Successful Pregnancy Outcome in a Case of Muscular Dystrophy
Ganeswar Barik1, Gowri Dorairajan2, S Murali3
1 Junior Resident, Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India.
2 Professor, Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India.
3 Assistant Professor, Department of Obstetrics and Gynaecology, JIPMER, Puducherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ganeswar Barik, Junior Resident, Department of Obstetrics and Gynaecology, Gorimedu, JIPMER, Puducherry-605006, India.
E-mail: drganes86@gmail.com
Limb girdle dystrophy, Muscle weakness, Quadriparesis
A 29-year-old primigravida female was referred as a case of asymmetrical Intra Uterine Growth Restriction (IUGR) and oligohydramnious at 39 weeks and six days of gestational age with quadriparesis. She had a history of one episode of convulsion at 13 years of age followed by progressive weakness of upper limbs and then in the lower limbs. The proximal muscle weakness was greater as compared to distal muscle weakness. The patient’s movement were restricted and she had to move by sitting and pushing herself with the help of her hands since last one month [Table/Fig-1]. On examination, bulk of both the muscles was normal, power of both upper and lower limbs was 0/5 as measured by Medical Research Council (MRC) scale [1]. Plantar reflexes were withdrawn and sensory sensation was intact. Vitals were as follows: the pulse rate was 78 per minute, blood pressure was 110/70 mmHg and respiratory rate was 14 per minute. The respiratory system and cardiovascular system examination were within normal limits. On obstetrics examination, per abdomen-fundal height was around 32 weeks, with cephalic presentation. Foetal Heart Sound (FHS) was good, per vaginal-Bishop score was three and pelvis was adequate. Doppler was normal. After counselling with the patient and her husband, an attempt of vaginal delivery was made. Cervical ripening was carried out with Foley’s catheter in view of IUGR and decreased foetal movement. Post ripening, oxytocin was started; however, emergency Lower Segment Caesarean Section (LSCS) was done under general anaesthesia due to foetal distress. The caesarean and recovery from anaesthesia was uneventful. There were no complications like preterm labour, pre-eclampsia and postpartum haemorrhage.
Typical position of the patient in case of limb-girdle dystrophy.

Atrophied rectus muscle was replaced by fatty tissue which was seen during operative period and a sample of tissue was taken for biopsy. There was no improvement in the muscle weakness in the postoperative period. On investigating her serum, creatine kinase (CK-MB) value was 22, creatine kinase (CK-T) value was 306 and Lactate Dehydrogenase (LDH) value was 946. Echocardiography (ECHO) showed normal valves, chambers and normal ejection functions but her electromyography was not done.
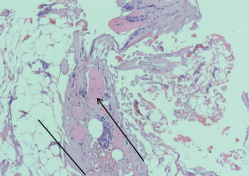
Rectus muscle biopsy showed muscle fibres replaced by adipose tissue, fascicular architecture was not maintained and few hyalinised round fibres were seen [Table/Fig-2].
Histopathology image of rectus muscle showing adipose tissue and hyalinised round fibres. Straight line= adipose tissue and arrow line= Hyalinised round fibres. (H&E 10X)
In our patient, muscle weakness had started at age of 13 years and it was progressive symmetrical weakness and proximal weakness. Her sensory system was normal. No evidence of facial, ocular, bulbar and neck muscle weakness was seen. No family history of quadriparesis. This was most probably a case of autosomal recessive variety of limb-girdle dystrophy. Differential diagnosis included Duchenne’s muscular dystrophy, Becker’s muscular dystrophy, myotonic dystrophy but Duchenne’s and Becker’s muscular dystrophy both are x-linked recessive disorders and are rare in female patients. Myotonic dystrophy presents with progressive weakness of face, which was absent in our patient, hence, it was excluded. Limb-girdle dystrophy, is an extremely rare disorder with the incidence quoted as <1/100,000 [2]. It maybe inherited in an Autosomal Recessive (AR) (90%) or dominant (10%) fashion [3]. Limb-girdle dystrophy typically manifest with weakness of pelvic and shoulder girdle muscles. Respiratory insufficiency and cardiomyopathy may occur as a result of muscles weakness. In limb-girdle muscular dystrophy muscle fibres slowly break down and are replaced by connective tissue and fat. Muscle degeneration leads to muscle weakness and atrophy. The name of the condition refers to the muscles affected, mainly those around the pelvic and shoulder girdles, also known as the limb-girdles. The clinical course of this group of muscular dystrophies is variable. Onset may be from the first to the fourth decade of life with severe forms of the disease beginning in early life and late onset disease running a milder course [4]. In our case, there were no signs and symptoms of respiratory insufficiency and cardiomyopathy. Very few case reports have mentioned about patients of limb-girdle dystrophy and pregnancy outcome [5]. One such case was reported by Ayoubi JM et al., on a case of limb-girdle dystrophy and pregnancy with vaginal delivery [6]. Another case was reported by Von Breunig F et al., where they had managed a case of limb-girdle dystrophy in pregnancy with LSCS [7]. Pregnancy in case of muscular dystrophy is rare and challenging to manage. But with multidisciplinary modality approach with a team of obstetricians, anesthesiologists, neurologists and ICU care, we can manage such cases successfully.
[1]. Medical Research Council. Aids to the examination of the peripheral nervous system, Memorandum no. 45, Her Majesty’s Stationery Office, London, 1981 [Google Scholar]
[2]. Allen T, Maguire S, Anaesthetic management of a woman with autosomal recessive limb-girdle muscular dystrophy for emergency caesarean sectionInt J Obstet Anesth 2007 16(4):370-74. [Google Scholar]
[3]. van der Kooi AJ, Barth PG, Busch HF, de Haan R, Ginjaar HB, van Essen AJ, The clinical spectrum of limb girdle muscular dystrophy. A survey in the NetherlandsBrain 1996 119:1471-80. [Google Scholar]
[4]. Ranjan RV, Ramachandran TR, Manikandan S, John R, Limb-girdle muscular dystrophy with obesity for elective cesarean section: Anesthetic management and brief review of the literatureAnesthesia, Essays and Researches 2015 9(1):127-29. [Google Scholar]
[5]. Rudnik-Schöneborn S, Glauner B, Röhrig D, Zerres K, Obstetric aspects in women with facioscapulohumeral muscular dystrophy, limb-girdle muscular dystrophy, and congenital myopathiesArch Neurol 1997 54(7):888-94. [Google Scholar]
[6]. Ayoubi JM, Meddoun M, Jouk PS, Favier M, Pons JC, Vaginal delivery in a women with limb-girdle muscular dystrophy. A case reportJ Reprod Med 2000 45(6):498-500. [Google Scholar]
[7]. von Breunig F, Goetz AE, Heckel K, Severe muscular dystrophy and pregnancy: Interdisciplinary challengeAnaesthesist 2012 61:52-55. [Google Scholar]