergency department with complaint of fever and paroxystic right hypochondrium pain since three days without any other signs. The physical examination found guarding of the right hypochondrium and fever at 100.4°F. She did not have jaundice. Haematological and biochemical investigation showed presence of Leucocytosis with WBC count at 13500 cells/mm3 and C-reactive protein 72 mg /l, total bilirubin 20 μmol/l with Direct bilirubin 2.8 μmol/l, alkaline phosphatases 64 UI/l and GGT 15 UI/l. There were no signs of hepatic cytolysis.
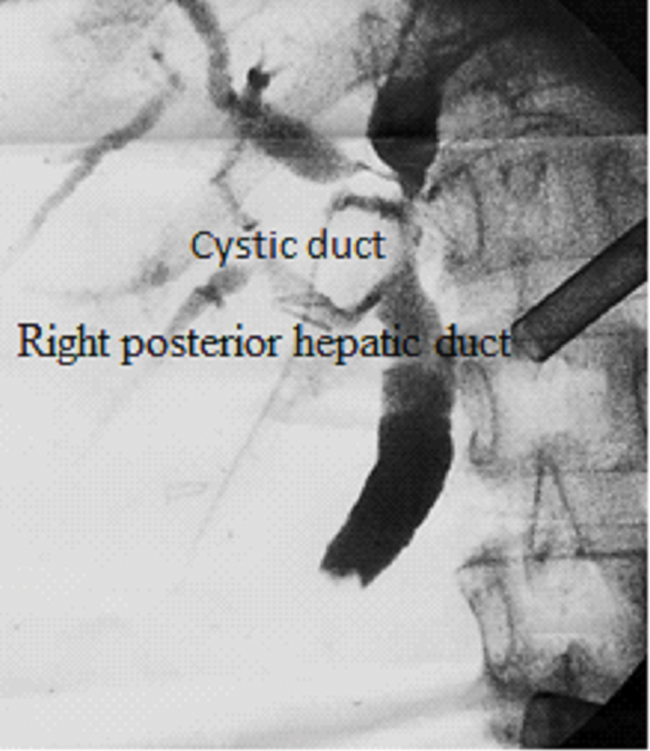
The abdominal ultrasound showed acute lithiasic cholecystitis. The intra and extra-hepatic bile ducts were thin. The patient was operated laparoscopically. The exploration found acute phlegmonous cholecystitis with intense pediculitis. The cystic duct was large containing multiple micro-calculations. Operative cholangiography through a transcystic drain was performed. It showed a dilation of the main bile duct upstream of a lacunar image in the lower bile duct [Table/Fig-1].
Intraoperative cholangiography showing the abutment of the posterior segmental canal on the main bile duct separately and downstream of the cystic duct opening.
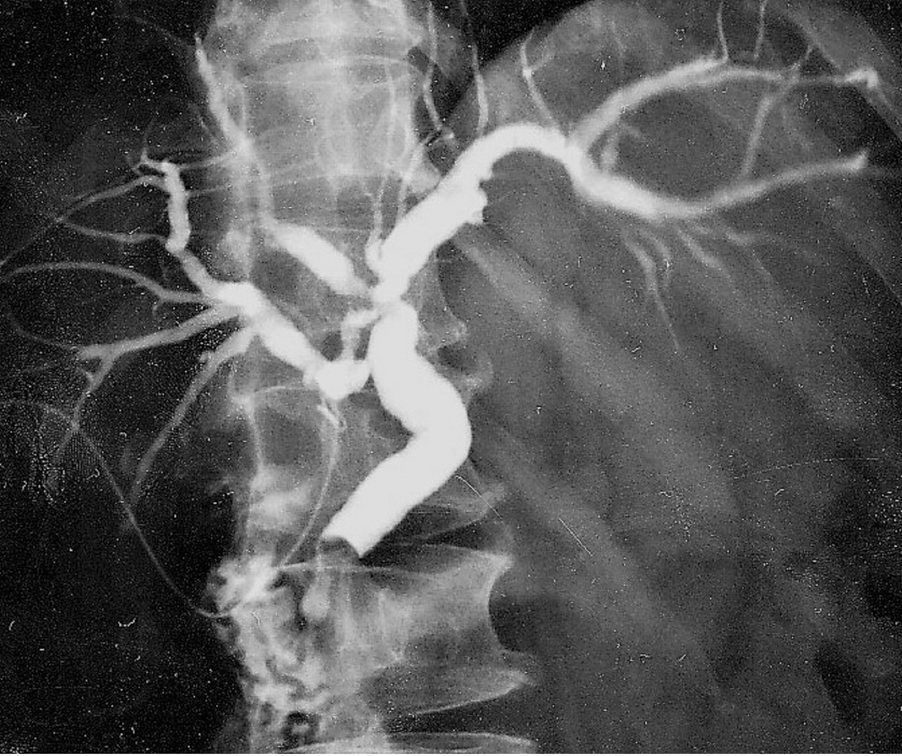
There was also a sliding of the posterior segmental canal with an insertion at the bile duct below the cystic duct, well identified by the transcystic drain [Table/Fig-2]. In the highly inflammatory atmosphere, the transcystic drain was left in place and a postoperative endoscopic sphincterotomy was scheduled. The postoperative course was uneventful. Cholangiography, through the transcystic drain, was repeated at the postoperative stage. It showed the same appearance with a persistence of the lacunar image in the lower bile duct [Table/Fig-2]. An endoscopic sphincterotomy with calculus extraction was then performed with simple course. The transcystic drain was removed after one month. The patient goes well after one year of follow up.
Cholangiography of control in left lateral decubitus showing the same aspect as on intraoperative cholangiography.
Discussion
In the modal distribution, the right posterior segmental bile duct joins, from the back and the left, the right frontal canal to form the right hepatic duct. In the different series of the literature, this situation is only found in about 50% of the cases [1]. In 30% of cases, the posterior segmental canal merges with the left hepatic canal or its confluence with the anterior sectoral duct.
Huang TL et al., described a classification of the anatomical variations of right and left canals [2]. This classification made from living liver donors is more reproducible in surgical practice than the purely anatomical classification of Couinaud, made on dissection of cadavers [2]. The Huang classification describes five types of anatomical variations of the right hepatic duct [2]. In a recent prospective X-Ray series using the Huang classification, the types of right sector canals insertion were represented as follows: A1: 55.3%, A2: 9.3%, A3: 27.6%, A4: 4%, A5: 0.8%.
The insertion of the posterior right sectoral duct in the bile duct canal downstream of the cystic ductal opening has never been described by the various classifications [3]. The rarest anatomical variant (2%), described in case report [4], is the insertion of the right sectoral duct in the cystic duct. It would therefore be lawful for our patient to speak of an A6 type, not described by Huang. This entity should be known for the daily practice of the surgeon. Laparoscopic cholecystectomy is one of the most common, but not least feared interventions in terms of complications. The biliary injury would be more frequent with biliary or vascular variation [5], especially when these variations are rarely described [6]. In liver transplantation, knowing all the biliary anatomical variants that can be encountered is fundamental to avoid the loss of grafts in transplantation from cadaveric donor. In hepatic transplantation from living donor, the consequence of a biliary injury would be redoubtable.
Conclusion
The opening of the posterior right sectoral duct in the bile duct downstream of the cystic duct opening is an anatomical variant that has never been described. It can be perfectly integrated into the Huang classification (Type A6). This “situation” of the posterior sectoral duct has real clinical implications in laparoscopic cholecystectomy or hepatic surgery.
[1]. Cucchetti A, Peri E, Cescon M, Zanello M, Ercolani G, Zanf C, Anatomic variations of intrahepatic bile ducts in a European series and meta-analysis of the literatureJ Gastrointest Surg 2011 15(4):623-30. [Google Scholar]
[2]. Huang TL, Cheng YF, Chen CL, Chen TY, Lee TY, Variants of the bile ducts: clinical application in the potential donor of living-related hepatic transplantationTranspl Proc 1996 28(3):1669-70. [Google Scholar]
[3]. Sarawagi R, Sundar S, Raghuvanshi S, Gupta SK, Jayaraman G, Common and uncommon anatomical variants of intrahepatic bile ducts in magnetic resonance cholangiopancreatography and its clinical implicationPl J Radiol 2016 81:250-55. [Google Scholar]
[4]. Suna N, Disibeyaz S, Kuzu UB, Yuksel M, Yildiz H, Kayaçetin E, Aberrant right posterior hepatic duct opening into the cystic duct: a very rarely seen biliary anatomic variationEndoscopy 2014 46(1):E657 [Google Scholar]
[5]. Kavitha Kamath B, Dual cystic arteries in association with Caterpillar Hump of right hepatic artery. A case report and its surgical relevanceJ Clin Diagn Res 2015 9(7):AD01-02. [Google Scholar]
[6]. Kurumi Y, Tani T, Hanasawa K, Kodama M, The prevention of bile duct injury during laparoscopic cholecystectomy from the point of view of anatomic variationSurg Laparosc Endoc Percutan Tech 2000 10(4):192-99. [Google Scholar]