An Uncommon Aetiology of a Common Disease: Leptospiral Infective Endocarditis
Shikha Ranjan1, Rama Krishnan T C Ramalingam2, Chinnasamy Balasubramanian3
1 Consultant, Department of Microbiology, KG Hospital and Postgraduate Medical Institute, Coimbatore, Tamil Nadu, India.
2 Consultant, Department of Neurology, KG Hospital and Postgraduate Medical Institute, Coimbatore, Tamil Nadu, India.
3 Consultant, Department of Cardiology, KG Hospital and Postgraduate Medical Institute, Coimbatore, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shikha Ranjan, Consultant, Department of Microbiology, KG Hospital and Postgraduate Medical Institute, Coimbatore-641018, Tamil Nadu, India.
E-mail: shiksthakur@gmail.com
Leptospirosis is a neglected global disease caused by pathogenic spirochetes, 10% cases of which present as severe disease resulting in multi-system disorders. Cardiac involvement in leptospirosis is not very uncommon, but mainly manifests as electrocardiographic changes and conduction defects. However, leptospiral endocarditis is an extremely rarely reported entity. We hereby present a case of infective endocarditis caused by Leptospira in 15-year-old boy. To our knowledge, this is only the sixth case of leptospiral infective endocarditis, highlighting the fact that clinicians need to be aware of the possibility of leptospirosis, even if the illness presents with unusual features like endocarditis.
Cardiac manifestations, Duke’s criteria, Leptospirosis
Case Report
A 15-year-old boy presented to the emergency room with right-sided weakness and slurring of speech for three hours. He had a history of fever for a week prior to presentation followed by development of right ankle swelling and erythematous rash on right palm. He did not have a history of similar complaints in the past.
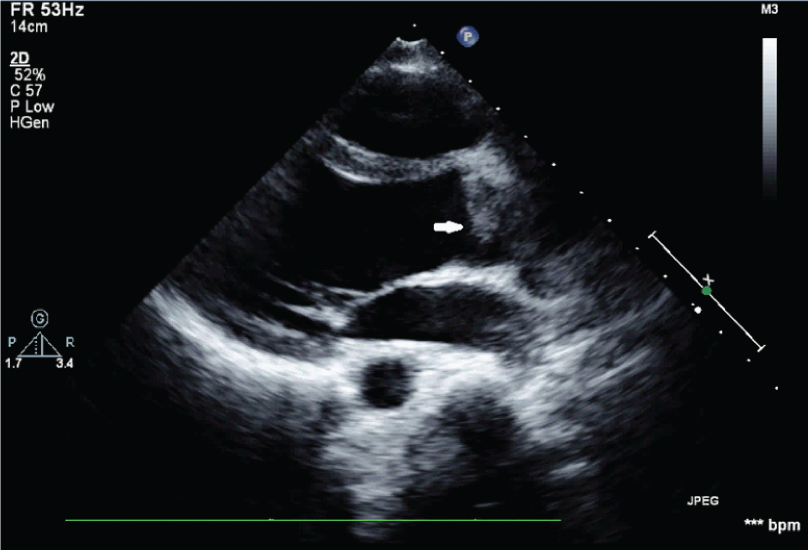
On presentation he was febrile. He had right hemiplegia with right Upper Motor Neuron (UMN) facial palsy and right sided 12th nerve palsy. Patient had marfanoid features. Patient had leucocytosis. Computerized Topography and Magnetic Resonance Imaging showed left middle cerebral artery infarct. Due to concern for infective endocarditis with infarcts an echocardiograph was obtained that showed irregular bicuspid aortic valve with vegetations measuring 0.8 cm x 0.5 cm [Table/Fig-1]. Blood culture was done in Bactec (Biomeurix) by taking paired blood culture (two blood culture bottles each time) and adding 10ml of blood in each blood culture bottle. Blood was collected from different sites like right and left hand and he was empirically started on ceftriaxone (1gram, intravenous, two times a day), vancomycin (1000 mg, iv, BD) and gentamycin (60 mg, iv, BD). The blood sample was also sent to Xcyton (commercially available Syndrome Evaluation System, which comprises of rapid multiplex amplification and accurate identification of the virulence associated genes of the causative organisms) for sepsis panel. Blood cultures as well as genetic analysis for causative organisms showed negative results. Patient’s fever (101-103°F) persisted despite broad-spectrum antibiotics (vancomycin, gentamycin, ceftriaxone) for 10 days. Laboratory investigations showed Complete blood count: Total count: 14200/mm3, HB: 12.6g/dL, Platelet: 344000/mm3, ESR: 36 mm/hour, Renal Function test: urea: 11 mg/dL, creatinine: 0.51mg/dL, hs-C-Reactive Protein: 40.5 mg/L (normal < 5 mg/ L), anti-Human Immunodeficiency Virus: Negative, Hepatitis B surface antigen: negative, anti-Hepatitis C Virus: negative. Liver function tests showed elevated level of SGOT and SGPT as 72U/L and 71U/L respectively. Echocardiogram was repeated showing an increase in size of the vegetations (2.0 cm x 0.9 cm).
Echocardiogram showing irregular bicuspid aortic valve with vegetation measuring 0.8 cm x 0.5 cm (white arrow).
At this point, tests for atypical causes of infective endocarditis including dengue, malaria and Leptospira were obtained. Malaria and dengue results were negative but his serum was positive for Leptospiral IgM antibodies by Enzyme Linked Immunosorbent Assay (ELISA). This test was repeated for confirmation as no risk factors for leptospiral infection such as rodent exposure were present in the patient. He was started on crystalline Penicillin G (CP) (4000000 units IV, quarterly) and Doxycycline (100 mg, oral, BD) for treatment of Leptospira after the second test returned positive too. Patient became afebrile within 24 hours after starting appropriate antibiotics. The patient was given antibiotics in hospital for four weeks, with improvement in right hemiplegia. His echocardiogram obtained before discharge showed reduction in vegetation size (1.2 cm x 0.4 cm). The patient was discharged following health education and hygiene instructions.
Discussion
About 90% cases of Leptospiral infection have relatively mild disease. Remaining 10% cases presents with severe leptospirosis or Weil’s disease resulting in multi-system disorder mainly involving hepatic and renal systems [1]. Humans acquire infection through contact with urine (or other body fluids, except saliva) from infected animals or contact with water, soil, or food contaminated with the urine of infected animals [2].
It also affects the pulmonary, hematopoietic, ocular, cardiovascular and central nervous system. Though under-reported and poorly understood, cardiac complications such as chest pain, arrhythmias, pulmonary edema and refractory shock have been reported in patients with severe disease [1].
Electrocardiographic (ECG) changes is a known clinical finding for cardiac manifestation in leptospirosis [3,4]. In a study, 70% of the patients out of 50 patients with serologically proven leptospirosis had ECG abnormalities, with atrial fibrilation being the commonest major arrhythmia [5]. In another study, 44% of patients with leptospirosis was reported to have atrioventricular block. A glycoprotein fraction of leptospiral cell wall, a Na-K ATPase inhibitor, has been thought to be responsible for the arrhythmia. However, our patient did not have any ECG abnormalities. Myocarditis manifesting as cardiac enzyme elevation and pericarditis are other reported cardiac abnormalities in leptospirosis [4]. Petechial hemorrhages were found in the heart and the pericardium in all the autopsy specimens, while interstitial myocarditis was found in five specimens of the total seven fatal leptospirosis cases [4].
Though cardiac enzyme elevation and ECG alterations are the common cardiac manifestations in leptospirosis, there are very few published cases in medical literature to show its association with Infective Endocarditis (IE). IE is an infection of the endocardial surface of the heart, and it indicates the presence of micro-organisms in the tissue [3]. Extensive literature search showed five cases of IE caused by Leptospira including four seropositive and one tissue proven case [Table/Fig-2]. Two factors usually lead to IE are; organism in the blood stream and an abnormal cardiac endothelium that predisposes to organism adherence and growth [3]. In our patient, the presence of marfanoid features was probably related to cardiac valvular abnormalities which consequently predisposed the patient to IE. Similar to the case reported by Ismail N et al, present case also met the Duke’s criteria of “definite endocarditis”: Echocardiographic evidence of endocardial involvement as aortic valve vegetations (major criteria), fever, marfanoid features and a positive Leptospira antibody titre (three minor criteria). On the basis of a positive serologic test for Leptospira with multiple negative blood culture results, a diagnosis of Leptospiral IE was made [3,6].
Total number of reported cases of leptospiral infective endocarditis.
| Sl. No. | Author | Year | Age (year)/Sex | Diagnostic modality | Antibiotic therapy | Outcome |
|---|
| 1. | Cornaert P et al., [7] | 1987 | NA | Microscopic agglutination test (MAT) | NA | NA |
| 2. | Benes J [8] | 2004 | 42/Male | MAT | Intravenous amoxicillin clavulanate | Survived |
| 3. | Wang LS et al., [9] | 2008 | 42/Male | Tissue biopsy and Polymerase Chain Reaction | Intravenous crystalline penicillin G | Survived |
| 4. | Radha D and Sakthivadivel V [10] | 2015 | 30/Male | MAT | Penicillin, ceftriaxone, gentamycin and metronidazole | Died |
| 5. | Ismail N et al., [3] | 2016 | 17/Female | ELISA and MAT | Intravenous crystalline penicillin G and intravenous gentamycin | Survived |
| 6. | Present case | 2017 | 15/Male | ELISA | Intravenous crystalline penicillin G and Doxycycline | Survived |
Wang LS et al., demonstrated the presence of spirochetes in surgical specimen of excised ventricular aneurysms and mitral valve of a patient with IE [9]. They suggested that direct invasion of cardiac tissue and endocardium could be the possible pathogenesis [9]. Even though the evidence of spirochetes in valvular tissue is confirmatory, the presence of valvular vegetations on imaging, negative blood cultures and positive serological test for Leptospira is sufficient for diagnosis as seen in our patient and other reported cases [10].
In the present case report, patient showed adequate clinical response to treatment with CP and doxycycline similar to prior reported cases [3,9,10]. To conclude, other uncommon causes of infective endocarditis should be evaluated in patients who have negative blood cultures and do not respond to broad spectrum antibiotic therapy.
Conclusion
This case to our knowledge will be the sixth reported case of leptospiral infective endocarditis so far. Though cardiac involvement in leptospirosis is usually manifested as ECG abnormality, it is possible to have normal ECG finding in cases of leptospiral IE. A high index of suspicion and effective collaboration between clinicians and medical microbiologists need to be maintained for prompt diagnosis and appropriate management.
[1]. Navinan MR, Rajapakse S, Cardiac involvement in leptospirosisTrans R Soc Trop Med Hyg 2012 106(9):515-20. [Google Scholar]
[2]. Centers for Disease Control and Prevention: Leptospirosis. At https://www.cdc.gov/leptospirosis/ accessed on 1.02.2017 [Google Scholar]
[3]. Ismail N, Ayub ZNS, Zueter AR, Loong NS, Yusof Z, Mohamed Z, Leptospiral Infective Endocarditis with Concurrent Dengue InfectionClin Microbiol Newsl 2016 38(4):32-34. [Google Scholar]
[4]. Bal AM, Unusual clinical manifestations of leptospirosisJ Postgrad Med 2005 51(3):179-83. [Google Scholar]
[5]. Rajiv C, Manjuran RJ, Sudhaya kumar N, Haneef M, Cardiovascular involvement in leptospirosisIndian Heart J 1996 48:691-94. [Google Scholar]
[6]. Endocarditis Diagnostic Criteria - Duke Criteria. At http://reference.medscape.com/calculator/endocarditis-diagnostic-criteria-dukeaccessed on 12.082017 [Google Scholar]
[7]. Cornaert P, Masson P, Forzy G, Graux P, Camblin J, Dutoit A, Croccel L, Infectious endocarditis caused by rare germs. Review of the literature apropos of 2 casesAnn Cardiol Angeiol 1987 36(2):87-93. [Google Scholar]
[8]. Benes J. 14th Europeon Congress on Clinical Microbiology and Infectious Diseases; 2004, abstr. 902 [Google Scholar]
[9]. Wang LS, Wang CCJ, Tsai PJ, Hsu YH, Chang BS, Su CF, Leptospire endocarditis and staphylococcus aureus bacteremia presenting with cardiac aneurysm and multiple infarcts of brain, liver, and kidneysInfect Dis Clin Pract 2008 16(1):66-68. [Google Scholar]
[10]. Radha D, Sakthivadivel V, Role of leptospirosis causing infective endocarditis - a case reportInt J Pure App Biosci 2015 3(2):218-20. [Google Scholar]