Urethral stricture is a mutifactorial obliterative disease of anterior urethra. Associated scar in the surrounding corpus spongiosum is known as ‘spongiofibrosis’ [1]. The scarring process can extend through the tissue of the corpus spongiosum and into adjacent structures. Contraction of this scar reduces the width of the urethral lumen. Anterior urethral stricture disease is a fairly common problem encountered by the urologists. The overall incidence of stricture disease varies from 0.6% to 0.9% worldwide [2]. Recent studies also find a similar rate of incidence of 0.9%, as compare to 1.4% in old series [3].
Strictures of the anterior urethra can be seen in patients of all ages, but their occurrence differs greatly among various populations [4]. Iatrogenic trauma is likely to be the most common cause of anterior urethral strictures now a day, however in some series inflammatory disease is responsible for the majority [5,6]. For a long time, urethral stricture disease is being managed by several procedures like dilatation, meatotomy, anastomotic or substitution urethroplasty using either grafts or flaps, but chances of recurrence, financial impact and morbidity of disease remains high [7].
In this study, we explored the epidemiology of urethral stricture disease along with evaluation and management in patients presenting in a teaching institute.
Materials and Methods
Study Design
Prospective observational study was undertaken in the Urology department from March 2012 to September 2014. Approval of institutional ethical committee was obtained. Patients were enrolled after taking written informed consent. Females, patients with neurological disease, prostatic enlargement and of less than 18 years were excluded from the study.
Data Collection
A total of 200 adult men of lower urinary tract symptoms were screened during the study period. All patients underwent initial work-up including history, physical examination, urine analysis, renal function measurement, uroflowmetry and Post-Void Residual (PVR) measurement. Stricture disease was suspected in cases with predominant obstructive symptoms, low Qmax or high PVR, with or without local evidence of lichen sclerosis. Retrograde Urethrography (RUG) and Voiding Cystourethrography (VCUG) was obtained in suspected cases followed by urethroscopy. Either radiological (RUG/VCUG) or urethroscopic evidence of stricture was necessary for confirmatory diagnosis. After work up of 200 patients, only 110 patients had radiological or endoscopic evidence of urethral stricture disease and were finally included in the study [Table/Fig-1] and further management of confirmed cases was recorded and patients were followed upto 1 year.
Screening of patients with non-prostatic, non-neurological lower urinary tract symptoms.
| Diagnosis | Number of cases (n=200) |
|---|
| Urethral stricture disease | 110 |
| Overactive bladder | 44 |
| Urinary tract infection | 20 |
| Chronic prostatitis | 14 |
| Underactive bladder | 7 |
| Bladder calculi | 5 |
Data Analysis
Patient’s demographics and stricture characteristics were obtained. Mean, median, standard deviation, percentage and range was utilized for presentation with the help of SPSS software (IBM Corporation, version 21.0). Primary Outcome of disease was defined as success or failure, and was analysed by site and procedure done. Success was labeled when patient voided with a Qmax of more than 15 ml/s or was able to calibrate urethra with a minimum of 12 Fr” catheter. Outcome was compared using Chi-square test. Alpha error was kept at 5% and confidence interval was set at 95%.
Results
Baseline Parameters
A total of 110 men with urethral stricture disease were included. Mean age was 38±15 years [Table/Fig-2]. Highest incidence was seen among the age group of 25-50 years (56.4%). Mean BMI was 23.5±4.2 kg/m2. Hypertension was the most common associated co morbidity (25.5%) followed by diabetes and cardiac disease. Addiction to tobacco chewing and smoking was seen in 43.6% and 20.9% of cases respectively.
Baseline parameters of study participants.
| Parameters | Frequency (n=110) |
|---|
| Age (years) | 38 ± 15 (12-80) |
| BMI (Kg/m2) | 23.5 ± 4.2 (17.0-38.5) |
| Residence | Urban-57 (51.8%)Rural- 53 (48.2%) |
| Religion | Hindu- 62 (56.4%)Muslim- 40 (36.4%)Others- 8 (7.2%) |
| Co-morbidity | Hypertension- 28 (25.5%)Diabetes- 14 (12.7%)Cardiac illness- 11 (10%)COPD- 4 (3.6%) |
| Addiction | Tobacco chewing- 48 (43.6%)Smoking- 23 (20.9%)Alcohol- 13 (11.8%) |
| Presentation | Primary- 92 (83.6%)Recurrent- 18 (16.4%) |
Presentation
Obstructing urinary symptoms including poor stream, straining, incomplete emptying and intermittency were the presenting complaints in 66% of the patients. Mean Qmax and PVR was 6.4±2.6 ml/s and 165±68 ml respectively. 30% of cases presented with Suprapubic Catheterization (SPC) in situ, done for acute retention of urine or following the trauma. Five patients had features of urosepsis. Renal function deterioration was discovered in three cases. Eighteen patients had previous history of urethral surgery and five of them were crippled (>3 surgical corrections). Phimosis with urethral discharge was found in five cases. Three patients had multiple fistulas.
Stricture Characteristics
Trauma was the most common aetiology seen in 39 patients (35.4%), followed by lichen sclerosis or Balanitis Xerotica Obliterans (BXO) [Table/Fig-3]. Trauma was mostly resulted from the road traffic accidents and 10 patients had pelvic fracture urethral distraction defect (PFUDD). The most common site of disease was bulbar region (36.4%), followed by external urethral meatus in the study. Stricture length ranged from 0.5 cm to 12 cm, with mean of 3.3±2.6 cm. A complete obstruction was discovered in 27.2% of cases, while rest had partial obstruction.
Urethral stricture characteristics of the study patients.
| Variables | Counts n (%) |
|---|
| Age wise incidence | <25 years- 6 (5.5%)25 – 50 – 62 (56.4%)50 – 75 – 38 (34.5%)>75 – 4 (3.6%) |
| Aetiology | Trauma- 39 (35.4%)BXO*- 26 (23.6%)Infection- 21 (19.1%)Idiopathic- 8 (7.3%)Catheterization- 6 (5.5%)Post-TUR- 6 (5.5%)Instrumentation- 2 (1.8%)Post-hypospadias- 2 (1.8%) |
| Site | Meatal- 30 (27.3%)Fossa navicularis- 11 (10.0%)Penile- 4 (3.6%)Bulbar- 40 (36.4%)Pan-anterior- 25 (22.7%) |
| Length | <1 cm- 9 (8.2%)1-2 cm- 37 (33.6%)2-4 cm- 41 (37.3%)4-6 cm- 17(15.4%)>6 cm- 6 (5.5%) |
| Degree | Complete- 30 (27.2%)Partial- 80 (72.8%) |
*- Balanitis xerotica obliterans.
Management and Outcome
For strictures involving meatus, meatotomy and Urethral Dilatation (UD) was successful in 83% of cases, while results of UD followed by Clobetasol and Tacrolimus application were inferior (67%, p=.233) [Table/Fig-4a]. Similarly for strictures extending upto fossa navicularis, UD and local agents proved less effective (60%). Though an extended meatotomy provided a less invasive alternative with excellent outcomes (100%, p=.099), splaying of urine and altered glans cosmesis were the main concerns. However in both these conditions, a Buccal Mucosal Graft (BMG) urethroplasty had higher and durable success rate (100%) in two years of follow up [Table/Fig-4b].
Comparison of various treatment options for urethral stricture disease according to site: a) Meatal strictures; b) Fossa navicularis and distal penile strictures; c) Bulbar urethral strictures; d) Pan-anterior urethral strictures.
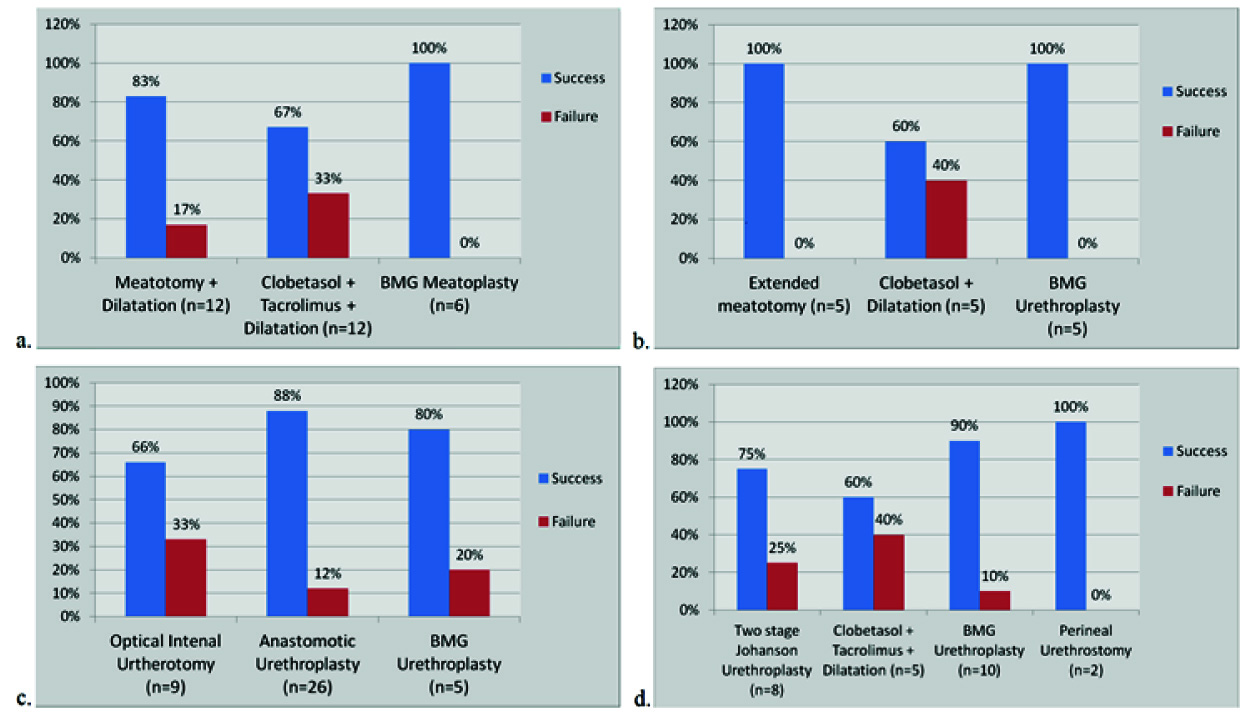
For small bulbar strictures (<2 cm), optical internal urethrotomy (OIU) was a minimally invasive procedure, but one third of cases failed to void satisfactorily. Anastomotic urethroplasty including perineal progressive approach successfully restored the normal urination in 88% of cases. In longer bulbar strictures, augmentation urethroplasty with BMG was successful in 80% of cases (p=.329) [Table/Fig-4c]. For pan-anterior strictures, two-staged johanson urethroplasty and BMG urethroplasty had 75% and 90% success rate in two years. For patients not opted for surgery, UD with local agents provided modest benefit (60%, p=.399) [Table/Fig-4d]. Two crippled cases ultimately chose perineal urethrostomy and both were continent.
Adverse Events
Minor complications were seen in eight cases. Six cases developed wound infections and were managed by partial opening of wound and dressings. Two cases had haematoma formation at the wound site, which required evacuation and pressure dressing. Recurrence of stricture was found in eight cases (4 in bulbar, 2 in pan-urethral and 2 in fossa navicularis). Urethro-cutaneous fistula was discovered in two cases following anastomotic urethroplasty for PFUDD.
Discussion
Stricture disease of urethra is commonly encountered in urological practice in both developed and developing countries. Data from developed world reveals a high prevalence after 55 years of age [8]. However, we found the majority of disease (61.9%) affecting a much younger population (<50 years). Reason may be the high rate of smoking and tobacco chewing in this region. Recent literature describes the trauma and iatrogenic factors to be the leading cause of the stricture disease [5]. In our series, though trauma due to road traffic accidents was the most common cause, BXO and infection together accounted for 42.7% of cases. Later conditions still accounts for a large burden of disease in developing nations. Obstructive LUTS are the classical presenting symptom in the literature; we additionally encountered many delayed presentations with complications including fistulas, deranged renal function and urosepsis [9].
Distal urethral strictures involving meatal, fossa navicularis and pendulous urethra differ from bulbar stricture with respect to their aetiology and nature [10]. Former are usually longer than bulbar strictures and most often have a non-traumatic aetiology [11]. In our series BXO and chronic infection caused majority of distal urethral strictures (70%), while trauma was the main culprit in bulbar strictures (90%). Average stricture length in bulbar region was 1.5±.7 cm, while in distal region it was 2.3±1.1 cm.
Management of urethral stricture disease within each urethral segment is determined by the individual aetiologic characteristics, cosmetics and availability of local tissues for the use in reconstruction [12]. For distal urethral strictures, recent studies support substitution urethroplasty over repeated UD or meatotomy [13]. We found later procedures to be effective in only 60-80% of cases, while BMG urethroplasty provided excellent results approaching 100%. Various claims of improvement after local application of Clobetasol, Tacrolimus along with UD has been made recently, but our results showed a modest benefit in around 60% of cases only [14].
Despite a high rate of recurrence after internal urethrotomy for bulbar strictures, it is the commonest procedure performed worldwide [15,16]. Out of our 40 cases of bulbar strictures, 26 (65%) underwent anastomotic repair. It still provided highest success rate (88%) compare to OIU (66%). Two third of OIU cases required a second OIU within 6 months. Cochrane database review analysed the efficacy of UD, OIU and urethroplasty in 2012. They failed to provide an answer to best treatment option due to lack of sufficient, well designed randomized studies [17]. However recent studies have shown a trend more in favour of definite open procedures compare to endourological [18,19].
Pan-urethral strictures are a surgical challenge as the inflammatory pathologies result in significant amount of spongiofibrosis. Results of repair are highly variable and range from 20-80% in the most series [20]. Kulkarni SB et al., reported good success with single stage BMG urethroplasty via perineal approach and penile inversion technique [21]. We utilized the same technique in 10 cases and nine were able to void satisfactorily. Two staged urethroplasty is also an attractive alternative especially in recurrent, post hypospadias and complicated cases with infection or fistula [22]. We performed it in eight of our cases with 75% success rate. UD with local agents were tried in five cases, who refused surgery. Only three of them could void successfully. Perineal urethrostomy was utilized as a last resort in two failed cases with multiple repairs.
Issue of intermittent self dilatation after urethroplasty is still unresolved due to lack of robust evidence [23,24]. Our protocol was to instruct the patients to perform self dilatation daily for one month after surgery and decrease the frequency to once a week in next six months. After one year self dilatation was stopped. Follow up guidelines after urethroplasty are also non-uniform and consisting of use of flexible urethroscopy, PVR measurement, uroflowmetry, retrograde urethrogram and patient reported outcome over a variable intervals [25]. We followed the patients three monthly with PVR and uroflowmetry.
Limitation
Limitations of this study are the limited number of cases, lack of cost analysis, sexual function measurement and patient reported outcomes. A large prospective multicentre randomized study is suggested including these issues.
Conclusion
Urethral stricture disease affects more of young and middle age population. Trauma, BXO and infections are the leading causes. Disease location and extent in different segments of urethra impart an additional challenge. Its management continues to evolve with results favouring urethroplasty over internal urethrotomy and dilatation. For longer and recurrent strictures, substitution urethroplasty offer excellent success rate. Intermittent self catheterization appears to offer long term benefit.