Scapula and clavicle are normally held together in humans by acromioclavicular joint and coracoclavicular ligament. Coracoclavicular ligament extends from posterosuperior surface of coracoid process to conoid tubercle and trapezoid line on inferior surface of lateral third of clavicle. A bursa is present between its conoid and trapezoid part. Sometimes a real joint, known as CCJ, can exist between conoid tubercle of clavicle and superior surface of coracoid process, which is surrounded by a capsule and lined by synovium, and the two bony surfaces are covered by cartilage [1]. True synovial nature of joint with cartilage and synovial fluid is also confirmed by magnetic resonance imaging [2].
During embryonic period coracoid process is connected with clavicle by cartilaginous procoracoid which becomes fibrous and ultimately transforms into coracoclavicular ligament. On the surface of ligament, nests of chondrocytes and even small nodules of cartilage are frequently seen. The conoid tubercle, which is usually in form of small rough surface elevation, occasionally grows out in the direction of coracoid process. The coracoid process may also react by forming a similar outgrowth. The two processes can then form real joint. In case of formation of joint, two processes are covered by cartilage and are surrounded by a capsule and lined by synovium. CCJ is a normal morphological trait in gorillas and gibbons [1]. Existence of this joint in humans was first reported in the latter half of nineteenth century [3]. It was thoroughly described way back in the end of nineteenth century [3-5], since then several osteological, radiological and cadaveric studies have reported the existence of this anomalous joint in various population. Recently a meta-analytical study reported that true prevalence of CCJ is approximately 2.7%, 5% and 7% respectively in radiological, skeletal and cadaveric studies [6].
Earlier CCJ was considered as fantasy of anatomists only and was neglected by clinical circle as it is rarely symptomatic, but incidental findings, in cases of intractable shoulder pain, created awareness in them too. If CCJ is symptomatic, lack of awareness of such entity may lead to delayed diagnosis or inappropriate management. Like other synovial joints, it can also develop osteoarthritic changes and is additionally said to be a predisposing factor for the degenerative changes of neighboring joints [7,8].
Our interest in the subject arose due to an incidental finding of facet for coracoclavicular as well as costoclavicular joints, both on the same clavicle in two cases [9]. We, then, further explored the literature for prevalence of this particular joint and found a few osteological and radiological studies from Delhi [10,11] and cadaveric study from Southern India [12]. Therefore, present study was undertaken to see the prevalence of coracoclavicular joint in North India.
Materials and Methods
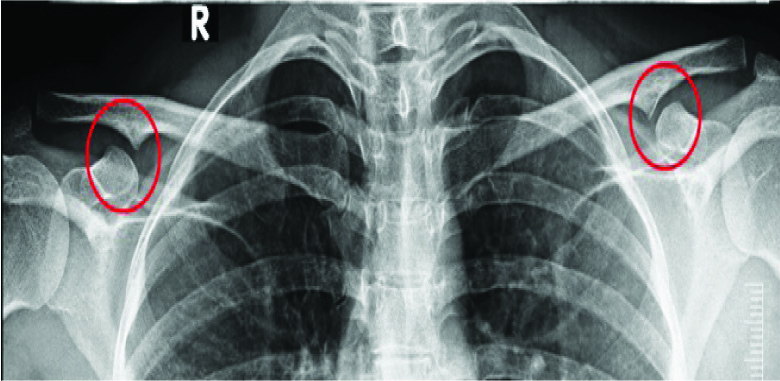
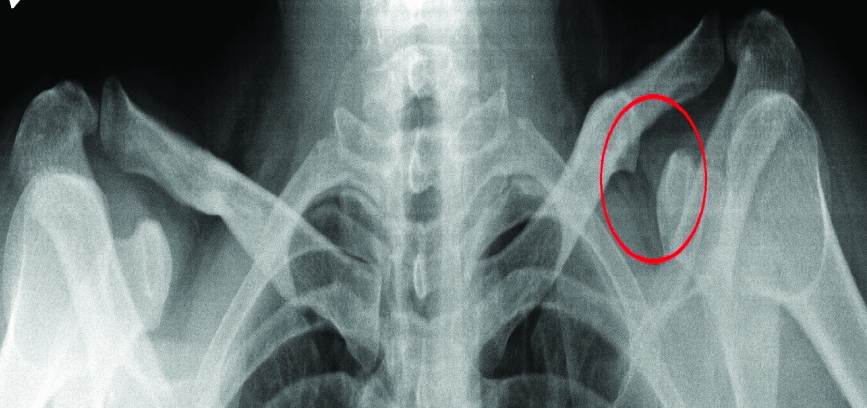
The present retrospective, observational study was carried out at King George’s Medical University, Lucknow, Uttar Pradesh, India. after obtaining ethical clearance from Institutional Ethical Committee. Soft copies of posteroanterior view of chest region, done between January 2016 to June 2016 were obtained from the data bank of Radio-diagnosis department. Total 1078 digital chest X-rays were obtained, out of which 38 films were discarded for various reasons like: 1) distorted anatomy of coracoclavicular complex due to recent or old fracture of clavicle; (2) area of interest obscured by artifact or not covered completely in view. These 1040 remaining images were independently reviewed by two authors to identify the cases with CCJ. Radiological appearance of CCJ has been described as a triangular bony out growth from under surface of clavicle with its base oriented towards the inferior surface of clavicle. The lateral border of this triangle forms an articular surface and comes in close approximation of tubercle on dorsomedial surface of coracoids process to form an articulation [13,14]. All the selected cases were discussed with a senior radiologist for confirmation.
Statistical Analysis
The prevalence of coracoclavicular joint was calculated. The cases with coracoclavicular joint were further evaluated for any association with laterality (right, left and bilateral) and gender. Chi-square for one-dimensional “goodness of fit” test and Chi-square test of independence were used to assess the association. Statistical analysis was done using Statistical Package for the Social Sciences (SPSS) version 24.0.
Results
A total of 1040 images were observed out of which 629 were of males and 411 of females. Age of the study population ranged from 8 months to 90 years. CCJ was observed in 35 cases, thus the observed prevalence was 3.37% [Table/Fig-1,2,3 and 4]. The unilateral occurrence of joint was significantly more common as compared to bilateral (p-value=0.001). Though, the CCJ was more common on left side as compared to right, the difference was statistically insignificant. While observing gender wise distribution, the joint was found to be more prevalent among males but the difference between the two was statistically insignificant [Table/Fig-5]. Gender was not found to be significantly associated with presence, laterality or sidedness of joint [Table/Fig-6]. All those individuals in whom CCJ was present were above 21 years of age.
Gender wise distribution of laterality of coracoclavicular joint.
| Gender | Present | Absent |
|---|
| Unilateral | Bilateral | Total |
|---|
| Right | Left | Total |
|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | No. | % |
|---|
| Male (n=629) | 4 | 0.64 | 13 | 2.07 | 17 | 2.70 | 5 | 0.79 | 22 | 3.50 | 607 | 96.50 |
| Female (n=411) | 6 | 1.46 | 4 | 0.97 | 10 | 2.43 | 3 | 0.73 | 13 | 3.16 | 398 | 96.84 |
| Total (n=1040) | 10 | 0.96 | 17 | 1.63 | 27 | 2.60 | 8 | 0.77 | 35 | 3.37 | 1005 | 96.63 |
Radiograph of thoracic region (PA view) of 42-year-old female showing bilateral presence of coracoclavicular joint (red encircled area).
Radiograph of thoracic region (PA view) of 40-year-old male showing bilateral presence of coracoclavicular joint (red encircled area).

Radiograph of thoracic region (PA view) of 34-year-old male showing unilateral presence of coracoclavicular joint (red encircled area).
Comparison of parameters {in cases where coracoclavicular joint was present (n=35)}.
| Parameter | Frequency | Chi-square* | p-value** |
|---|
| Number | Percentage |
|---|
| Laterality | Unilateral | 27 | 77.15 | 10.314 | 0.001 |
| Bilateral | 8 | 22.85 |
| Side | Right | 10 | 37.04 | 1.815 | 0.178 |
| Left | 17 | 62.96 |
| Gender | Male | 22 | 62.86 | 2.314 | 0.128 |
| Female | 13 | 37.14 |
[*Chi-square for a one-dimensional “goodness of fit” test is used. Calculations done at df=1
**the result is significant at p=≤0.05]
Association between gender and presence, laterality and sidedness of coracoclavicular joint.
| Parameters | Gender | Chi-square* | p-value** |
|---|
| Male | Female |
|---|
| No. | % | No. | % |
|---|
| Joint | Present | 22 | 3.50 | 13 | 3.16 | 0.086 | 0.770 |
| Absent | 607 | 96.50 | 398 | 96.84 |
| Laterality | Unilateral | 17 | 48.57 | 10 | 28.57 | 0.001 | 0.981 |
| Bilateral | 5 | 14.28 | 3 | 8.57 |
| Side | Right | 4 | 14.81 | 6 | 22.22 | 3.591 | 0.058 |
| Left | 13 | 48.15 | 4 | 14.81 |
*Chi-square test of independence was used
**the result is significant at p≤0.05
Discussion
In the present radiological study, 3.37% prevalence of joint was observed in Northern India. Majority of radiological studies done worldwide have shown 0.55%-4.3% prevalence of CCJ [1,3,15-18] except few in which extra ordinarily high prevalence (14.6%-21%) was documented [11,19]. Prevalence documented in dissection studies is highest (9.8%-28.26%) [20,21]. Osteological studies have observed it as 0.7%-16%, which is relatively higher than that reported in radiological observations [7,10,11,22-24] [Table/Fig-7].
Comparison of prevalence of CCJ in world population.
| Reference | Year | Population | Sample size | Prevalence |
|---|
| Radiological studies |
| Nutter PD [15] | 1941 | USA | 1000 | 1.2% |
| Wertheimer LG [3] | 1948 | Brazil | 277 | 0.7% |
| De Haas WHD et al., [1] | 1962 | Amsterdam | 1000132 | 1.2% (in adults)1.5% in children |
| Cockshott WP [16] | 1979 | Malaysian | - | 4.3% |
| Cockshott WP [19] | 1992 | Chinese | - | 21% |
| Nehme A et al., [17] | 2004 | French | 2192 | 0.82% |
| Olotu JE et al., [18] | 2007 | Nigerian | 1637 | 0.55% |
| Kaul N [11] | 2016 | Indian | 300 | 14.6% |
| Present study | 2016 | Indian | 1040 | 3.37% |
| Cadaveric studies |
| Lewis OJ [20] | 1959 | | 46 | 28.26% |
| Cho BP and Kang HS [21] | 1998 | Korean | 204 | 9.8% |
| Sembian U et al., [12] | 2012 | South India | 50 | 2% |
| Osteological studies |
| Ray LJ [22] | 1959 | Japanese, Australian | 584 | 9.9%0.7% |
| Kaur H and Jit I [23] | 1991 | Punjab, North India | 2000 | 10.1% |
| Nalla S and Asvat R [24] | 1995 | South African | 240 | 9.6% |
| Gumina S et al., [7] | 2002 | Italian | 1020 | 0.78% |
| Das SS et al., [10] | 2016 | Indian | 144 | 5.6% |
| Kaul N [11] | 2016 | Indian | 150 | 16% |
Kaul N also studied radiographs and Computed Tomography (CT) Scans of chest of adult humans and reported 14.6% prevalence of CCJ in Indian population which is much higher than reported by us. So much disparity in result between the two studies is probably because of the criteria taken for existence of the joint. In 4% cases only, the author has observed strongly positive indicator of CCJ, which is almost same as that reported in present study [11]. Radiological studies from Europe, USA and Africa have reported the prevalence between 0.55%-1.2% [1,3,15,18,19] whereas in a Malaysian study a higher prevalence (4.3%) was observed [16]. In present study we also reported higher occurrence suggesting CCJ, a dominant trait among Asians [19].
Osteological studies conducted in India reports 5.6-16% prevalence of CCJ [10,11,23] which is higher as compared to present study. The difference in result could be due to mode of study, as radiological study underreports the occurrence of joint as compared to osteological and dissection studies.
Differences in the prevalence of CCJ by different mode of studies can be explained explicitly. Radiological recognition of CCJ depends on the presence of bony process projecting from conoid tubercle of clavicle, approaching towards reciprocal flattened area on coracoid process of scapula, whereas in osteological studies, presence of articular facet on coracoid process and facet on conoid tubercle on inferior surface of clavicle is considered as an evidence of existence of CCJ. As the CCJ can exist even without elevation of conoid tubercle, hence such joints may be missed in radiological studies and this explains its higher prevalence in osteological studies [25]. On the other hand, in dissection studies presence of joint is recognised by articular cartilage and synovium, accounting for highest occurrence in these studies [19]. Hence, only dissection and MRI studies can truly state the prevalence of CCJ.
In present study, it was observed that unilateral occurrence of joint was significantly more common than bilateral (p<0.001). Thorough exploration of literature also suggested that unilateral occurrence of joint is more common than bilateral, however few studies reported bilateral occurrence as common one [17,18,21,24]. We noticed left side preference for CCJ, which is in consensus with available literature [24,25].
Most of the authors did not notice any statistically significant difference between genders in the occurrence of joint [17,21,23,24]. In present study also the joint was more frequently observed in males as compared to female but the difference was not statistically significant. In one study only the incidence of joint was observed substantially greater (11:1) in males [20]. In the present study we took a wide range of age to observe any correlation between presence of CCJ and age, but as in many plates age was not mentioned so we were unable to see the correlation. Infants were included in study to look for congenital presence of joint. The age of the cases, showing presence of coracoclavicular joint ranged from 21-56 years. In seven cases (out of 35) age was not mentioned. In those cases the ossification center at the sternal end of clavicle was found to be fused therefore we stated that all those individuals in whom coracoclavicular joint was present were above 21 years of age. De Hass, reported 1.5% prevalence of this joint in children up to 12 years of age but contrary to this in present study we have not observed even a single case in children [1].
Geographical variations in the prevalence of this joint have also been described. This articulation is extremely rare in Europe, but is common in Asia [19]. The results of present study further support this view. In a study based on a survey of published and unpublished anatomical, anthropological and radiological material, the global distribution of this anatomical variant was analysed and suggested that this genetically determined trait arose in Central Asia in Pleistocene times and its frequency decreases as the distance from the epicentre in China increases, and suggested using studies of the CCJ as a way of understanding patterns of migration [19].
As far as origin of joint is concerned, lots of disagreement exists in this regard. Few believe in genetic origin of this variant [17,26,27]. Some hypothesized that it is an acquired variation either due to occupational stress [6] or due to ageing [18,21]. Nehme A et al., suggested that its occurrence is probably influenced by environmental factor, while Kaur H and Jit I proposed an alternative view, suggesting that it appears after first decade of life [17,23]. Saunders SR explained it very logically as genetic trait that does not follow a simple Mendelian pattern of inheritance. He elucidated that manifestation of trait in phenotype is determined by a physiological threshold. Individuals, who surpass the threshold, manifest the trait [28].
A controversy exists as far as clinical relevance of CCJ is considered. Few believe that CCJ, an anatomic variation, seen on radiographs, is an incidental finding with very little clinical significance [29], while others believed that presence of coracoclavicular articulation limits rotation of scapula and thus predisposes to fracture of neck of humerus. Fall on outstretched hand is buffered by rotation of scapula about the thorax, but due to presence of this extra articulation buffering mechanism is not possible resulting in fracture [3]. There are few case reports of CCJ with symptoms of painful shoulder [8,27,30-32]. Presence of CCJ pulls coracoid process downwards and restricts free upward movement of acromian. This results in decrease space between acromian and supraspinatus leading to impingement of supraspinatus muscle against acromian process which due to repeated friction causes shoulder pain [27,33].
A meta-analysis of all the symptomatic cases of CCJ revealed that mean age of presentation of symptoms is 42 years with male to female ratio of 1.4:1. The most common presenting features are shoulder pain (70.58%) followed by limitation of shoulder movements associated with painful arc (29.41%), upper limb paresthesia (23.53%), brachialgia and radiation of pain to ipsilateral side (17.65%) and rarely loacalised swelling and tenderness at the site of joint or fracture of neck of humerus [25]. Osteoarthritis of coracoclavicular joint is a rare phenomenon but if present, it is hypothesized that instability of this joint over a long period results into degenerative changes. Moreover, weight lifting by ipsilateral arm exerts “weight bearing stress” on this particular joint further aggravating the situation [8]. CCJ is also a predisposing factor for the development of degenerative changes in all ‘neighbouring’ joints [7].
The present study reports that out of 1040 individuals 35 may have CCJ in Northern India which is quite high to be designated as rare. This condition is actually more common than cervical rib, whose prevalence is only 0.6% [34]. While making differential diagnosis of shoulder pain, brachialgia or upper limb paresthesia, cervical rib is a well known cause among clinical fraternity but not coracoclavicular joint, that is more prevalent. The unawareness of orthopaedic and radiologists’ community about CCJ pathology as the cause of shoulder pain has lead to gross underestimation of actual incidence of symptomatic CCJ and delayed diagnosis or inappropriate management. Therefore description of joint should be included in the text books of anatomy, radiology and orthopaedics.
Limitation
As the present observational study was done retrospectively on the data available in the Radiodiagnosis Department, therefore presence of CCJ could not be correlated with occupation or clinical history of the patient. Correlation with age was not possible because in many cases age of the patient was not mentioned.
Conclusion
Prevalence of CCJ in Northern India is 3.37%, which cannot be considered as rare and is higher than Europeans, Africans and Americans. Unilateral occurrence of joint is significantly more common than bilateral, but preference for any gender or side cannot be established. Knowledge of presence of CCJ as a cause of shoulder pain is important as it is not a rare entity and will prevent misdiagnosis and hence inappropriate treatment.
[*Chi-square for a one-dimensional “goodness of fit” test is used. Calculations done at df=1
**the result is significant at p=≤0.05]
*Chi-square test of independence was used
**the result is significant at p≤0.05